Potrebbero piacerti anche
- PAPER WORKPaediatricsDocumento22 paginePAPER WORKPaediatricsIzzati OthmanNessuna valutazione finora
- Therapist's Guide to Pediatric Affect and Behavior RegulationDa EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNessuna valutazione finora
- MPDF PDFDocumento3 pagineMPDF PDFMariana DanNessuna valutazione finora
- Manual for Child and Vision Development MilestoneDa EverandManual for Child and Vision Development MilestoneNessuna valutazione finora
- Clinical Guide to Assessment and Treatment of Communication DisordersDa EverandClinical Guide to Assessment and Treatment of Communication DisordersNessuna valutazione finora
- Autism Guideline For PatientsDocumento2 pagineAutism Guideline For PatientsNastitiPutriArianiNessuna valutazione finora
- They Are What You Feed Them: How Food Can Improve Your Child’s Behaviour, Mood and LearningDa EverandThey Are What You Feed Them: How Food Can Improve Your Child’s Behaviour, Mood and LearningNessuna valutazione finora
- Primary Therapies: Read, Read, Read. Sensory World (Documento4 paginePrimary Therapies: Read, Read, Read. Sensory World (Andreea SanduNessuna valutazione finora
- Attention-Deficit/Hyperactivity Disorder Clinical Practice Guideline: Diagnosis and Evaluation of The Child WithDocumento15 pagineAttention-Deficit/Hyperactivity Disorder Clinical Practice Guideline: Diagnosis and Evaluation of The Child WithSuppiah AnarsalamNessuna valutazione finora
- Overcoming Autism Spectrum Disorder in children: Empowering Young Minds: A Holistic Approach to Navigating Autism Spectrum Disorder in ChildrenDa EverandOvercoming Autism Spectrum Disorder in children: Empowering Young Minds: A Holistic Approach to Navigating Autism Spectrum Disorder in ChildrenNessuna valutazione finora
- Geriatric AssessmentDocumento27 pagineGeriatric AssessmentNeil Philip MaturanNessuna valutazione finora
- Comprehensive Geriatric AssessmentDocumento25 pagineComprehensive Geriatric Assessmentsantosestrella100% (6)
- AUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONDocumento5 pagineAUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONvai2Nessuna valutazione finora
- Pediatric Physical Therapy PrinciplesDocumento46 paginePediatric Physical Therapy PrinciplesrizabNessuna valutazione finora
- Handbook of Evidence-Based Practice in Clinical Psychology, Child and Adolescent DisordersDa EverandHandbook of Evidence-Based Practice in Clinical Psychology, Child and Adolescent DisordersNessuna valutazione finora
- Paediatric Physiotherapy for Children's Physical DevelopmentDocumento4 paginePaediatric Physiotherapy for Children's Physical Developmentnavuru5kNessuna valutazione finora
- Cerebral Palsy Prep CardDocumento4 pagineCerebral Palsy Prep CardBenNessuna valutazione finora
- Children's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationDa EverandChildren's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationNessuna valutazione finora
- Navigating the Spectrum: A Comprehensive Guide to AutismDa EverandNavigating the Spectrum: A Comprehensive Guide to AutismNessuna valutazione finora
- Gordons Functional Health AssessmentDocumento73 pagineGordons Functional Health Assessmentdigracia manatigaNessuna valutazione finora
- Nutrition Management For Cerebral PalsyDocumento27 pagineNutrition Management For Cerebral PalsyPCMC Dietitians NDDNessuna valutazione finora
- 09 ABCs of Ped PTDocumento3 pagine09 ABCs of Ped PTGabriela MarinNessuna valutazione finora
- Peds 2011-2654 FullDocumento18 paginePeds 2011-2654 FullOriana CamposNessuna valutazione finora
- Attention Deficit/Hyperactivity Disorder, Screen Time, Physical Activity, And Diet Quality: An EssayDa EverandAttention Deficit/Hyperactivity Disorder, Screen Time, Physical Activity, And Diet Quality: An EssayValutazione: 2 su 5 stelle2/5 (1)
