www.tjprc.org editor@tjprc.
org
International Journal of Economics,
Commerce and Research (IJECR)
ISSN(P): 2250-0006; ISSN(E): 2319-4472
Vol. 4, Issue 2, Apr 2014, 13-20
TJPRC Pvt. Ltd.
SOCIO ECONOMIC FACTORS RESPONSIBLE FOR CHILD IMMUNIZATION IN THREE
SAARC COUNTRIES: INDIA, BANGLADESH AND PAKISTAN
SAMRA SUBHANI
1
, SOFIA ANWAR
2
& G. M. SUBHANI
3
1
Lecturer, Department of Economics, Government College University, Faisalabad, Pakistan
2
Associate Professor, Department of Economics, Government College University, Faisalabad, Pakistan
3
Associate Professor, Punjab Medical College, Faisalabad, Pakistan
ABSTRACT
It was a comparative study based on the socioeconomic factors that were affecting the participation in the child
immunization program. This study was conducted at the Department of Economics GC University Faisalabad from
February 2012 to September 2013.To see the effect of socioeconomic factors on child immunization in Pakistan, India and
Bangladesh. Data was collectected from DHS (Demographic and Health Survey) from year 2006-2007.
Following variables were studied: 1.Mothers education 2.Fathers education 3.Mothers employment 4.Living standard 5.
Residential Area Variables were categorized accordingly. Children vaccinated up to the age of 5-years were included while
the older were excluded from the study. Multi logistic model was applied to see the significance of these variables on child
immunization. Immunization was better in the children of employed mothers in all selected countries. Uneducated mothers
had less likelihood to immunize their children compared to highly educated mothers. Uneducated fathers had less
likelihood to immunize their children in all selected countries. Poor people residing in villages had less probability to
immunize their children as compared to the rich persons residing in the cities. Education of parents, Mothers employment,
Richest and people living in urban area were the factors which were significantly different from uneducated parents,
unemployed mothers, poorest and people living in rural areas. These factors should be improved considerably for making
planning to achieve optimum results of successful immunization.
KEYWORDS: Immunization, Vaccination, Education, Children, Unemployment, Socio-Economic Factors, SAARC
Countries
INTRODUCTION
Economical crises is prevailing universally creating hurdles in the development of the countries. Development is a
constant rise in the GDP of a country for a long period of time (Todero, 2011). Human capital is the most important factor,
influencing development. Human capital is mainly influenced by two factors education and health (Akram and
Faheem, 2007; Idrees, 2010).
Education is the key factor of development. But a person cannot be educated well without a healthy body and
mind. At the same time a diseased person cannot be able to perform his duties properly. People all over the world are
looking for different factors effecting economy of their countries. Beside other factors, good health of people is one of the
key factors in improving the human capital (Idrees, 2010). Physically unhealthy people cannot perform their role in the
uplifting of the economy of their nation and increasing incidence of ailing people becomes cause of deficient budget
availabile for other progressive and productive projects. Good physical health can be achieved by elimination of different
14 Samra Subhani, Sofia Anwar & G. M. Subhani
Impact Factor (JCC): 4.2234 Index Copernicus Value (ICV): 3.0
diseases at proper time. Different diseases are eradicated or kept under maximum control by two ways, i prevention of
disease before its occurrence ie. treatment after its occurrence. Prevention is easy and needs minimal financial expenditures
while treatment of dieses is painful, costly and time consuming process involving a lot of manpower, equipment, medicine
and different surgical procedures. There are different preventive methods for different diseases (Hong and Banta, 2005).
Besides other, Immunization is one of the most effective and well recognized methods in this context. Human
body possesses an immune system which protect it from different diseases by developing antibodies against the causative
organisms. One is natural innate immunity which is present by birth and other is acquired which is created afterwards by
giving specific attenuated organisms to a person by giving a vaccine. Immunity for different diseases can be achieved in
children as well as in adults. The method to create resistance against disease is called as immunization
(Guyton and Hall, 2000).Child of today is the adult of tomorrow. Child Immunization is the main focus for preventing the
human beings from certain disease all over the world in the form of Expanded Programme of Immunization (EPI). EPI is
implemented by WHO in all countries for eradication and control of certain diseases. The vaccines include Beccillis
Calmatte Guerin (BCG), Oral Polio Vaccine (OPV), Dephtheria Pertusis Tatanus (DPT), Measles Mumps Rubella (MMR)
(Mangrio et al., 2008).
