Potrebbero piacerti anche
- A Case Study About AbortionDocumento10 pagineA Case Study About AbortionPatricia JerusalemNessuna valutazione finora
- Sex ManualDocumento14 pagineSex ManualCally LiueNessuna valutazione finora
- Benign Gynecologic Lesions: Urethral Caruncle, Cyst, Nevus, Hemangioma, Fibroma, Lipoma, Endometriosis, Urethral DiverticulumDocumento158 pagineBenign Gynecologic Lesions: Urethral Caruncle, Cyst, Nevus, Hemangioma, Fibroma, Lipoma, Endometriosis, Urethral DiverticulumArianne Joy C. TamarayNessuna valutazione finora
- Ectopic PregnancyDocumento14 pagineEctopic PregnancytaufiqNessuna valutazione finora
- Premature Rupture of MembranesDocumento4 paginePremature Rupture of MembranesNikko Pabico67% (3)
- Maternity Nursing ReviewDocumento8 pagineMaternity Nursing ReviewJulienne Sanchez-Salazar100% (2)
- Nursing Care Plan Breast Feeding IneffectiveDocumento1 paginaNursing Care Plan Breast Feeding Ineffectivederic88% (8)
- Period Power by Maisie HillDocumento11 paginePeriod Power by Maisie HillsimasNessuna valutazione finora
- Grade 10 Science Quarter 3 WEEK 4 I.: Menstrual-CycleDocumento3 pagineGrade 10 Science Quarter 3 WEEK 4 I.: Menstrual-CycleAnn ClarisseNessuna valutazione finora
- HEICSDocumento36 pagineHEICSYeli Asti100% (1)
- Managing Placenta Accreta: Medical vs Surgical OptionsDocumento9 pagineManaging Placenta Accreta: Medical vs Surgical OptionsAslesa Wangpathi PagehgiriNessuna valutazione finora
- Obstetrics Mcqs PDFDocumento2 pagineObstetrics Mcqs PDFJennifer47% (17)
- Uterine Rupture in Nulliparous Woman Without Risk Factors: A Case Report and Literature ReviewDocumento6 pagineUterine Rupture in Nulliparous Woman Without Risk Factors: A Case Report and Literature ReviewBOHR International Journal on GynaecologyNessuna valutazione finora
- The Back Alley Revisited: Sepsis After Attempted Self-Induced AbortionDocumento3 pagineThe Back Alley Revisited: Sepsis After Attempted Self-Induced Abortionmila nurmalaNessuna valutazione finora
- Case Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaeDocumento4 pagineCase Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaemelisaberlianNessuna valutazione finora
- Placenta Increta Causing Um in The 26th Week of Pregnancy 2Documento3 paginePlacenta Increta Causing Um in The 26th Week of Pregnancy 2Kester ApostolNessuna valutazione finora
- Ultrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDocumento4 pagineUltrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDavid Eka PrasetyaNessuna valutazione finora
- Medicine: Intrauterine Device Found in An Ovarian TumorDocumento5 pagineMedicine: Intrauterine Device Found in An Ovarian TumorRezky amalia basirNessuna valutazione finora
- Acute Non-Puerperal Uterine Inversion Case ReportDocumento4 pagineAcute Non-Puerperal Uterine Inversion Case ReportALfuNessuna valutazione finora
- Cases Journal: Torsion of Ovarian Cyst During Pregnancy: A Case ReportDocumento3 pagineCases Journal: Torsion of Ovarian Cyst During Pregnancy: A Case ReportAde Gustina SiahaanNessuna valutazione finora
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDocumento6 pagineUC Irvine: Clinical Practice and Cases in Emergency MedicinePatrick NunsioNessuna valutazione finora
- Cesarean Scar Ectopic Pregnancy Case ReportDocumento6 pagineCesarean Scar Ectopic Pregnancy Case ReportMominah MayamNessuna valutazione finora
- 2 5 21 861 PDFDocumento3 pagine2 5 21 861 PDFAhmed ZidanNessuna valutazione finora
