Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Gynecological Cancer in Indonesia: M. Farid AzizDocumento3 pagineGynecological Cancer in Indonesia: M. Farid AzizYosua_123Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- CVDocumento1 paginaCVDesi DamayantiNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Definisi FarmakoepidemiologiDocumento11 pagineDefinisi FarmakoepidemiologiDesi Damayanti100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Macville 1999Documento11 pagineMacville 1999Desi DamayantiNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Uji AnovaDocumento7 pagineUji AnovaDesi DamayantiNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Jgo 23 147Documento6 pagineJgo 23 147Yosua_123Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- CVDocumento1 paginaCVDesi DamayantiNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- LK PphisDocumento7 pagineLK PphisDesi DamayantiNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Kul II - HipertensiDocumento75 pagineKul II - HipertensiDesi DamayantiNessuna valutazione finora
- 2012BeersCriteria JAGSDocumento16 pagine2012BeersCriteria JAGSluxedeNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- 1.phar OwnersipDocumento12 pagine1.phar OwnersipDesi DamayantiNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Abs TactDocumento1 paginaAbs TactDesi DamayantiNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Sepsis BWDocumento22 pagineSepsis BWDesi DamayantiNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Treatment Table MalariaDocumento3 pagineTreatment Table MalariaFauziah Husnu ShofiahNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Sepsis BWDocumento22 pagineSepsis BWDesi DamayantiNessuna valutazione finora
- The Impact of Followup Telephone Calls Dudas Am J MedDocumento5 pagineThe Impact of Followup Telephone Calls Dudas Am J MedDesi DamayantiNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Treatment of TuberculosisDocumento4 pagineTreatment of TuberculosisMeta Dwi ANessuna valutazione finora
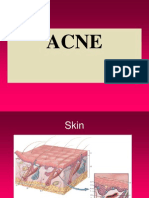
- AcneDocumento34 pagineAcneDesi DamayantiNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Temu Putih, Temulawak, MengkuduDocumento5 pagineTemu Putih, Temulawak, MengkuduDesi DamayantiNessuna valutazione finora
- Presentation 7Documento1 paginaPresentation 7Desi DamayantiNessuna valutazione finora
- Ginja LDocumento97 pagineGinja LDesi DamayantiNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- CriticalAppraisalWorksheetSys ReviewDocumento2 pagineCriticalAppraisalWorksheetSys ReviewDesi DamayantiNessuna valutazione finora
- Sediaan Modified Release Compatibility ModeDocumento36 pagineSediaan Modified Release Compatibility ModeDesi DamayantiNessuna valutazione finora
- 20Documento1 pagina20Desi DamayantiNessuna valutazione finora
- Presentation 2Documento1 paginaPresentation 2Desi DamayantiNessuna valutazione finora
- Presentation 6Documento1 paginaPresentation 6Desi DamayantiNessuna valutazione finora
- Presentation 5Documento1 paginaPresentation 5Desi DamayantiNessuna valutazione finora
- Presentation 4Documento1 paginaPresentation 4Desi DamayantiNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Presentation 3Documento1 paginaPresentation 3Desi DamayantiNessuna valutazione finora
- User Manual of Egov 11.0 Implementation of It Solution For RVNL D3799 Document Version / DetailsDocumento64 pagineUser Manual of Egov 11.0 Implementation of It Solution For RVNL D3799 Document Version / DetailsRVNLPKG6B VBL-GTLMNessuna valutazione finora
- 2-Way Doherty Amplifier With BLF888ADocumento27 pagine2-Way Doherty Amplifier With BLF888AerdemsecenNessuna valutazione finora
- Guidelines For Utility Impact Assessment For Local Roads in Developed Areas MME 2012 Cross-SectionDocumento81 pagineGuidelines For Utility Impact Assessment For Local Roads in Developed Areas MME 2012 Cross-Sectionirfan mohammedNessuna valutazione finora