Millennium Development Goals were formulated in 1990 and it was aimed to achieve these goals in 2015. Due to
the importance of immunization in health sector the 5
th
Millennium Development Goal was to improve immunization in
the society. Improved immunization is very helpful in decreasing the child mortality. It requires 12 months for the
completion of immunization in children. It protects the body against fatal diseases such as tuberculosis, malaria, whooping
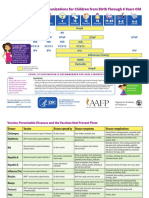
cough, typhoid, diarrhea etc, (Easterly, 2009). Schedule of child immunization is shown in table 1.
Table 1: The Schedule of Child Immunization
Recipient Age Vaccine
Infants
Birth
Six weeks
10 weeks
14 weeks
9 months
14 months
BCG/OPV
DPT/OPV
Measles
vaccine
DPT/OPV
Children
5 years
10 years
16 years
DT vaccine
Tetanus
(Source: WHO India 2007)
The main cause of infant mortality in the world is the Vaccine Preventable Diseases (VPD) such as diarrhea,
tuberculosis, whooping cough, Pneumonia etc. Pakistan is considered a country where Infant Mortality Rate (IMR) is very
high among the Asian countries. In 2006 and 2007 it was about 78 and 94 per 1000 births respectively (Pildat, 2010).
In Pakistan 120 children die before reaching the five years of their age due to the less access to vaccination. In addition
40% children in Pakistan are not able to get essential food for their health that is a big dilemma as well (Yasin et al., 2004).
Pakistan, India and Bangladesh are situated in the same geographic region having same environment. Pakistan is
not able to eradicate Polio from the country inspite of high availability of medicines in the country due to ineffective
immunization programme (Hensy et al., 2000). Similarly situation in Bangladesh is not different. Comparatively EPI was
introduced in Bangladesh in 1979 and started its full activities in 1985. The situation of vaccination in Bangladesh is better
Socio Economic Factors Responsible for Child Immunization in: 15
Three SAARC Countries India, Bangladesh and Pakistan
www.tjprc.org editor@tjprc.org
than Pakistan but not optimal standards. In 1984 the coverage was less than 10 % but in 1994 it was about 70%. It was a
big improvement for Bangladesh in 10 years (Chowdhary et al., 2002).
In India, the situation of immunization is better but it still does not have attained the optimum results of successful
immunization according to the EPI (Extended Program on Immunization) which was started in 1978. An important
predictor of effective immunization in a child is its timely initiation i e soon after birth 12 (Patra, 2004). Contrarily the
mothers education has an inverse relationship with child immunization. Less educated mothers are more interested in
child immunization than the highly educated mothers (Muula, et al. 2009).
Pakistan, India and Bangladesh are the countries which are implementing the immunization program EPI.
Regional disperities are more common among people residing in cities. They are showing more sophisticated behavior and
take their children to the vaccination centers while the people in villages are less conscious about the immunization
program (Chaudary, et al 2002). The success results of such vaccination programs in this region are not as good as are in
developing countries due to noncompliance of the people. There are different factors which are responsible for then on
compliance. These factors include living standards, mothers education, fathers education, mothers employment and
residential area (rural/urban). By knowing the impact of the above factors on the success of immunization, significant
improvements can be made. This will result in proper planning to enhance human capital, the economical development
status of a country and general prosperity of the nation.
Objectives: To see the effect of socioeconomic factors on child immunization in three selected countries
Pakistan, India and Bangladesh.
MATERIALS AND METHODS
This study was conducted at the Department of Economics, G. C. University Faisalabad Pakistan from
February 2012 to September 2013. It is a comparative study. Demographic and Health Survey of India, Pakistan and
Bangladesh have collected data about the different variables all over the countries. Data from the above survey regarding
immunization of children up to 5 years of age, who were eligible for immunization, was included in the study. Children
above the age of 5 years who were not eligible for immunization were excluded from the study. Data summary is given
table 2.
Table 2: Data Summary Showing Name of the Country, Duration of Data Collection and Sample Size
Country Year Sample
Pakistan 2006-2007 95441
India 2005-2006 109041
Bangladesh 2007 10400
Child immunization was taken as the dependent variable. It was further divided into three categories (1) not
immunized (2) partially immunized (3) fully immunized. This variable is constructed by taking the following
injections/vaccines into considerations: (1) BCG,(2) Polio1 (3) DPT2, (4) Polio2, (5) DPT3, (6) Polio 3, (7) MMR,
(8) Polio 0, (9) HBV1, (10) HBV 2 and (11) HBV3.
