Potrebbero piacerti anche
- 1 Intro To EpidemiologyDocumento20 pagine1 Intro To EpidemiologyamylaNessuna valutazione finora
- Lynch SyndromeDocumento3 pagineLynch SyndromeAmy LaPointeNessuna valutazione finora
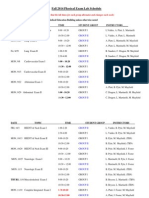
- Fall 2014 Physical Exam Lab Schedule: (Please Note That The Lab Times For Each Group Alternates and Changes Each Week)Documento3 pagineFall 2014 Physical Exam Lab Schedule: (Please Note That The Lab Times For Each Group Alternates and Changes Each Week)Amy LaPointeNessuna valutazione finora
- Direct To Consumer TestingDocumento2 pagineDirect To Consumer TestingAmy LaPointeNessuna valutazione finora
- Experiment 1 Organic Chemistry PanacetinDocumento6 pagineExperiment 1 Organic Chemistry PanacetinAmy LaPointe0% (1)
- Separating The Components of Panacetin PrelabDocumento5 pagineSeparating The Components of Panacetin PrelabAmy LaPointe100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Proposed) Declaration of Factual Innocence Under Penal Code Section 851.8 and OrderDocumento4 pagineProposed) Declaration of Factual Innocence Under Penal Code Section 851.8 and OrderBobby Dearfield100% (1)
- A Beautiful Mind - Psychology AnalysisDocumento15 pagineA Beautiful Mind - Psychology AnalysisFitto Priestaza91% (34)
- SHS PE MODULE 1 - RemovedDocumento21 pagineSHS PE MODULE 1 - RemovedXypher NNessuna valutazione finora
- Adverbs Before AdjectivesDocumento2 pagineAdverbs Before AdjectivesJuan Sanchez PrietoNessuna valutazione finora
- Q3 Grade 8 Week 4Documento15 pagineQ3 Grade 8 Week 4aniejeonNessuna valutazione finora
- Extinct Endangered Species PDFDocumento2 pagineExtinct Endangered Species PDFTheresaNessuna valutazione finora
- Rele A Gas BuchholtsDocumento18 pagineRele A Gas BuchholtsMarco GiraldoNessuna valutazione finora
- Materials System SpecificationDocumento14 pagineMaterials System Specificationnadeem shaikhNessuna valutazione finora
- Chapin Columbus DayDocumento15 pagineChapin Columbus Dayaspj13Nessuna valutazione finora
- Design of Corn ThresherDocumento11 pagineDesign of Corn ThresherFrancisco ToroNessuna valutazione finora
- DLL LayoutDocumento4 pagineDLL LayoutMarife GuadalupeNessuna valutazione finora
- Meike SchalkDocumento212 pagineMeike SchalkPetra BoulescuNessuna valutazione finora
- Fry 2016Documento27 pagineFry 2016Shahid RashidNessuna valutazione finora
- Roberts, Donaldson. Ante-Nicene Christian Library: Translations of The Writings of The Fathers Down To A. D. 325. 1867. Volume 15.Documento564 pagineRoberts, Donaldson. Ante-Nicene Christian Library: Translations of The Writings of The Fathers Down To A. D. 325. 1867. Volume 15.Patrologia Latina, Graeca et OrientalisNessuna valutazione finora
- Lista Agentiilor de Turism Licentiate Actualizare 16.09.2022Documento498 pagineLista Agentiilor de Turism Licentiate Actualizare 16.09.2022LucianNessuna valutazione finora
- Jaimini Astrology and MarriageDocumento3 pagineJaimini Astrology and MarriageTushar Kumar Bhowmik100% (1)
- Volvo D16 Engine Family: SpecificationsDocumento3 pagineVolvo D16 Engine Family: SpecificationsJicheng PiaoNessuna valutazione finora
- GemDocumento135 pagineGemZelia GregoriouNessuna valutazione finora
- The BreakupDocumento22 pagineThe BreakupAllison CreaghNessuna valutazione finora
- Wwe SVR 2006 07 08 09 10 11 IdsDocumento10 pagineWwe SVR 2006 07 08 09 10 11 IdsAXELL ENRIQUE CLAUDIO MENDIETANessuna valutazione finora
- Introduction To Philosophy of The Human Person: Presented By: Mr. Melvin J. Reyes, LPTDocumento27 pagineIntroduction To Philosophy of The Human Person: Presented By: Mr. Melvin J. Reyes, LPTMelvin J. Reyes100% (2)
- Field Assignment On Feacal Sludge ManagementDocumento10 pagineField Assignment On Feacal Sludge ManagementSarah NamyaloNessuna valutazione finora
- Jurnal UlkusDocumento6 pagineJurnal UlkusIndri AnggraeniNessuna valutazione finora
- S Jozsef Viata in DiosigDocumento52 pagineS Jozsef Viata in Diosigunoradean2Nessuna valutazione finora
- Logo DesignDocumento4 pagineLogo Designdarshan kabraNessuna valutazione finora
- Science Project FOLIO About Density KSSM Form 1Documento22 pagineScience Project FOLIO About Density KSSM Form 1SarveesshNessuna valutazione finora
- BRAC BrochureDocumento2 pagineBRAC BrochureKristin SoukupNessuna valutazione finora
- Espn NFL 2k5Documento41 pagineEspn NFL 2k5jojojojo231Nessuna valutazione finora
- Alice (Alice's Adventures in Wonderland)Documento11 pagineAlice (Alice's Adventures in Wonderland)Oğuz KarayemişNessuna valutazione finora
- Outline - Criminal Law - RamirezDocumento28 pagineOutline - Criminal Law - RamirezgiannaNessuna valutazione finora