- Intro Adobe Photoshop HandoutDocumento13 pagineIntro Adobe Photoshop Handoutoyindamola ayobamiNessuna valutazione finora
- Math 138 Functional Analysis Notes PDFDocumento159 pagineMath 138 Functional Analysis Notes PDFAidan HolwerdaNessuna valutazione finora
- C++ NotesDocumento11 pagineC++ NotesVedant AmonkarNessuna valutazione finora
- Tài Liệu CAT Pallet Truck NPP20NDocumento9 pagineTài Liệu CAT Pallet Truck NPP20NJONHHY NGUYEN DANGNessuna valutazione finora
- MagPi70 PDFDocumento100 pagineMagPi70 PDFDaniel TuarezNessuna valutazione finora
- Essilor MR - Blue - 20-1Documento132 pagineEssilor MR - Blue - 20-1Primoz DolinsekNessuna valutazione finora
- Tefnol 1Documento11 pagineTefnol 1Moustapha Salem MansourNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Abnormal Labour: Perceptor: Dr. Nurul Islamy, M. Kes., Sp. OGDocumento54 pagineAbnormal Labour: Perceptor: Dr. Nurul Islamy, M. Kes., Sp. OGramadhiena destia100% (1)
- KippZonen Manual Datalogger COMBILOG1022 V104 PDFDocumento173 pagineKippZonen Manual Datalogger COMBILOG1022 V104 PDFHaimeNessuna valutazione finora
- Shaft Alignment: Your Photo HereDocumento75 pagineShaft Alignment: Your Photo HereMahmoud Elghandour0% (1)
- Civil Engineering - Development Length Calculation As Per Indian CodeDocumento2 pagineCivil Engineering - Development Length Calculation As Per Indian CodeOsthePrakashNessuna valutazione finora
- TUC5+ Modbus ID Details PDFDocumento10 pagineTUC5+ Modbus ID Details PDFvijikeshNessuna valutazione finora
- Wrong Number Series 23 June by Aashish AroraDocumento53 pagineWrong Number Series 23 June by Aashish AroraSaurabh KatiyarNessuna valutazione finora
- Cantors Algebra of SetsDocumento29 pagineCantors Algebra of SetsKevs SebastianNessuna valutazione finora
- Alcatel 4029 EngDocumento31 pagineAlcatel 4029 Engafsanto2000Nessuna valutazione finora
- Degree of Kinematic IndeterminacyDocumento8 pagineDegree of Kinematic IndeterminacyshahrukhNessuna valutazione finora
- Thermal Engineering PDFDocumento5 pagineThermal Engineering PDFabhinavgiri17Nessuna valutazione finora
- Western Dragon V3 Updated PDFDocumento19 pagineWestern Dragon V3 Updated PDFMark Moldez94% (17)
- Figure of MeritDocumento33 pagineFigure of MeritmuhammadmaihadisiNessuna valutazione finora
- Translating Mathematical PhrasesDocumento16 pagineTranslating Mathematical PhrasesApple Jean Yecyec AlagNessuna valutazione finora
- Cross-Cultural Validation of The Scales For Outcomes in Parkinson's Disease-Psychosocial Questionnaire (SCOPA-PS) in Four Latin American CountriesDocumento7 pagineCross-Cultural Validation of The Scales For Outcomes in Parkinson's Disease-Psychosocial Questionnaire (SCOPA-PS) in Four Latin American Countriesfozia hayyatNessuna valutazione finora
- EagleBurgmann - API682 4th Facts, Innovations, SolutionsDocumento26 pagineEagleBurgmann - API682 4th Facts, Innovations, SolutionsTasawwur Tahir100% (1)
- A) I) Define The Term Variable Costs Variable Costs Are Costs That Change With The Quantity of Products SoldDocumento2 pagineA) I) Define The Term Variable Costs Variable Costs Are Costs That Change With The Quantity of Products SoldAleksandra LukanovskaNessuna valutazione finora
- Iohexol USP42NF37Documento5 pagineIohexol USP42NF37John Alejandro Restrepo GarciaNessuna valutazione finora
- Confidence IntervalDocumento22 pagineConfidence Intervallloyd balinsuaNessuna valutazione finora
- Silvaco ATHENA Description 1 PDFDocumento18 pagineSilvaco ATHENA Description 1 PDFRahul JaiswalNessuna valutazione finora
- DSI - MPS® Transfer System Compact Trainer I4.0 - EN - DID1089 (Screen)Documento2 pagineDSI - MPS® Transfer System Compact Trainer I4.0 - EN - DID1089 (Screen)mhafizanNessuna valutazione finora
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerDa EverandGut: the new and revised Sunday Times bestsellerValutazione: 4 su 5 stelle4/5 (393)