- Pregnancy in a Didelphic Uterus- A case ReportDocumento7 paginePregnancy in a Didelphic Uterus- A case ReportAmin BashyrNessuna valutazione finora
- Nir Hus Absite Review Q12Documento11 pagineNir Hus Absite Review Q12nir4846Nessuna valutazione finora
- Laparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDocumento4 pagineLaparoscopic Management of Cervical-Isthmic Pregnancy: A Proposal MethodDinorah MarcelaNessuna valutazione finora
- 9.radha Et Al.Documento3 pagine9.radha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)Nessuna valutazione finora
- Blighted Ovum: A Case ReportDocumento2 pagineBlighted Ovum: A Case Reportakhmad ikhwanNessuna valutazione finora
- Rectovaginal Fistulae: Bidhan Das, MD Michael Snyder, MDDocumento7 pagineRectovaginal Fistulae: Bidhan Das, MD Michael Snyder, MDNovaNessuna valutazione finora
- Ectopic PregnancyDocumento7 pagineEctopic PregnancyDeepshikha MahapatraNessuna valutazione finora
- Abnormal PlacentationDocumento9 pagineAbnormal PlacentationJack BladeNessuna valutazione finora
- Uterine Rupture at 21 Weeks in Twin Pregnancy WithDocumento5 pagineUterine Rupture at 21 Weeks in Twin Pregnancy WithGatoso OsoNessuna valutazione finora
- Laparoscopic Management of Rudimentary Uterine Horn Pregnancy: Case Report and Literature ReviewDocumento4 pagineLaparoscopic Management of Rudimentary Uterine Horn Pregnancy: Case Report and Literature ReviewCamacho OmarNessuna valutazione finora
- Ovarian Ectopic Pregnancy: A Rare Case: Iran J Reprod Med Vol. 12. No. 4. PP: 281-284, April 2014Documento4 pagineOvarian Ectopic Pregnancy: A Rare Case: Iran J Reprod Med Vol. 12. No. 4. PP: 281-284, April 2014alif bagusNessuna valutazione finora
- Ruptured Ectopic Pregnancy in The Presence of An Intrauterine DeviceDocumento5 pagineRuptured Ectopic Pregnancy in The Presence of An Intrauterine DevicePatrick NunsioNessuna valutazione finora
- Uterine Adherence To Anterior Abdominal Wall After Caesarean SectionDocumento3 pagineUterine Adherence To Anterior Abdominal Wall After Caesarean SectionGladstone AsadNessuna valutazione finora
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDocumento7 paginePrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naNessuna valutazione finora
- MainDocumento4 pagineMainselvia oktavianiNessuna valutazione finora
- Abrasio PlacentaDocumento3 pagineAbrasio Placentamuhammad azamNessuna valutazione finora
- Gynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernDocumento3 pagineGynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernIrvin MarcelNessuna valutazione finora
- Hematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDocumento3 pagineHematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDexter BluesNessuna valutazione finora
- Bilateral Tubo-Ovarian Abscess After Cesarean Delivery: A Case Report and Literature ReviewDocumento4 pagineBilateral Tubo-Ovarian Abscess After Cesarean Delivery: A Case Report and Literature ReviewIntan PermataNessuna valutazione finora
- 03 JCR 004 Rajendra EndometrialDocumento4 pagine03 JCR 004 Rajendra EndometrialReza HidayatNessuna valutazione finora
- Suspected Illegal Abortion and Unsafe Abortion Leading To Uterine RuptureDocumento4 pagineSuspected Illegal Abortion and Unsafe Abortion Leading To Uterine Ruptureoke boskuNessuna valutazione finora
- Vaginal Extrusion of A Ventriculoperitoneal Shunt A Case Report and Review ofDocumento10 pagineVaginal Extrusion of A Ventriculoperitoneal Shunt A Case Report and Review ofDian AdiNessuna valutazione finora
