Potrebbero piacerti anche
- Metronidazole Baxter in FDocumento12 pagineMetronidazole Baxter in Fgautam gurjarNessuna valutazione finora
- Metronidazole AFTinfDocumento8 pagineMetronidazole AFTinfSmartishag BediakoNessuna valutazione finora
- Metronidazole Injection for Treating Anaerobic Bacterial InfectionsDocumento20 pagineMetronidazole Injection for Treating Anaerobic Bacterial InfectionsYuniNessuna valutazione finora
- Dailymed - Nlm.nih - Gov METRONIDAZOLEDocumento16 pagineDailymed - Nlm.nih - Gov METRONIDAZOLELip StickNessuna valutazione finora
- Clinical Pharmacology Module 14 1Documento14 pagineClinical Pharmacology Module 14 1Steven Mark MananguNessuna valutazione finora
- Klint Klint: Tablets/Injection SuspensionDocumento1 paginaKlint Klint: Tablets/Injection SuspensionibtesamNessuna valutazione finora
- Flagyl Metronidazole TabletsDocumento11 pagineFlagyl Metronidazole TabletsYantari TiyoraNessuna valutazione finora
- FlagystatinDocumento18 pagineFlagystatinChristian YongkyNessuna valutazione finora
- Flagyl-suspension-SmPC-05.2021 For DistributionDocumento9 pagineFlagyl-suspension-SmPC-05.2021 For Distributionrx bafnaNessuna valutazione finora
- MetronidazoleDocumento3 pagineMetronidazoleAvigale Arcillas BasilioNessuna valutazione finora
- Metronidazole Problems and Solutions ReviewDocumento21 pagineMetronidazole Problems and Solutions Reviewصباح جوادNessuna valutazione finora
- Preformulation of MetronidazoleDocumento11 paginePreformulation of MetronidazoleJoseLuisHuamanNessuna valutazione finora
- Metronidazol PropiedadesDocumento9 pagineMetronidazol PropiedadesYonatan Gómez VargasNessuna valutazione finora
- Anti-Amoebic Drugs: Madan Sigdel Lecturer Department of Pharmacology Gandaki Medical CollegeDocumento21 pagineAnti-Amoebic Drugs: Madan Sigdel Lecturer Department of Pharmacology Gandaki Medical Collegemadan sigdelNessuna valutazione finora
- Metro Dinaz OleDocumento3 pagineMetro Dinaz OleFadli ArchieNessuna valutazione finora
- Metro Nida ZolDocumento9 pagineMetro Nida ZolAnna Thalita CardosoNessuna valutazione finora
- MetronidazoleDocumento5 pagineMetronidazoleGwyneth JangadNessuna valutazione finora
- Metoclopramide HCL Metoclopramide Inj 10mg-2ml IreDocumento7 pagineMetoclopramide HCL Metoclopramide Inj 10mg-2ml IresiripNessuna valutazione finora
- Anthelmintic Drugs: Pharmacology IvDocumento27 pagineAnthelmintic Drugs: Pharmacology IvShashidharan MenonNessuna valutazione finora
- Flagystatin SG 1222Documento15 pagineFlagystatin SG 1222MarjMalubayArriolaNessuna valutazione finora
- Depo MedrolDocumento33 pagineDepo MedrolarianjafarirmNessuna valutazione finora
- Obat - BMDocumento50 pagineObat - BMNovita PermataNessuna valutazione finora
- Baby Case Study (FINAL)Documento44 pagineBaby Case Study (FINAL)Rouie Björn ABrianNessuna valutazione finora
- Therapeutic Uses of Metronidazole and Its Side Effects: An UpdateDocumento5 pagineTherapeutic Uses of Metronidazole and Its Side Effects: An UpdateSandrina NajwaNessuna valutazione finora
- Medsafe Data Sheet Dotareminj - Prefilled Syringe PDFDocumento6 pagineMedsafe Data Sheet Dotareminj - Prefilled Syringe PDFizalxrayNessuna valutazione finora
- Tinidazole Is An AntiDocumento6 pagineTinidazole Is An AntiNoi Maya Anggrita SariNessuna valutazione finora
- Decadron: (Dexamethasone Tablets, Usp)Documento8 pagineDecadron: (Dexamethasone Tablets, Usp)Anonymous QqyLDoW1Nessuna valutazione finora
- (500 MG Metronidazole and 100,000 IU Nystatin) Vaginal OvulesDocumento22 pagine(500 MG Metronidazole and 100,000 IU Nystatin) Vaginal OvulesAngel CoNessuna valutazione finora