- Management of Children With Cerebral PalsyDocumento45 pagineManagement of Children With Cerebral PalsyNamakau MuliloNessuna valutazione finora
- How to diagnose autism: Early signs and assessmentsDocumento5 pagineHow to diagnose autism: Early signs and assessmentsYeni ZeonNessuna valutazione finora
- Diagnosis and Treatment of Children With Autism Spectrum DisordersDa EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersValutazione: 5 su 5 stelle5/5 (1)
- Autism and OTDocumento8 pagineAutism and OTNameeta Shroff JainNessuna valutazione finora
- Educational Strategies for Children With Autism Spectrum DisordersDa EverandEducational Strategies for Children With Autism Spectrum DisordersNessuna valutazione finora
- When Your Child Hates Food: Parent’s Practical Guide to Help Kids Overcome Eating Disorder (Anorexia)Da EverandWhen Your Child Hates Food: Parent’s Practical Guide to Help Kids Overcome Eating Disorder (Anorexia)Valutazione: 5 su 5 stelle5/5 (1)
- Caring for Your School-Age Child: Ages 5-12Da EverandCaring for Your School-Age Child: Ages 5-12Nessuna valutazione finora
- The Clinical Guide to Assessment and Treatment of Childhood Learning and Attention ProblemsDa EverandThe Clinical Guide to Assessment and Treatment of Childhood Learning and Attention ProblemsNessuna valutazione finora
- ADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentDocumento18 pagineADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentBen CulpepperNessuna valutazione finora
- Assessment of Hearing Loss in ChildrenDocumento25 pagineAssessment of Hearing Loss in ChildrenCristóbal Murillo MuñozNessuna valutazione finora
- ADHD, Comprehensive Guide: A Comprehensive Guide to Understanding, Diagnosis, and TreatmentDa EverandADHD, Comprehensive Guide: A Comprehensive Guide to Understanding, Diagnosis, and TreatmentNessuna valutazione finora
- The ADHD Handbook for Schools: Effective Strategies for Identifying and Teaching Students with Attention-Deficit/Hyperactivity DisorderDa EverandThe ADHD Handbook for Schools: Effective Strategies for Identifying and Teaching Students with Attention-Deficit/Hyperactivity DisorderValutazione: 5 su 5 stelle5/5 (1)
- The Clinician's Guide to Cognitive-Behavioral Therapy for Childhood Obsessive-Compulsive DisorderDa EverandThe Clinician's Guide to Cognitive-Behavioral Therapy for Childhood Obsessive-Compulsive DisorderEric A. StorchNessuna valutazione finora
- Askep Autisme 2Documento9 pagineAskep Autisme 2Ririn sagitaNessuna valutazione finora
- ADHD: Attention Deficit Hyperactivity Disorder: The 21 st century illness?Da EverandADHD: Attention Deficit Hyperactivity Disorder: The 21 st century illness?Nessuna valutazione finora
- Indus College of Nursing & MidwiferyDocumento52 pagineIndus College of Nursing & MidwiferyArsalan khanNessuna valutazione finora
- A Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareDa EverandA Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareNessuna valutazione finora
- FinalautismbookletDocumento10 pagineFinalautismbookletapi-228136529Nessuna valutazione finora
- The Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary CareDocumento8 pagineThe Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary CarecpNessuna valutazione finora
- Emotional and Behavioral Problems: A Handbook for Understanding and Handling StudentsDa EverandEmotional and Behavioral Problems: A Handbook for Understanding and Handling StudentsNessuna valutazione finora
- HOLISTIC APPROACH TO TREATMENT OF CHILDREN WITH SPECIAL NEEDSDa EverandHOLISTIC APPROACH TO TREATMENT OF CHILDREN WITH SPECIAL NEEDSNessuna valutazione finora
- ADHD Pathway GuideDocumento28 pagineADHD Pathway GuideFreditya Mahendra Putra100% (1)
- Nutritional and Herbal Therapies for Children and Adolescents: A Handbook for Mental Health CliniciansDa EverandNutritional and Herbal Therapies for Children and Adolescents: A Handbook for Mental Health CliniciansNessuna valutazione finora