Mothers education is the independent variable and it has four categories (0) not educated (1) primary education
(2) secondary education (3) higher education and fathers education is also categorized as the mothers education. Mothers
16 Samra Subhani, Sofia Anwar & G. M. Subhani
Impact Factor (JCC): 4.2234 Index Copernicus Value (ICV): 3.0
employment is divided into two categories, (0) is unemployed and (1)is employed. To check the effect of the living
standard wealth index is taken which is divided into five categories (1) poorest (2) poor (3) middle (4) rich and (5) richest.
Area business can be seen by taking the variable of a residential area that is divided into two categories (1) rural (2) urban
Analytical Framework
In this study our predicted model is in three categories so multi logistic model is applied here. The basic equation
is given below-
( , ) , ( , )
1
P r ( , )
l n ( )
P r ( )
J
a b i a b a b j i j
j
Y a b
Y Z
Y c
=
=
= = +
=
=+
1
(LS) +
2
(MEd) +
3
(FED) +
4
(ME) +
5
(RA)
Here is a constant and is a slope co-efficient of the variables that is to be estimated. P/1-p shows the odd ratio
to explain the predictor variable. The variables are interpreted on the basis of their significance level. Odd ratios explain
the variables on the basis of child immunization.
RESULTS AND DISCUSSIONS
Frequency distribution was given below according to the variables. In Pakistan poorest persons were highest in
number while in India and Bangladesh the richest persons were highest in number. The ratio of uneducated parents were
highest in Pakistan
Table 3: Variable Distribution in Three Selected Countries
Description Category
Pakistan India Bangladesh
No Percentage No Percentage No Percentage
Family
Income
Poorest 1915 22.7 1144 19.8 1144 19.8
Poor 1800 21.3 1196 20.7 1196 20.7
Middle 1717 20.3 1078 18.6 1078 18.6
Rich 1568 18.6 1081 18.7 1081 18.7
Richest 1446 17.1 1289 22.3 1289 22.3
Mothers
education
No education 5642 66.8 1552 26.8 1552 26.8
Primary 1168 13.8 1810 31.3 1810 31.3
Secondary 1115 13.2 1985 34.3 1985 34.3
Higher 521 6.2 441 7.6 441 7.6
Fathers
Education
No education 3101 36.7 1942 33.6 1942 33.6
Primary 1375 16.3 1633 28.2 1633 28.2
Secondary 2615 31 1502 26 1502 26
Higher 1342 15.9 711 12.3 711 12.3
Mothers
Employment
Employed 6511 77.1 13996 28.8 4403 76.1
Not employed 1935 22.9 34675 71.2 1384 23.9
Area
Rural 5509 65.2 30053 61.7 3784 65.4
Urban 2937 34.8 18618 38.3 2004 34.6
Frequency distribution of three selected countries explained the percentages of people according to the
socioeconomic factors. Poorest persons were more in Pakistan while in India and Bangladesh they were comparatively
less. The percentage of richest person was also highest in Pakistan. This percentage showed more income inequality in
Pakistan. Illiteracy rate in Pakistan was also found to be highest. Females were more empowered in Pakistan due to high
percentage of employed mothers. The percentage of people living in villages was almost same in all three countries.
Socio Economic Factors Responsible for Child Immunization in: 17
Three SAARC Countries India, Bangladesh and Pakistan
www.tjprc.org editor@tjprc.org
Table 4: Results for Partial Immunization in Three Selected SAARC Countries
Dependent
Variable
Coefficient Sig Odd Ratio Coefficient Sig Odd Ratio Coefficient Sig Odd Ratio
Constant 3.973 .000
3.895 .000
87.572 000
Mothers Employment
MW0 -.410 .000 0.664 -.186 .000 .830 -.534 .000 .587
MW1 0
0
0
Mothers Education
MED0 -.972 .002 .378 -1.072 .000 .342 -.616 .098 0.587
MED1 -.443 .183 0.642 -.983 .000 .374 -.165 .651 .848
MED2 -.351 .291 .704 -.732 .000 .481 .048 .889 1.049
MED3 0
0
0
Fathers Education
FED0 -.076 .795 .965 -.545 0 .580 -.274 .347 .760
FED1 .247 .111 1.280 -.507 0 .603 -.241 .398 .786
FED2 .207 .140 1.230 -.147 .132 .863 -.104 .706 .902
FED3 0
0
0
Living Standard
LS 1 -.985 .000 .373 -1.130 .000 .323 -.020 .928 .980
LS2 -.797 .000 .451 -1.107 .000 .331 .008 .971 1.008
LS3 -.925 .000 .396 -.822 .000 .439 -.001 .995 .999
LS4 -.562 .003 .570 -.521 .000 .594 -.015 .943 .985
LS5 0
0
0
Residential Area
RA 0 -.270 .007 .763 -.046 .306 .955 -.022 .871 .978
RA 1 0
0
0
Results of Multi logistic model explained that the women who were less empowered had less attention towards
participation in partial child immunization, the probabilities in three countries was 0.664, 0.830 and 0.587. Nath et al
(2007) have showed the same results that the employed mothers were more conscious to immunize their children compared
to the unemployed mothers. 14 Illiterate mothers due to less knowledge had less attention towards immunization.
