Potrebbero piacerti anche
- Leading 100 Billion Neurons - A journey into the brain and how this impacts business and leadershipDa EverandLeading 100 Billion Neurons - A journey into the brain and how this impacts business and leadershipNessuna valutazione finora
- 04: Prenatal CF Development IDocumento9 pagine04: Prenatal CF Development INYUCD17Nessuna valutazione finora
- Head & Neck Anatomy - Embryology & Pharyngeal Arches - INBDEDocumento13 pagineHead & Neck Anatomy - Embryology & Pharyngeal Arches - INBDEHạnh TrangNessuna valutazione finora
- 08 Cranio Development IVDocumento8 pagine08 Cranio Development IVNYUCD17Nessuna valutazione finora
- 09: Cranio Development VDocumento19 pagine09: Cranio Development VNYUCD17Nessuna valutazione finora
- The Maze WithinDocumento148 pagineThe Maze WithinDr Martyn Green100% (3)
- Basal Ganglia and Cerebellum Lecture - by Dr. SchiffDocumento12 pagineBasal Ganglia and Cerebellum Lecture - by Dr. SchiffNYUCD17Nessuna valutazione finora
- 1 - 2 - Module 1 (Neuroanatomy) - Part 1 - Learning Objectives and Overview of Neuroanatomy (27-46)Documento14 pagine1 - 2 - Module 1 (Neuroanatomy) - Part 1 - Learning Objectives and Overview of Neuroanatomy (27-46)Rodrigo Eberhart Musaio SommaNessuna valutazione finora
- Dr. David A. Sirois - We Left Off Yesterday Having Talked About Things That HappenedDocumento18 pagineDr. David A. Sirois - We Left Off Yesterday Having Talked About Things That HappenedNYUCD17Nessuna valutazione finora
- MCB80.2x V2 2k Optogenics V2FC JW - Edxmstr V1-30-EnDocumento9 pagineMCB80.2x V2 2k Optogenics V2FC JW - Edxmstr V1-30-EnAnina YangNessuna valutazione finora
- The Emerging Brain - Vilayanur S Ramachandran (BBC Radio 4 - Reith Lectures 2003)Documento67 pagineThe Emerging Brain - Vilayanur S Ramachandran (BBC Radio 4 - Reith Lectures 2003)ivanasena100% (1)
- Development, Nature & Nurture IDocumento25 pagineDevelopment, Nature & Nurture IAnda_Ilinca_BooksNessuna valutazione finora
- Meet The Gastrointestinal Tract! 3Documento12 pagineMeet The Gastrointestinal Tract! 3PsycOwl ꨄNessuna valutazione finora
- Embryology Article John WilksDocumento4 pagineEmbryology Article John Wilkspfi_jenNessuna valutazione finora
- Lesson Plan in Biology IiDocumento8 pagineLesson Plan in Biology IiPablo Ragay Jr100% (27)
- Science 6 Oct26 30 - Nervous System Part 2Documento9 pagineScience 6 Oct26 30 - Nervous System Part 2Pardeep DhillonNessuna valutazione finora
- Neuroscience Lecture 10 - Neurons by Dr. Jean-Pierre Saint-JeannetDocumento7 pagineNeuroscience Lecture 10 - Neurons by Dr. Jean-Pierre Saint-JeannetNYUCD17Nessuna valutazione finora
- Document 25Documento8 pagineDocument 25AroojNessuna valutazione finora
- Neuroscience Lecture 13 - Central Nervous System by Dr. Jean-Pierre Saint-JeannetDocumento10 pagineNeuroscience Lecture 13 - Central Nervous System by Dr. Jean-Pierre Saint-JeannetNYUCD17Nessuna valutazione finora
- TUCI Data Book V 2010.02 Babys Brain Begins Now.v2Documento12 pagineTUCI Data Book V 2010.02 Babys Brain Begins Now.v2George ManuNessuna valutazione finora
- Mitosis TranscriptDocumento2 pagineMitosis Transcriptesutch2535Nessuna valutazione finora
- 2 - The Brain#1Documento10 pagine2 - The Brain#1Nur Ain Faezah RoslanNessuna valutazione finora
- The Brain and Nervous SystemDocumento16 pagineThe Brain and Nervous SystemchristoftabosoNessuna valutazione finora
- Nervous SystemDocumento296 pagineNervous SystemDr. Serin KuriakoseNessuna valutazione finora
- Option A - Neurobiology and BehaviourDocumento29 pagineOption A - Neurobiology and Behaviour玛丽娜Nessuna valutazione finora