- Autism: The Management and Support of Children and Young People On The Autism SpectrumDocumento36 pagineAutism: The Management and Support of Children and Young People On The Autism SpectrumPauNessuna valutazione finora
- Health and Wellness: DR Kainat Faizan BSPT (G Old-Medalist), PPDPTDocumento32 pagineHealth and Wellness: DR Kainat Faizan BSPT (G Old-Medalist), PPDPTAflaha KhanNessuna valutazione finora
- Autism Clinical Prep CardDocumento3 pagineAutism Clinical Prep CardBenNessuna valutazione finora
- Cerebral Palsy Theory 3 EssayDocumento7 pagineCerebral Palsy Theory 3 Essayapi-315331895Nessuna valutazione finora
- Rehabilitation PsychologyDocumento22 pagineRehabilitation PsychologyGURNOOR KAURNessuna valutazione finora
- Timely Interventions: A Parent's Guide to Help Your Child with Special NeedsDa EverandTimely Interventions: A Parent's Guide to Help Your Child with Special NeedsNessuna valutazione finora
- Learning with ADHD - A Practical Guide to Manage and Master ADHD in ChildrenDa EverandLearning with ADHD - A Practical Guide to Manage and Master ADHD in ChildrenNessuna valutazione finora
- Pediatrics 2011 Peds.2011 2654Documento18 paginePediatrics 2011 Peds.2011 2654Mauricio Pincheira GuerreroNessuna valutazione finora
- Autism Evaluation Online WorkshopDocumento29 pagineAutism Evaluation Online WorkshopQurrat ulainNessuna valutazione finora
- Opt Nextsteps06Documento8 pagineOpt Nextsteps06api-297150429Nessuna valutazione finora
- Caring for Senior Pets: Tips and Strategies for Meeting the Needs of Aging PetsDa EverandCaring for Senior Pets: Tips and Strategies for Meeting the Needs of Aging PetsNessuna valutazione finora
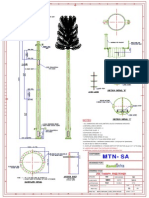
- 15m Camouflage DrawingDocumento1 pagina15m Camouflage DrawingRamadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- I S 456 Ammenment 3 - 2007Documento3 pagineI S 456 Ammenment 3 - 2007Gopi Raja100% (2)
- STL HelpDocumento3 pagineSTL HelpDaniela CazarottiNessuna valutazione finora
- Guy Anchor Design 9sqmDocumento9 pagineGuy Anchor Design 9sqmRamadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- ZProject Head - BIJOY P C - 14 Yrs - B.tech - Kochi (Kerala)Documento4 pagineZProject Head - BIJOY P C - 14 Yrs - B.tech - Kochi (Kerala)Ramadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- Total Month December S.No Description Last Date Amount Status Paid AmountDocumento2 pagineTotal Month December S.No Description Last Date Amount Status Paid AmountRamadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- BEPL designs infrastructure solutionsDocumento38 pagineBEPL designs infrastructure solutionsRamadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- Eurocode 3 steel joint design guideDocumento2 pagineEurocode 3 steel joint design guideneverreturnNessuna valutazione finora
- Dinesh TicketDocumento1 paginaDinesh TicketChandra Ganesh ChowdaryNessuna valutazione finora
- CC C CCC C C C C - C - !" #$%!&' !! - : Paper-2 (Concerned Subject) Electrical EngineeringDocumento3 pagineCC C CCC C C C C - C - !" #$%!&' !! - : Paper-2 (Concerned Subject) Electrical EngineeringRamadugula Rama Subrahmanya VenkateswararaoNessuna valutazione finora
- Ashtalakshmi Stotra-2Documento2 pagineAshtalakshmi Stotra-2Hima ShankarNessuna valutazione finora
- Terms and ConditionsDocumento2 pagineTerms and ConditionsSwati TandonNessuna valutazione finora
- Mitchell, Carol - ResumeDocumento2 pagineMitchell, Carol - Resumeapi-238460511Nessuna valutazione finora
- Occupational Therapists' Experiences in Extending Services in Metro Manila Tertiariy Hospitals - Proposed Employment Development StrategiesDocumento147 pagineOccupational Therapists' Experiences in Extending Services in Metro Manila Tertiariy Hospitals - Proposed Employment Development StrategiesRonnie Sta TeresaNessuna valutazione finora