Their probabilities were 0.378, 0.342 and 0.540 respectively. Singh et al (2012) observed that uneducated low standard
women were reluctant to immunize their children. 15.Ibn of et al (2007) found the significant relationship between
mothers education and child immunization 16.Yasin et al (2004), Adem et al (2003) and Biswas et al (2001) had the same
positive impact as this study had revealed 9,17,18.
Similarly illiterate fathers were also not interested in partial immunization of their children. Low standard poorest
persons also showed less attention towards participation in partial child immunization. Their probabilities were 0.373,
0.323 and 0.980.Bandhari et al (2007) explained that the rich people had more chances to immunize their children as
compared to the poor people 18.
The results of Babalola (2008) were similar to this study as they showed significant relationship with Parents
income and child immunization. Rural residents had less chances to avail the opportunity of partial immunization of
children 20. Comparatively the study by Antai et al (2010) revealed different results, the children living in rural areas had
more chances to get immunization as compared to the children living in urban areas 21.
Table 5: Results for Fully Immunized Children in Three Selected Countries
Pakistan India Bangladesh
Variable Coefficient Sig Odd Ratio Coefficient Sig Odd Ratio Coefficient Sig Odd Ratio
Constant 3.802 .000 1.106 .002 12.222 .000
Mothers Employment
MW0 -.346 .001 .707 -.284 .000 .753 -.399 .074 .671
18 Samra Subhani, Sofia Anwar & G. M. Subhani
Impact Factor (JCC): 4.2234 Index Copernicus Value (ICV): 3.0
Table 5: Contd.,
MW1 0 0 0
Mothers Education
MED0 -1.505 .000 .222 -2.085 .000 .124 -1.586 .001 .205
MED1 -.844 .012 .430 -1.361 .000 .256 -1.020 .024 .361
MED2 -.627 .061 .534 -.864 .000 .422 -.284 .468 .753
MED3 0 0 0
Fathers Education
FED0 -.237 .112 .789 -.357 .003 .700 -.932 .022 .394
FED1 .125 .453 1.133 -.142 .235 .868 -.780 .035 .458
FED2 .206 .162 1.229 .031 .766 1.032 -.587 .076 .556
FED3 0 .152 1.263 0 0
Living Standard
LS 1 -1.902 .000 .149 -2.222 .000 .108 -.557 .150 .573
LS2 -1.321 .000 .267 -1.919 .000 .166 -.542 .125 .581
LS3 -1.152 .000 .316 -1.178 .000 .147 -.428 .187 .652
LS4 -.575 .003 .563 -.893 .000 .432 -.461 .112 .631
LS5 0 0 0
Residential Area
RA 0 -.218 .043 .804 -.003 .341 .957 -.410 .052 .664
RA 1 0 0 0
Women who were not empowered had less chances to fully immunize their children as compared to the
empowered women who had the opportunity to go out and work for the benefit of their family. Illiterate mothers had also
less attention towards full immunization of their children. Patra (2006) similarly found that the mothers education had
positive impact on child immunization 12. Different studies by Ibn of et al (2007), Jamil et al 1999, Pearce et al 2007,
Yadav (2004) had observed the same results 16,22,23,24. Uneducated fathers showed the same attitude and give less
attention towards full immunization of their children.
Poorest persons were low standard people and they gave less attention towards immunization because they did not
consider it important. Chaudhary et al (2002) found that the poor parents were less likely to immunize their children as
compared to the richest person of the society 11. Tinkew and Gordon (2005) had shown the same results. People living in
villages had less access to child immunization programme 25.
SUGGESTIONS
It is suggested that literacy rate should be improved in all segments of the society without gender biased at all age
levels.