- 02 - CNS DevelopmentDocumento3 pagine02 - CNS DevelopmentCemre KuzeyNessuna valutazione finora
- Bio 109 Module 4Documento18 pagineBio 109 Module 4Marites Maylanon0% (1)
- Unit III Development and Plasticity of The BrainDocumento10 pagineUnit III Development and Plasticity of The Brainjusq marimarNessuna valutazione finora
- The Nervous SystemDocumento19 pagineThe Nervous SystemD.T. Wit, deNessuna valutazione finora
- Name: Cauilan, Darwin C. Score: Year and Section: Bs Pharma 1-A Set A DateDocumento4 pagineName: Cauilan, Darwin C. Score: Year and Section: Bs Pharma 1-A Set A DateDarwin CauilanNessuna valutazione finora
- Mrs Gren: Notes: Copy The Table Below Into Your Jotter. You Will Be GivenDocumento31 pagineMrs Gren: Notes: Copy The Table Below Into Your Jotter. You Will Be GivenknoxscienceNessuna valutazione finora
- Lecture: 5 - Brain and BehaviourDocumento28 pagineLecture: 5 - Brain and BehaviourAnoma ModakNessuna valutazione finora
- Vilayanur S. Ramachandran: The Emerging Mind-Reith LecturesDocumento70 pagineVilayanur S. Ramachandran: The Emerging Mind-Reith LecturesNadeem GrahamNessuna valutazione finora
- Assignment of Neurobehavioral ScienceDocumento6 pagineAssignment of Neurobehavioral ScienceAnza NoorNessuna valutazione finora
- Laporan Nbss ...Documento88 pagineLaporan Nbss ...Nita AndriyaniNessuna valutazione finora
- Development of Brain:: Spinal CordDocumento3 pagineDevelopment of Brain:: Spinal Cordhaseeb ShafaatNessuna valutazione finora
- Mind Machine Theme 1 Lecture 1Documento77 pagineMind Machine Theme 1 Lecture 1minerva_stanciuNessuna valutazione finora
- How To Use Mental Imagery For Any Clinical ConditionDocumento15 pagineHow To Use Mental Imagery For Any Clinical ConditionRaphael Soltoski100% (2)
- Embryology-Development of Central Nervous SystemDocumento28 pagineEmbryology-Development of Central Nervous Systemtenshi315Nessuna valutazione finora
- Lesson 3.Documento15 pagineLesson 3.Maedel Rose EsguerraNessuna valutazione finora
- Head and Neck. Embryology. Topographic RegionsDocumento56 pagineHead and Neck. Embryology. Topographic RegionsXerox medNessuna valutazione finora
- 33 HR 1 AsdadDocumento3 pagine33 HR 1 AsdadbingchillingNessuna valutazione finora
- Introduction To Biology 1Documento17 pagineIntroduction To Biology 1Samuel PonceNessuna valutazione finora
- Article EmbriologyDocumento6 pagineArticle Embriologycestrada10Nessuna valutazione finora
- Module 3 - Sensory NeuromarketingDocumento17 pagineModule 3 - Sensory NeuromarketinganaNessuna valutazione finora
- Antonio DamasioDocumento19 pagineAntonio Damasiosoho87100% (1)
- Chapter 9Documento28 pagineChapter 9AndriusjoNessuna valutazione finora
- Dr. Fresco GuideDocumento58 pagineDr. Fresco GuideItzaameth Moreno-AllenNessuna valutazione finora
- Sight Telepathy Your Eyes - More Than A CameraDocumento6 pagineSight Telepathy Your Eyes - More Than A CameraResmyrrandaNessuna valutazione finora
- ReithDocumento9 pagineReithshiva rahmanNessuna valutazione finora
- Embryology, Central Nervous System - StatPearls - NCBI BookshelfDocumento6 pagineEmbryology, Central Nervous System - StatPearls - NCBI Bookshelfleandro.silvaNessuna valutazione finora
- 1.7 WhatdoesbrainlooklikeDocumento1 pagina1.7 WhatdoesbrainlooklikeAdeyinkaNessuna valutazione finora
- 1.7 WhatdoesbrainlooklikeDocumento1 pagina1.7 WhatdoesbrainlooklikeAdeyinkaNessuna valutazione finora
- Neuro Clinica 1Documento70 pagineNeuro Clinica 1Pamela Tapia SandovalʚiɞNessuna valutazione finora
- Plexo BraquialDocumento26 paginePlexo BraquialXavier RiveraNessuna valutazione finora