- Test-Retest Reliability of The Purdue Pegboard Test: Bri Ef ReportDocumento4 pagineTest-Retest Reliability of The Purdue Pegboard Test: Bri Ef Report蘇柏霖Nessuna valutazione finora
- The Intentional Relationship Occupational Therapy and Use of Self 2nd EditionDocumento401 pagineThe Intentional Relationship Occupational Therapy and Use of Self 2nd Editiondana ries100% (3)
- EKOS - A SMART SolutionDocumento6 pagineEKOS - A SMART SolutionSpeech & Language Therapy in PracticeNessuna valutazione finora
- 10Documento8 pagine10Gabriela LalaNessuna valutazione finora
- Nursing Leadership and Management Case StudyDocumento9 pagineNursing Leadership and Management Case StudyCamille GraceNessuna valutazione finora
- Characterizing OT Practice Stroke Rehab RichardsDocumento10 pagineCharacterizing OT Practice Stroke Rehab Richardssidney drecotteNessuna valutazione finora
- Case-Smiths Occupational Therapy For Children and Adolescents - Ebook (Jane Clifford OBrien Heather Kuhaneck)Documento1.597 pagineCase-Smiths Occupational Therapy For Children and Adolescents - Ebook (Jane Clifford OBrien Heather Kuhaneck)Anthony stark100% (7)
- Writing Occupational Therapy Sample Test 1 PDFDocumento5 pagineWriting Occupational Therapy Sample Test 1 PDFKumarisarithaNessuna valutazione finora
- Guidelines For Documentation of Occupational Therapy PDFDocumento7 pagineGuidelines For Documentation of Occupational Therapy PDFMaria Airam100% (2)
- Rehabilitation in Palliative CareDocumento38 pagineRehabilitation in Palliative CareFiona 'Hope' RaeNessuna valutazione finora
- Generic Letter For Elective Requests - 2023Documento1 paginaGeneric Letter For Elective Requests - 2023EbrahimNessuna valutazione finora
- Safecom Revised August 2023Documento17 pagineSafecom Revised August 2023api-699389850Nessuna valutazione finora
- Business Communication Case StudyDocumento2 pagineBusiness Communication Case StudyalexNessuna valutazione finora
- Dysphagia PDFDocumento6 pagineDysphagia PDFPavel LeahuNessuna valutazione finora
- ASRA - School For Children With Special NeedsDocumento10 pagineASRA - School For Children With Special NeedsJoyce Ellen Hernandez JavierNessuna valutazione finora
- Paediatric Intake Form Modern OT 2018Documento6 paginePaediatric Intake Form Modern OT 2018SefNessuna valutazione finora
- AOTA Handout - Establishing Toileting Routines For ChildrenDocumento2 pagineAOTA Handout - Establishing Toileting Routines For ChildrenCharisse Martha Leyba100% (1)
- Occupational Performance CoachingDocumento8 pagineOccupational Performance CoachingEtneciv ParedesNessuna valutazione finora
- Adapted Physical Education: A GuideDocumento6 pagineAdapted Physical Education: A GuideAldre MalupengNessuna valutazione finora
- U.S. Army Medical Specialist Corps Fact SheetDocumento6 pagineU.S. Army Medical Specialist Corps Fact SheetU.S. Army Medical Department (AMEDD)Nessuna valutazione finora
- DysfagiaDocumento4 pagineDysfagiaVarvara MarkoulakiNessuna valutazione finora
- Modulo 03 CONTROL DE LECTURADocumento10 pagineModulo 03 CONTROL DE LECTURAGloria Morales BastiasNessuna valutazione finora
- CapstoneessayDocumento5 pagineCapstoneessayapi-256089742Nessuna valutazione finora
- The 1969 Eleanor Clarke Slagel LectureDocumento7 pagineThe 1969 Eleanor Clarke Slagel LectureAde Perez Otero100% (1)
- Telehealth in Occupational Therapy: AOTA Position PaperDocumento18 pagineTelehealth in Occupational Therapy: AOTA Position PaperdanielNessuna valutazione finora
- Effects of An Energy Conservation Course On Fatigue Impact For Persons With Progressive Multiple SclerosisDocumento9 pagineEffects of An Energy Conservation Course On Fatigue Impact For Persons With Progressive Multiple SclerosisXouya SuizenNessuna valutazione finora
- Work and Occupational TherapyDocumento31 pagineWork and Occupational Therapysmith197077Nessuna valutazione finora
- Occupational TherapyDocumento15 pagineOccupational Therapymanu sethi100% (1)