- C1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Documento13 pagineC1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Mina AzmyNessuna valutazione finora
- Farmakologi Obat Kusta Dan Antiparasit 2015Documento84 pagineFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandNessuna valutazione finora
- Metronidazole uses, side effects and nursing considerationsDocumento2 pagineMetronidazole uses, side effects and nursing considerationshauteanicoleNessuna valutazione finora
- 12623slr059 Flagyl LBLDocumento7 pagine12623slr059 Flagyl LBLgeeenaaNessuna valutazione finora
- Daunorubicin: Drug NameDocumento7 pagineDaunorubicin: Drug NameEdgar Ledesma-MartínezNessuna valutazione finora
- Trusopt: (Dorzolamide Hydrochloride Ophthalmic Solution)Documento16 pagineTrusopt: (Dorzolamide Hydrochloride Ophthalmic Solution)Upik MoritaNessuna valutazione finora
- EPS Ec MetoclopramideDocumento3 pagineEPS Ec MetoclopramideMrprads5Nessuna valutazione finora
- Mot Ilium TabDocumento11 pagineMot Ilium TabChandra FatmaNessuna valutazione finora
- Metronidazole Drug StudyDocumento2 pagineMetronidazole Drug StudyJessica Christine Datuin Gustilo100% (1)
- S 039 LBLDocumento45 pagineS 039 LBLAstha BhalodiaNessuna valutazione finora
- Pharmacology Final Exam Name: SectionDocumento19 paginePharmacology Final Exam Name: SectionGlen Norwel LabayogNessuna valutazione finora
- Keto Vs Mikonazol PharmacologyDocumento6 pagineKeto Vs Mikonazol PharmacologyRanda NovalinoNessuna valutazione finora
- KETOCONAZOLEDocumento22 pagineKETOCONAZOLEAbdul khodir jaelaniNessuna valutazione finora
- Ethambutol HydrochlorideDocumento10 pagineEthambutol HydrochlorideAdithFullNessuna valutazione finora
- MetronidazoleDocumento26 pagineMetronidazoleNdayisaba CorneilleNessuna valutazione finora
- Danladi Emmanuel 20CH1024Documento11 pagineDanladi Emmanuel 20CH1024Mohammed kashimNessuna valutazione finora
- AntimetabolitesDocumento25 pagineAntimetabolitestheintrovNessuna valutazione finora
- Nor Metrogyl KDocumento5 pagineNor Metrogyl KManish ShankarpureNessuna valutazione finora
- Antiprotozoal Drugs I: Metronidazole and Tinidazole for AmebiasisDocumento36 pagineAntiprotozoal Drugs I: Metronidazole and Tinidazole for AmebiasisShashidharan MenonNessuna valutazione finora
- ETHAMBUTOLDocumento11 pagineETHAMBUTOLIrbasMantiniSyaifulNessuna valutazione finora
- Nitrofurantoin: Tejal Khade Assistant Professor KGRDCP & RiDocumento10 pagineNitrofurantoin: Tejal Khade Assistant Professor KGRDCP & RiAkshada bhangreNessuna valutazione finora
- TB TreatmentDocumento58 pagineTB TreatmentNdayisaba CorneilleNessuna valutazione finora
- Antiproto & AnthelminticsDocumento57 pagineAntiproto & AnthelminticsDrMohan GuptaNessuna valutazione finora
- For Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsDocumento3 pagineFor Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsAnastasia Lilian SuryajayaNessuna valutazione finora
- RPHS 084Documento8 pagineRPHS 084Amik IndrayaniNessuna valutazione finora
- Targocid - PI - Sanofi Aventis - MCC Format 24 January 2019Documento15 pagineTargocid - PI - Sanofi Aventis - MCC Format 24 January 2019DR JAMAL WARISNessuna valutazione finora
- Medical Management 3 Objectives of ManagementDocumento4 pagineMedical Management 3 Objectives of ManagementSaima Sawal SalicNessuna valutazione finora
- AMOEBIASISDocumento67 pagineAMOEBIASISmahveen balochNessuna valutazione finora
- Nitrofurantoin Drug StudyDocumento11 pagineNitrofurantoin Drug StudyNicole Keesha MataNessuna valutazione finora
- The Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.Da EverandThe Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.Nessuna valutazione finora
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESDa EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESNessuna valutazione finora
- Dietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiaDocumento7 pagineDietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiamustikaarumNessuna valutazione finora
- 24 4 385Documento6 pagine24 4 385mustikaarumNessuna valutazione finora
- Nutrition and Stroke: Review ArticleDocumento9 pagineNutrition and Stroke: Review Articlerichie_ciandraNessuna valutazione finora
- ViaClinica RICA EnglishDocumento127 pagineViaClinica RICA EnglishmustikaarumNessuna valutazione finora
- Bushra, 2010Documento7 pagineBushra, 2010Citta ArastiNessuna valutazione finora
- Gastric Volvulus: Bang Chau, Susan DufelDocumento2 pagineGastric Volvulus: Bang Chau, Susan DufelmustikaarumNessuna valutazione finora
- Parenteral Nutrition in Critical CareDocumento5 pagineParenteral Nutrition in Critical CaremustikaarumNessuna valutazione finora
- Selected Health IndicatorsDocumento93 pagineSelected Health IndicatorsmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
- Cooking RequirementsDocumento1 paginaCooking RequirementsvectorNessuna valutazione finora
- Logistics Execution Suite Manages Warehouse OperationsDocumento9 pagineLogistics Execution Suite Manages Warehouse OperationsmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
- Vitamind - TB PDFDocumento7 pagineVitamind - TB PDFmustikaarumNessuna valutazione finora
- Tingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarDocumento4 pagineTingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
- Reliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodDocumento5 pagineReliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodmustikaarumNessuna valutazione finora
- BCAADocumento8 pagineBCAAmustikaarumNessuna valutazione finora
- Laporan Week 9 BDocumento36 pagineLaporan Week 9 BmustikaarumNessuna valutazione finora
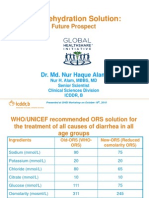
- Oral Rehydration Solution:: Future ProspectDocumento48 pagineOral Rehydration Solution:: Future ProspectmustikaarumNessuna valutazione finora
- Ioi 160069Documento9 pagineIoi 160069mustikaarumNessuna valutazione finora
- Posterior Sagittal Anorectoplasty in Anorectal MalformationsDocumento5 paginePosterior Sagittal Anorectoplasty in Anorectal MalformationsmustikaarumNessuna valutazione finora
- Metronidazole: Common Drug Name Common Brand NamesDocumento1 paginaMetronidazole: Common Drug Name Common Brand NamesmustikaarumNessuna valutazione finora
- Diarrhoea Guidelines PDFDocumento58 pagineDiarrhoea Guidelines PDFmustikaarumNessuna valutazione finora
- Micronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93Documento9 pagineMicronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93mustikaarumNessuna valutazione finora
- 18 Total Quality ApstractDocumento5 pagine18 Total Quality ApstractPooja GuptaNessuna valutazione finora
- Mustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsDocumento18 pagineMustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsmustikaarumNessuna valutazione finora
- Hungx BuiDocumento92 pagineHungx BuimustikaarumNessuna valutazione finora
- Consumer Medicine Information Arrow - Ranitidine: What Is in This LeafletDocumento8 pagineConsumer Medicine Information Arrow - Ranitidine: What Is in This LeafletmustikaarumNessuna valutazione finora
- Nousea and Vomiting Mediciation 130509Documento3 pagineNousea and Vomiting Mediciation 130509mustikaarumNessuna valutazione finora
- Bilirubin Production: Hemoglobin (70 To 80%) Erythroid Cells Heme Proteins Myoglobin, Cytochromes (20 To 25%)Documento5 pagineBilirubin Production: Hemoglobin (70 To 80%) Erythroid Cells Heme Proteins Myoglobin, Cytochromes (20 To 25%)Daffa Samudera Nakz DoeratipNessuna valutazione finora