Education level should be elevated in people living in urban as well as rural areas. Gender discrimination should
be removed. Boys and girls should have equal rights to get education and health facilities.
Maximum employment opportunities should be given to the people at large scale without sex discrimination to
raise their standards of living.
Immunization system should be improved in rural areas. So the backward people can also get easy access to the
immunization programmes.
Government should also add the subject of health at primary level and there should be a chapter of immunization,
social and health awareness. Seminars should be conducted on this topic in education institutions, health institutions and
different community centers. Health workers and social workers should go door to door to motivate the people in this
regard.
Socio Economic Factors Responsible for Child Immunization in: 19
Three SAARC Countries India, Bangladesh and Pakistan
www.tjprc.org editor@tjprc.org
Awareness campaigns should be launched at every level by the Government as well as Non government
organizations to highlight the importance of child Immunization.
REFERENCES
1. Adem A, Tacettin I, Sevin A and Vildan E (2003). Diphtheria immunization rates and the effect of several socio
demographic factors on immunization of children in eastern Turkey. Pediatrics international, 45: 461-466.
2. Akram M and Khan FJ (2007). Health care services and government spending in Pakistan. PIDE working papers
32: 1-31.
3. Antai D (2009). Inequitable childhood immunization uptake in Nigeria: a multilevel analysis of individual and
contextual determinants. BMC Infectious Diseases, 9:181. Biswas CS, Darda AM and Alam FM (2001).
The Pakistan development review. Factors affecting Childhood immunization in Bangladesh. 40 (1): 57-70
4. Bhandari P, Shrestha SS and Ghimire DJ (2007). Socio cultural and geographical disparities in child
immunization in Nepal. Asia Pacific Population Journal, 22(1) 43-64.
5. Babalola S (2008). Determinants of the uptake of the full dose of diphtheria-pertusis-tetanus vaccines (DPT3) in
Northern Nigeria: a multilevel analysis. Maternal child Health J, DOI 10.1007/s10995-008-0386-5, 13(4):550-8.
6. Chowdhury AMR, Bhuiya A, Mahmad S, Abdus Salam AKM and Karim F (2002). Who gets vaccinated in
Bangladesh? The immunization divide. Bangladesh Health Equity Watch Equity Watch Paper No.1: 5-27.
7. Easterly W (2009). How the millennium development goals are unfair to Afrca. World development 37 (1): 26-35.
8. Gyton MD, John EH (2007). A Textbook of Medical Physiology 11
th
Edition Publisher: Saunders; pp 405.
9. Hennesy AK, Marx A, Hafiz R, Asghar H, Hadler CS, Jafri H and Suttar WR (2000). The Journal of infectious
diseases. Widespread paralytic poliomyelitis in Pakistan: A case control study to determine risk factors and
implications for Poliomylitis eradication 182 (1) 6-11.
10. Hong R and Banta JE (2005). Effects of extra immunization efforts n routine immunization at district level in
Pakistan. Eastern Mediterranean Health Journal, 11(4) 745-52.
11. Idrees H (2010). Factors determine the infant mortality in Punjab. LUND UNIVERSITY, School of Economics
and Management 14-18.
12. Ibnouf AH, Borne VD and Jam M (2007). Factors influencing immunization coverage among children under five
years of age in Khartoum State, Sudan. SA Fam Pract, 49(8): 14.
13. Jamil K, Bhuyia A, Strearfield K and Chakarbharti A (1999). Journal of health policy and planning.
The immunization Programme in Bangladesh: impressive gains in coverage but gaps reemains. 14 (1):49-58.
14. Mangrio NK, Alam MM and Sheikh BT (2008). Is expanded programme on immunization doing enough? View
point of health workers and mangers in Sindh, Pakistan. J Pak Med Association, 58(2): 64-67.
20 Samra Subhani, Sofia Anwar & G. M. Subhani
Impact Factor (JCC): 4.2234 Index Copernicus Value (ICV): 3.0
15. Muula AS, Polyearpe MY, Job J, Siziya S, and Rudatikira E (2009). Association between maternal use of
traditional health services and child vaccination coverage in Pont-Sonde, Haiti. International Journal for Equity in
Health, 8:1.
16. Nath B, Singh JV, Awasthi S, Bhushan V, Kumar V and Singh SK (2007). A study on determinants of
immunization coverage among 12-23 months old children in urban slums of Luckhnow district India. Indian
J Med sci, 61(11): 598-606.