- Primary Ovarian Abscess in Pregnancy: Case ReportDocumento3 paginePrimary Ovarian Abscess in Pregnancy: Case ReportVinnyRevinaAdrianiNessuna valutazione finora
- Ectopic Pregnancy22Documento43 pagineEctopic Pregnancy22Sunil YadavNessuna valutazione finora
- Cesarean SectionDocumento139 pagineCesarean SectionMisganaw WorkuNessuna valutazione finora
- Ectopic PregenancyDocumento69 pagineEctopic PregenancyMahmoud AbbasNessuna valutazione finora
- Spontaneous Rupture of An Unscarred GravidDocumento4 pagineSpontaneous Rupture of An Unscarred GraviddelaNessuna valutazione finora
- Khing Journal...Documento5 pagineKhing Journal...Khing AbatNessuna valutazione finora
- A. Tunica Albuguinea: NCM 102: Assessment ExamDocumento9 pagineA. Tunica Albuguinea: NCM 102: Assessment ExamdubhieNessuna valutazione finora
- Primary Carcinoma of Fallopian Tube: Case Series Case ReportDocumento4 paginePrimary Carcinoma of Fallopian Tube: Case Series Case ReportChi NgôNessuna valutazione finora
- acute polihidramnios wong1986Documento4 pagineacute polihidramnios wong1986Francisco MirettiNessuna valutazione finora
- Anesthetic Management of An Undiagnosed Advanced Extrauterine Pregnancy Under Combined Spinal-Epidural AnesthesiaDocumento4 pagineAnesthetic Management of An Undiagnosed Advanced Extrauterine Pregnancy Under Combined Spinal-Epidural AnesthesiaHanayuki VizureiNessuna valutazione finora
- Case Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureDocumento9 pagineCase Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureYosie Yulanda PutraNessuna valutazione finora
- Term Live Primary Ovarian Pregnancy A Case ReportDocumento4 pagineTerm Live Primary Ovarian Pregnancy A Case ReportNico PlantadoNessuna valutazione finora
- Clinical Medicine Insights: Case ReportsDocumento4 pagineClinical Medicine Insights: Case ReportsJer KelNessuna valutazione finora
- MainDocumento3 pagineMaindivyanshu kumarNessuna valutazione finora
- Kista OvariumDocumento4 pagineKista OvariumAde Gustina SiahaanNessuna valutazione finora
- مرجع 2Documento4 pagineمرجع 2Ahmed AnwarNessuna valutazione finora
- A Case Report: Twisted Ovarian Cyst in PregnancyDocumento3 pagineA Case Report: Twisted Ovarian Cyst in PregnancyPHitphitt Jeleck SangaattNessuna valutazione finora
- Criog2014 108973Documento4 pagineCriog2014 108973Denia Haritsa AprilianiNessuna valutazione finora
- Article IJGCP 118Documento3 pagineArticle IJGCP 118Jessica MarianoNessuna valutazione finora
- Rare Uterine Leiomyoma in Adolescent FemaleDocumento3 pagineRare Uterine Leiomyoma in Adolescent Femaledr.putra888Nessuna valutazione finora
- Case Study-Endometrial PyometraDocumento7 pagineCase Study-Endometrial Pyometrasimbarashe tangwadzanaNessuna valutazione finora
- Spontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportDocumento2 pagineSpontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportTomy SaputraNessuna valutazione finora
- Uterine Myoma, Myomectomy and Minimally Invasive TreatmentsDa EverandUterine Myoma, Myomectomy and Minimally Invasive TreatmentsNessuna valutazione finora
- Damage Control in Trauma Care: An Evolving Comprehensive Team ApproachDa EverandDamage Control in Trauma Care: An Evolving Comprehensive Team ApproachJuan DuchesneNessuna valutazione finora
- Ni Hms 288677Documento15 pagineNi Hms 288677Yeli AstiNessuna valutazione finora
- Risk Factors Associated With Facial FracturesDocumento7 pagineRisk Factors Associated With Facial FracturesYeli AstiNessuna valutazione finora