- Brain Structures and Their Functions PDFDocumento26 pagineBrain Structures and Their Functions PDFNur Nashran Mahran100% (4)
- (ANA) Brachial Plexus IbookDocumento15 pagine(ANA) Brachial Plexus IbookRamses Dagoy100% (1)
- Material EnglishDocumento8 pagineMaterial EnglishnguyenquangyNessuna valutazione finora
- Fall Newsletter Nov 14Documento1 paginaFall Newsletter Nov 14NYUCD17Nessuna valutazione finora
- Happy: TurkeyDocumento8 pagineHappy: TurkeyNYUCD17Nessuna valutazione finora
- Reminders:: T Shirt Design Contes T!Documento1 paginaReminders:: T Shirt Design Contes T!NYUCD17Nessuna valutazione finora
- Fall Newsletter #3Documento1 paginaFall Newsletter #3NYUCD17Nessuna valutazione finora
- Week of November 30th, 2015 - Class of 2017 NewsletterDocumento9 pagineWeek of November 30th, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Happy: TurkeyDocumento8 pagineHappy: TurkeyNYUCD17Nessuna valutazione finora
- Week of September 12Documento1 paginaWeek of September 12NYUCD17Nessuna valutazione finora
- Week of September 5Documento1 paginaWeek of September 5NYUCD17Nessuna valutazione finora
- Week of October 19th, 2015 - Class of 2017 NewsletterDocumento9 pagineWeek of October 19th, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of October 26th, 2015 - Class of 2017 NewsletterDocumento9 pagineWeek of October 26th, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of November 2nd, 2015 - Class of 2017 NewsletterDocumento10 pagineWeek of November 2nd, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of November 9th, 2015 - Class of 2017 NewsletterDocumento9 pagineWeek of November 9th, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of October 5th, 2015 - Class of 2017 NewsletterDocumento8 pagineWeek of October 5th, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of September 8th - Class of 2017 NewsletterDocumento8 pagineWeek of September 8th - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of September 8th - Class of 2017 NewsletterDocumento8 pagineWeek of September 8th - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of September 14, 2015 - Class of 2017 NewsletterDocumento7 pagineWeek of September 14, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of September 21st, 2015 - Class of 2017 NewsletterDocumento8 pagineWeek of September 21st, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of September 28, 2015 - Class of 2017 NewsletterDocumento8 pagineWeek of September 28, 2015 - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- September 2, 2015 MinutesDocumento3 pagineSeptember 2, 2015 MinutesNYUCD17Nessuna valutazione finora
- Week of August 31st - Class of 2017 NewsletterDocumento7 pagineWeek of August 31st - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- Week of August 31st - Class of 2017 NewsletterDocumento7 pagineWeek of August 31st - Class of 2017 NewsletterNYUCD17Nessuna valutazione finora
- July 8, 2015 Meeting MinutesDocumento2 pagineJuly 8, 2015 Meeting MinutesNYUCD17Nessuna valutazione finora
- 2-20-15 MinutesDocumento2 pagine2-20-15 MinutesNYUCD17Nessuna valutazione finora
- September 2, 2015 MinutesDocumento3 pagineSeptember 2, 2015 MinutesNYUCD17Nessuna valutazione finora
- 10-17-14 MinutesDocumento2 pagine10-17-14 MinutesNYUCD17Nessuna valutazione finora
- D2 Council Meeting Minutes: 12:00 - 1:00pm Room 8SDocumento3 pagineD2 Council Meeting Minutes: 12:00 - 1:00pm Room 8SNYUCD17Nessuna valutazione finora
- 1-9-15 MinutesDocumento3 pagine1-9-15 MinutesNYUCD17Nessuna valutazione finora
- 1-23-15 MinutesDocumento2 pagine1-23-15 MinutesNYUCD17Nessuna valutazione finora