- Anticoagulant and Antiplatelet Medications and Dental Procedures ADADocumento8 pagineAnticoagulant and Antiplatelet Medications and Dental Procedures ADADeeNessuna valutazione finora
- Speech in ActionDocumento160 pagineSpeech in ActionSplashXNessuna valutazione finora
- HSPK 2021Documento270 pagineHSPK 2021Sabrina Agustien SimanungkalitNessuna valutazione finora
- Emergency Preparedness Concepts Test BankDocumento13 pagineEmergency Preparedness Concepts Test BankTyson Easo JonesNessuna valutazione finora
- v1 High Sensitivity C-Reactive Protein HSCDocumento2 paginev1 High Sensitivity C-Reactive Protein HSCKhendy SugihartoNessuna valutazione finora
- Joint InfectionsDocumento10 pagineJoint InfectionsJPNessuna valutazione finora
- Psychological Point of ViewDocumento3 paginePsychological Point of ViewForam PatelNessuna valutazione finora
- Prothrombin Time Normal RangeDocumento2 pagineProthrombin Time Normal RangeKent AlveNessuna valutazione finora
- RAV Admission Notice for Ayurveda CoursesDocumento4 pagineRAV Admission Notice for Ayurveda CoursesBhargav KalalNessuna valutazione finora
- Vitamins Are Organic Compounds Required in The Diet in Small Quantities To Perform Biological FunctionsDocumento70 pagineVitamins Are Organic Compounds Required in The Diet in Small Quantities To Perform Biological FunctionsRose LiteNessuna valutazione finora
- Scrotal HerniaDocumento9 pagineScrotal HerniaReymart BolagaoNessuna valutazione finora
- Hyperthermia and Risk For AspirationDocumento3 pagineHyperthermia and Risk For AspirationAlmyr RimandoNessuna valutazione finora
- Lactose intolerance diagnosis and treatmentDocumento12 pagineLactose intolerance diagnosis and treatmentNico BatallaNessuna valutazione finora
- Pelvic Floor Exercises in The Elderly Irmina Nahon1Documento34 paginePelvic Floor Exercises in The Elderly Irmina Nahon1Anonymous C7H7wS6Nessuna valutazione finora
- Cardiogenic Shock Causes and TreatmentDocumento43 pagineCardiogenic Shock Causes and TreatmentGalih Arief Harimurti WawolumajaNessuna valutazione finora
- ق 4Documento36 pagineق 4Zainab HasanNessuna valutazione finora
- Hydralazine For Severe PIHDocumento4 pagineHydralazine For Severe PIHYwagar YwagarNessuna valutazione finora
- ReviewerDocumento20 pagineReviewerYang MolosNessuna valutazione finora
- Basic Load (Individual) Veterinarian Field PackDocumento3 pagineBasic Load (Individual) Veterinarian Field PackJohn MillerNessuna valutazione finora
- Pathology - List - 89.8.20Documento25 paginePathology - List - 89.8.20Mamula RiazNessuna valutazione finora
- Child Development Mannualfinal-SinhalaDocumento250 pagineChild Development Mannualfinal-SinhalaAshhara FazalNessuna valutazione finora
- Class 11 English Snapshots Chapter 7Documento2 pagineClass 11 English Snapshots Chapter 7Alpha StarNessuna valutazione finora
- Sound Transduction EarDocumento7 pagineSound Transduction Earhsc5013100% (1)
- 2014 Body Code Client Information PDFDocumento7 pagine2014 Body Code Client Information PDFkrug100% (1)
- Cognitv EmphatyDocumento6 pagineCognitv EmphatyAndrea MenesesNessuna valutazione finora
- Physiotherapy in LeprosyDocumento4 paginePhysiotherapy in LeprosymichaelsophianNessuna valutazione finora
- Pest Control Risk Assessment Indoor and OutdoorDocumento72 paginePest Control Risk Assessment Indoor and OutdoorarmkarthickNessuna valutazione finora
- Elphos Erald: Second Shot: Hillary Clinton Running Again For PresidentDocumento10 pagineElphos Erald: Second Shot: Hillary Clinton Running Again For PresidentThe Delphos HeraldNessuna valutazione finora
- Caesalpinia CristaDocumento5 pagineCaesalpinia CristaDarmawan Said100% (1)