- Canmedaj01175 0030Documento3 pagineCanmedaj01175 0030Yeli AstiNessuna valutazione finora
- Reliabel Sikap 1Documento3 pagineReliabel Sikap 1Yeli AstiNessuna valutazione finora
- Obsgyn BooksDocumento4 pagineObsgyn BooksYulian NuswantoroNessuna valutazione finora
- Pustaka CannabisDocumento2 paginePustaka CannabisYeli AstiNessuna valutazione finora
- Molluscum Contagiosum Treatment OptionsDocumento12 pagineMolluscum Contagiosum Treatment OptionsShivani JainNessuna valutazione finora
- Obsgyn BooksDocumento4 pagineObsgyn BooksYulian NuswantoroNessuna valutazione finora
- PDF HM5 Adolescents HealthDocumento68 paginePDF HM5 Adolescents HealthYeli AstiNessuna valutazione finora
- Obsgyn BooksDocumento4 pagineObsgyn BooksYulian NuswantoroNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento13 pagineNIH Public Access: Author ManuscriptYeli AstiNessuna valutazione finora
- Tetanus BagusDocumento11 pagineTetanus BagusArief Yudho PrabowoNessuna valutazione finora
- Risk Factors For and Prevention of Human Papillomaviruses (HPV), Genital Warts and Cervical CancerDocumento9 pagineRisk Factors For and Prevention of Human Papillomaviruses (HPV), Genital Warts and Cervical CancerYeli AstiNessuna valutazione finora
- Validitas Sikap 1Documento4 pagineValiditas Sikap 1Yeli AstiNessuna valutazione finora
- Book 2Documento7 pagineBook 2Yeli AstiNessuna valutazione finora
- Dietary Consumption of Antioxidant Nutrients and Risk of Incident Cervical Intraepithelial NeoplasiaDocumento9 pagineDietary Consumption of Antioxidant Nutrients and Risk of Incident Cervical Intraepithelial NeoplasiaYeli AstiNessuna valutazione finora
- Dietary Consumption of Antioxidant Nutrients and Risk of Incident Cervical Intraepithelial NeoplasiaDocumento9 pagineDietary Consumption of Antioxidant Nutrients and Risk of Incident Cervical Intraepithelial NeoplasiaYeli AstiNessuna valutazione finora
- Tetanus BagusDocumento11 pagineTetanus BagusArief Yudho PrabowoNessuna valutazione finora
- Kanker ServiksDocumento16 pagineKanker ServiksYeli AstiNessuna valutazione finora
- Viaviliappendix1.Php FIGODocumento3 pagineViaviliappendix1.Php FIGOYeli AstiNessuna valutazione finora
- Hospital Preparedness For Emergency ResponseDocumento15 pagineHospital Preparedness For Emergency ResponseYeli AstiNessuna valutazione finora
- Hvi 8 355Documento8 pagineHvi 8 355Yeli AstiNessuna valutazione finora
- BMC Neurology: Autonomic Nervous System Dysfunction Predicts Poor Prognosis in Patients With Mild To Moderate TetanusDocumento4 pagineBMC Neurology: Autonomic Nervous System Dysfunction Predicts Poor Prognosis in Patients With Mild To Moderate TetanusYeli AstiNessuna valutazione finora
- Antioxidants in Cervical Cancer Chemopreventive and Chemotherapeutic Effects of PolyphenolsDocumento11 pagineAntioxidants in Cervical Cancer Chemopreventive and Chemotherapeutic Effects of PolyphenolsYeli AstiNessuna valutazione finora
- Tetanus BagusDocumento11 pagineTetanus BagusArief Yudho PrabowoNessuna valutazione finora
- Reproductive Morbidity Among Iranian Women Issues Often Inappropriately Addressed in Health Seeking BehaviorsDocumento8 pagineReproductive Morbidity Among Iranian Women Issues Often Inappropriately Addressed in Health Seeking BehaviorsYeli AstiNessuna valutazione finora
- Reproductive Morbidity Among Iranian Women Issues Often Inappropriately Addressed in Health Seeking BehaviorsDocumento8 pagineReproductive Morbidity Among Iranian Women Issues Often Inappropriately Addressed in Health Seeking BehaviorsYeli AstiNessuna valutazione finora