- Macleod - S - Clinical - Examination - 15th NeuroDocumento18 pagineMacleod - S - Clinical - Examination - 15th Neurowxyngtc4n9Nessuna valutazione finora
- Zanki Neuro BoldedDocumento25 pagineZanki Neuro Boldedsmian08Nessuna valutazione finora
- The Brain and Cranial NervesDocumento82 pagineThe Brain and Cranial NervesImmanuel Ronald LewisNessuna valutazione finora
- MCQS CNS-1Documento5 pagineMCQS CNS-1Umer Ahmad100% (1)
- Cns QuestionsDocumento8 pagineCns QuestionsSyed HussainNessuna valutazione finora
- Burton Hunt Pony Club: Quiz 2021Documento25 pagineBurton Hunt Pony Club: Quiz 2021api-306398192Nessuna valutazione finora
- Middle Cerebral ArteryDocumento4 pagineMiddle Cerebral Arterykat9210Nessuna valutazione finora
- Clinical Approach To QuadriplegiaDocumento11 pagineClinical Approach To QuadriplegiaUmesh BabuNessuna valutazione finora
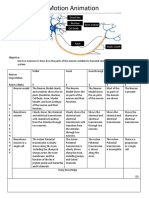
- Neurons Stop Motion AnimationDocumento2 pagineNeurons Stop Motion Animationapi-495006167Nessuna valutazione finora
- Multiple Choice Questions: Control of Body MovementDocumento20 pagineMultiple Choice Questions: Control of Body MovementwanderagroNessuna valutazione finora
- Central Nervous System OVL ANA 2103Documento76 pagineCentral Nervous System OVL ANA 2103Baguma MichaelNessuna valutazione finora
- 19 Neuromuscular DisordersDocumento39 pagine19 Neuromuscular DisordersSara 'Yaa SaraaNessuna valutazione finora
- Radial Nerve Palsy: ReferatDocumento13 pagineRadial Nerve Palsy: ReferatFrilia Elri BotilangiNessuna valutazione finora
- Nervous System (Fundamental & Central Questions)Documento13 pagineNervous System (Fundamental & Central Questions)Mohammed Morsy AlsherifNessuna valutazione finora
- Functional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Documento465 pagineFunctional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Eduardo RodriguezNessuna valutazione finora
- Autonomic Nervous SystemDocumento83 pagineAutonomic Nervous SystemChaudhry F MasoodNessuna valutazione finora
- Extrasegmental Acupuncture Points and Autonomic FunctionDocumento2 pagineExtrasegmental Acupuncture Points and Autonomic FunctionTrung Hiệp ĐàoNessuna valutazione finora
- Posterior Column-Medial Lemniscus PathwayDocumento4 paginePosterior Column-Medial Lemniscus PathwayRachmadina Basyarial BasyaruddinNessuna valutazione finora
- CVADocumento116 pagineCVAkathy100% (1)
- Pathophysiology of Peripheral Nerve InjuryDocumento12 paginePathophysiology of Peripheral Nerve Injuryblack_eagelNessuna valutazione finora
- Case Study of Bacterial MeningitisDocumento125 pagineCase Study of Bacterial MeningitisNap IchNessuna valutazione finora
- 430 MCQ Team: Nervous System BlockDocumento10 pagine430 MCQ Team: Nervous System BlockAhmadAlHajjhassanNessuna valutazione finora
- Tutorilas On Ascending Tracts of The Spinal CordDocumento7 pagineTutorilas On Ascending Tracts of The Spinal CordanojanNessuna valutazione finora
- Jinnah Sindh Medical University NERVOUS SYSTEM-1, MBBS Year-2, 2021Documento4 pagineJinnah Sindh Medical University NERVOUS SYSTEM-1, MBBS Year-2, 2021Mushtaq GajooNessuna valutazione finora
- Effective SLPDocumento10 pagineEffective SLPRené Ignacio Guzmán SalgadoNessuna valutazione finora
- The Nervous System: Elaine N. MariebDocumento92 pagineThe Nervous System: Elaine N. MariebhamidiNessuna valutazione finora
- Somatosensory System OkDocumento47 pagineSomatosensory System OkIrayumastutiNessuna valutazione finora
- Motor Neuron DiseasesDocumento103 pagineMotor Neuron DiseasesJamil AhmadNessuna valutazione finora
- Raeders SyndromeDocumento6 pagineRaeders SyndromeSundayperfectNessuna valutazione finora