17. Pildat (2010). Immunization in Pakistan. PILDAT (Pakistan Institute of Legislative Development and
Transparency) 37: 11-12.
18. Patra N (2006). Universal immunization programme in India: The determinants of childhood immunization.
Dehli School of Economics pp 1-41.
19. Pearce A, Law C, Elliman D, Cole TJ and Bedford H (2008). Factors associated with uptake of measles, mumps
and rubella vaccine (MMR) and use of single antigen vaccines in a contemporary UK cohort: prospective cohort
study BMJ 336 (7647): 754-7.
20. Singh B, Singh A, Singh N (2012) European Journal of Scientific research Determinants of Immunization in
Bosmotwe District of Ashanti Region, Ghana. 77 (1): 77-94.
21. Todero MP and Smith SC (2011). Economic Development 11
th
edition pp 7-9
22. Tinkew JB and Dejong GF (2005). Do household structure and household economic resources predict childhood
immunization? Evidence from Jamaica and Trinidad and Tobago. Population Research and Policy Review,
24: 27-57.
23. Yadav K, Rai SK, Vidushi A, Pandav CS (2009). Intensified pulse Polio immunization: Time spent and cost
incurred at primary healthcare centre. Natl Med J India 22 (1) 13.
24. Yasin G, Qureshi AI, Aslam M and Naz S (2004). Socio-economic factors affecting the trend towards vaccination
of mother and infants in Multan. Journal of Research (Science), Bahauddin Zakariya University, Multan, Pakistan,
15(1): 107-112.
Potrebbero piacerti anche
- Flame Retardant Textiles For Electric Arc Flash Hazards: A ReviewDocumento18 pagineFlame Retardant Textiles For Electric Arc Flash Hazards: A ReviewTJPRC PublicationsNessuna valutazione finora
- Comparative Study of Original Paithani & Duplicate Paithani: Shubha MahajanDocumento8 pagineComparative Study of Original Paithani & Duplicate Paithani: Shubha MahajanTJPRC PublicationsNessuna valutazione finora
- 2 29 1645708157 2ijtftjun20222Documento8 pagine2 29 1645708157 2ijtftjun20222TJPRC PublicationsNessuna valutazione finora
- 2 33 1641272961 1ijsmmrdjun20221Documento16 pagine2 33 1641272961 1ijsmmrdjun20221TJPRC PublicationsNessuna valutazione finora
- 2 51 1656420123 1ijmpsdec20221Documento4 pagine2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNessuna valutazione finora
- 2 52 1649841354 2ijpslirjun20222Documento12 pagine2 52 1649841354 2ijpslirjun20222TJPRC PublicationsNessuna valutazione finora
- 2 31 1648794068 1ijpptjun20221Documento8 pagine2 31 1648794068 1ijpptjun20221TJPRC PublicationsNessuna valutazione finora
- Baluchari As The Cultural Icon of West Bengal: Reminding The Glorious Heritage of IndiaDocumento14 pagineBaluchari As The Cultural Icon of West Bengal: Reminding The Glorious Heritage of IndiaTJPRC PublicationsNessuna valutazione finora
- Development and Assessment of Appropriate Safety Playground Apparel For School Age Children in Rivers StateDocumento10 pagineDevelopment and Assessment of Appropriate Safety Playground Apparel For School Age Children in Rivers StateTJPRC PublicationsNessuna valutazione finora
- 2 4 1644229496 Ijrrdjun20221Documento10 pagine2 4 1644229496 Ijrrdjun20221TJPRC PublicationsNessuna valutazione finora
- Using Nanoclay To Manufacture Engineered Wood Products-A ReviewDocumento14 pagineUsing Nanoclay To Manufacture Engineered Wood Products-A ReviewTJPRC PublicationsNessuna valutazione finora
- 2 51 1651909513 9ijmpsjun202209Documento8 pagine2 51 1651909513 9ijmpsjun202209TJPRC PublicationsNessuna valutazione finora
- The Conundrum of India-China Relationship During Modi - Xi Jinping EraDocumento8 pagineThe Conundrum of India-China Relationship During Modi - Xi Jinping EraTJPRC PublicationsNessuna valutazione finora
- 2 44 1653632649 1ijprjun20221Documento20 pagine2 44 1653632649 1ijprjun20221TJPRC PublicationsNessuna valutazione finora