- BMC Neurology: Autonomic Nervous System Dysfunction Predicts Poor Prognosis in Patients With Mild To Moderate TetanusDocumento4 pagineBMC Neurology: Autonomic Nervous System Dysfunction Predicts Poor Prognosis in Patients With Mild To Moderate TetanusYeli AstiNessuna valutazione finora
- Sen, Gita y Östlin. Gender Inequity in Health, Why It Exists and How We Can Change It. 2008Documento14 pagineSen, Gita y Östlin. Gender Inequity in Health, Why It Exists and How We Can Change It. 2008Diana Paola Valencia CamachoNessuna valutazione finora
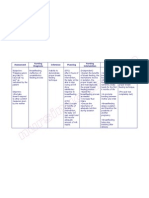
- Assessment Nursing Diagnosis Rationale Expected Outcome Nursing Interventions Rationale EvaluationDocumento1 paginaAssessment Nursing Diagnosis Rationale Expected Outcome Nursing Interventions Rationale EvaluationMark FernandezNessuna valutazione finora
- OBSTETRICS Enhancement - FINAL COPY 1Documento17 pagineOBSTETRICS Enhancement - FINAL COPY 1Jan Joseph BanzuelaNessuna valutazione finora
- Chlamydia TrachomatisDocumento7 pagineChlamydia TrachomatisDewi SetiawatiNessuna valutazione finora
- Case Study For Uterine-CancerDocumento9 pagineCase Study For Uterine-CancerGabbii CincoNessuna valutazione finora
- Malpresentations: Liji Raichel Kurian Dept of OBGDocumento41 pagineMalpresentations: Liji Raichel Kurian Dept of OBGliji raichel kurian100% (1)
- Opd SheetDocumento1 paginaOpd SheetTwingkol Just TwingkolNessuna valutazione finora
- Presentation-WPS OfficeDocumento47 paginePresentation-WPS OfficeJeffrey JasarenoNessuna valutazione finora
- Episiotomy Case and Postpartum HemorrhageDocumento2 pagineEpisiotomy Case and Postpartum HemorrhageRoni NurdiantoNessuna valutazione finora
- INCOMPETENT CER-WPS OfficeDocumento5 pagineINCOMPETENT CER-WPS OfficeRickNessuna valutazione finora
- The Role of Parity in The Mode of DeliveryDocumento11 pagineThe Role of Parity in The Mode of DeliveryKanuyasa GekzNessuna valutazione finora
- The Female Reproductive System: Paul F. Terranova, PH.DDocumento17 pagineThe Female Reproductive System: Paul F. Terranova, PH.DMekuriya BeregaNessuna valutazione finora
- Female Reproductive SystemDocumento2 pagineFemale Reproductive SystemVishesh KumarNessuna valutazione finora
- Womens Knowledge Regarding Symptoms of Menopause in Al Najaf CityDocumento9 pagineWomens Knowledge Regarding Symptoms of Menopause in Al Najaf CityakankshaNessuna valutazione finora
- The Use of Acupuncture With in Vitro Fertilization: Is There A Point?Documento10 pagineThe Use of Acupuncture With in Vitro Fertilization: Is There A Point?lu salviaNessuna valutazione finora
- Jurnal HPP TinaDocumento8 pagineJurnal HPP TinaShafa AnitasyahNessuna valutazione finora
- Prior Cesarean Delivery: 100 Years of ControversyDocumento17 paginePrior Cesarean Delivery: 100 Years of ControversyNoahYudhaNessuna valutazione finora
- 2.1 Assessment of Normal Pregnant MotherDocumento41 pagine2.1 Assessment of Normal Pregnant Mother11 - JEMELYN LOTERTENessuna valutazione finora
- 2.early Pregnancy and BleedingDocumento79 pagine2.early Pregnancy and BleedingjosephNessuna valutazione finora
- Superior Hypogastric Plexus Anatomy QuizDocumento4 pagineSuperior Hypogastric Plexus Anatomy QuizMaryneth EvangelistaNessuna valutazione finora
- HORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARSDocumento21 pagineHORMON REPRODUKSI DAN SIKLUS HAID Prof. Dr. Dr. Nusratuddin Abdullah, SP - OG (K) MARStenri olaNessuna valutazione finora