- 2 52 1642055366 1ijpslirjun20221Documento4 pagine2 52 1642055366 1ijpslirjun20221TJPRC PublicationsNessuna valutazione finora
- Dr. Gollavilli Sirisha, Dr. M. Rajani Cartor & Dr. V. Venkata RamaiahDocumento12 pagineDr. Gollavilli Sirisha, Dr. M. Rajani Cartor & Dr. V. Venkata RamaiahTJPRC PublicationsNessuna valutazione finora
- 2 51 1647598330 5ijmpsjun202205Documento10 pagine2 51 1647598330 5ijmpsjun202205TJPRC PublicationsNessuna valutazione finora
- Covid-19: The Indian Healthcare Perspective: Meghna Mishra, Dr. Mamta Bansal & Mandeep NarangDocumento8 pagineCovid-19: The Indian Healthcare Perspective: Meghna Mishra, Dr. Mamta Bansal & Mandeep NarangTJPRC PublicationsNessuna valutazione finora
- An Observational Study On-Management of Anemia in CKD Using Erythropoietin AlphaDocumento10 pagineAn Observational Study On-Management of Anemia in CKD Using Erythropoietin AlphaTJPRC PublicationsNessuna valutazione finora
- Vitamin D & Osteocalcin Levels in Children With Type 1 DM in Thi - Qar Province South of Iraq 2019Documento16 pagineVitamin D & Osteocalcin Levels in Children With Type 1 DM in Thi - Qar Province South of Iraq 2019TJPRC PublicationsNessuna valutazione finora
- A Review of "Swarna Tantram"-A Textbook On Alchemy (Lohavedha)Documento8 pagineA Review of "Swarna Tantram"-A Textbook On Alchemy (Lohavedha)TJPRC PublicationsNessuna valutazione finora
- Self-Medication Prevalence and Related Factors Among Baccalaureate Nursing StudentsDocumento8 pagineSelf-Medication Prevalence and Related Factors Among Baccalaureate Nursing StudentsTJPRC PublicationsNessuna valutazione finora
- Effect of Degassing Pressure Casting On Hardness, Density and Tear Strength of Silicone Rubber RTV 497 and RTV 00A With 30% Talc ReinforcementDocumento8 pagineEffect of Degassing Pressure Casting On Hardness, Density and Tear Strength of Silicone Rubber RTV 497 and RTV 00A With 30% Talc ReinforcementTJPRC PublicationsNessuna valutazione finora
- Effectiveness of Reflexology On Post-Operative Outcomes Among Patients Undergoing Cardiac Surgery: A Systematic ReviewDocumento14 pagineEffectiveness of Reflexology On Post-Operative Outcomes Among Patients Undergoing Cardiac Surgery: A Systematic ReviewTJPRC PublicationsNessuna valutazione finora
- 2 67 1645871199 9ijmperdfeb202209Documento8 pagine2 67 1645871199 9ijmperdfeb202209TJPRC PublicationsNessuna valutazione finora
- 2 67 1648211383 1ijmperdapr202201Documento8 pagine2 67 1648211383 1ijmperdapr202201TJPRC PublicationsNessuna valutazione finora
- Analysis of Bolted-Flange Joint Using Finite Element MethodDocumento12 pagineAnalysis of Bolted-Flange Joint Using Finite Element MethodTJPRC PublicationsNessuna valutazione finora
- 2 67 1653022679 1ijmperdjun202201Documento12 pagine2 67 1653022679 1ijmperdjun202201TJPRC PublicationsNessuna valutazione finora
- Numerical Analysis of Intricate Aluminium Tube Al6061T4 Thickness Variation at Different Friction Coefficient and Internal Pressures During BendingDocumento18 pagineNumerical Analysis of Intricate Aluminium Tube Al6061T4 Thickness Variation at Different Friction Coefficient and Internal Pressures During BendingTJPRC PublicationsNessuna valutazione finora
- 2 67 1645017386 8ijmperdfeb202208Documento6 pagine2 67 1645017386 8ijmperdfeb202208TJPRC PublicationsNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- D.S.S AIIMS PREPRATION TEST SERIES MODEL PAPER - 8 SMALLPOX AND CHICKENPOXDocumento8 pagineD.S.S AIIMS PREPRATION TEST SERIES MODEL PAPER - 8 SMALLPOX AND CHICKENPOXDr-Sanjay SinghaniaNessuna valutazione finora
- Providing Immunizations for ChildrenDocumento72 pagineProviding Immunizations for ChildrenChiyo Natha100% (1)
- Expanded Program On Immunization Philippines)Documento8 pagineExpanded Program On Immunization Philippines)Mark AcuzarNessuna valutazione finora
- Gas Gangrene: DR Mohammed Akbar KhanDocumento89 pagineGas Gangrene: DR Mohammed Akbar KhanAkbar KhanNessuna valutazione finora
- Vaccine Project - FinalDocumento2 pagineVaccine Project - Finalchelsea garzaNessuna valutazione finora
- Aluminum Toxicity in Mitochondrial Dysfunction and ASDDocumento8 pagineAluminum Toxicity in Mitochondrial Dysfunction and ASDDr. Amy Yasko100% (6)
- Baseline Survey On Child and Related Maternal Health Care-Revised Report - Rajasthan-494 - 1Documento123 pagineBaseline Survey On Child and Related Maternal Health Care-Revised Report - Rajasthan-494 - 1National Child Health Resource Centre (NCHRC)Nessuna valutazione finora
- Immunization and PregnancyDocumento1 paginaImmunization and PregnancySANANessuna valutazione finora
- Handbook for Vaccine & Cold Chain HandlersDocumento112 pagineHandbook for Vaccine & Cold Chain HandlersasmintehminaNessuna valutazione finora
- Vaccine Information For 11-Year-Old StudentsDocumento1 paginaVaccine Information For 11-Year-Old StudentsAnonymous gH0Y8V0Nessuna valutazione finora
- Over-All Goal: To Reduce The Morbidity and Mortality Among Children Against The Most Common Vaccine-Preventable Specific GoalDocumento9 pagineOver-All Goal: To Reduce The Morbidity and Mortality Among Children Against The Most Common Vaccine-Preventable Specific GoalRetiza EllaNessuna valutazione finora
- Paediatric Protocols 3rd Edition 2012.Documento693 paginePaediatric Protocols 3rd Edition 2012.Sumita Muniandy67% (3)
- Community Health Nursing Exam 145 Questions The Filipino Nurse PDFDocumento49 pagineCommunity Health Nursing Exam 145 Questions The Filipino Nurse PDFapremsNessuna valutazione finora
- Community Health Nursing Exam 1 Practice & Text ModeDocumento33 pagineCommunity Health Nursing Exam 1 Practice & Text ModeAngelica SorianoNessuna valutazione finora
- Osce QuestionsDocumento128 pagineOsce Questionsdean100% (1)
- Article Review: Protecting Infants Against PertussisDocumento2 pagineArticle Review: Protecting Infants Against PertussisMadiNessuna valutazione finora
- Infanrix Hexa RSMKL July 2023Documento37 pagineInfanrix Hexa RSMKL July 2023Bayu KurniawanNessuna valutazione finora
- Notes FileDocumento78 pagineNotes FileSEIYADU IBRAHIM K100% (1)
- Immunization UipDocumento20 pagineImmunization Uipdevesh gargNessuna valutazione finora
- DOH Programs Related To Family HealthDocumento6 pagineDOH Programs Related To Family HealthJADE MAIKHA A. MIERGASNessuna valutazione finora
- Diphtheria and Tetanus Toxoids AdsorbedDocumento20 pagineDiphtheria and Tetanus Toxoids AdsorbedShaffy UngaNessuna valutazione finora
- Important Questions For CBSE Class 9 Science Chapter 13Documento13 pagineImportant Questions For CBSE Class 9 Science Chapter 13Ankita GuptaNessuna valutazione finora
- Parent Ver SCH 0 6yrsDocumento2 pagineParent Ver SCH 0 6yrsSrinivasamurthy KamarthiNessuna valutazione finora
- Informative Essay On My CareerDocumento5 pagineInformative Essay On My Careerapi-241280029Nessuna valutazione finora
- Set 2 Post Test CA3 EPI IMCI Mother and Child With AnswerDocumento15 pagineSet 2 Post Test CA3 EPI IMCI Mother and Child With AnswerScarlet GrayNessuna valutazione finora
- Document From DR Abhay ShahDocumento20 pagineDocument From DR Abhay ShahRavikiran SuryanarayanamurthyNessuna valutazione finora
- DRAFT Narrative-Report Case-StudyDocumento5 pagineDRAFT Narrative-Report Case-Studyboxed juiceNessuna valutazione finora
- Case Presentation On AppendicitisDocumento24 pagineCase Presentation On AppendicitissonutalkNessuna valutazione finora
- Test DrillsDocumento103 pagineTest DrillsOlive NNessuna valutazione finora
- Iap Immunization Guide Book 2009 2010Documento180 pagineIap Immunization Guide Book 2009 2010Muralikannan Mj100% (1)