Potrebbero piacerti anche
- Madeleine LeiningerDocumento2 pagineMadeleine LeiningerAnonymous 75TDy2yNessuna valutazione finora
- M.leininger ArticleDocumento6 pagineM.leininger ArticleAldrin Ian Oraza AlpeNessuna valutazione finora
- New Orem TheoryDocumento58 pagineNew Orem Theoryริดิ พูตรา100% (1)
- Nursing TheoriesDocumento83 pagineNursing TheoriesIvan OlivaNessuna valutazione finora
- Self Care Defisit Nursing TheoryDocumento9 pagineSelf Care Defisit Nursing TheoryiswantoNessuna valutazione finora
- Women and Occupational HealthDocumento12 pagineWomen and Occupational Healthniju_grgNessuna valutazione finora
- Impacts of Parenting Practices To The Academic Behavior of Grade 12 Stem Students of Cor Jesu CoDocumento8 pagineImpacts of Parenting Practices To The Academic Behavior of Grade 12 Stem Students of Cor Jesu CoMaxenia Fabores100% (1)
- Basic Principles of Nursing Care Volina ContinueDocumento2 pagineBasic Principles of Nursing Care Volina Continuealena volinaNessuna valutazione finora
- Examples of Abdellah's Publications: TestabilityDocumento3 pagineExamples of Abdellah's Publications: TestabilityleewfNessuna valutazione finora
- Pamela G ReedDocumento3 paginePamela G ReedGabNessuna valutazione finora
- The Benefits of Attachment Parenting For Infants and Children: A Behavioral Developmental ViewDocumento14 pagineThe Benefits of Attachment Parenting For Infants and Children: A Behavioral Developmental Viewda5id665Nessuna valutazione finora
- Learning Theories 1Documento8 pagineLearning Theories 1api-258761055Nessuna valutazione finora
- Manuscript Martha RogersDocumento8 pagineManuscript Martha Rogersnotyourvincent kNessuna valutazione finora
- Imogene KingDocumento3 pagineImogene KingKarl AcuñaNessuna valutazione finora
- Orem's TheoryDocumento40 pagineOrem's TheoryREVATHI H KNessuna valutazione finora
- Community Health NursingDocumento27 pagineCommunity Health NursingKhatlen Bagares100% (1)
- Basic Principles of NursingDocumento23 pagineBasic Principles of Nursingpumpkin21100% (1)
- Human BecomingDocumento3 pagineHuman BecomingCharles DaveNessuna valutazione finora
- Nursing Theory: Dr. Waleed SagironDocumento23 pagineNursing Theory: Dr. Waleed SagironABHA,M-ALI MOHAMMDNessuna valutazione finora
- Swanson - Tee, GammadDocumento9 pagineSwanson - Tee, GammadCheiramina Serolc EetNessuna valutazione finora
- Human Becoming TheoryDocumento23 pagineHuman Becoming TheorykeiNessuna valutazione finora
- Spirituality in Healthcare: Perspectives for Innovative PracticeDa EverandSpirituality in Healthcare: Perspectives for Innovative PracticeNessuna valutazione finora
- Application - of - Theory - in - NursingDocumento9 pagineApplication - of - Theory - in - Nursingako at ang exo100% (1)
- Marthe Elizabeth RogersDocumento17 pagineMarthe Elizabeth RogersKristan Keith EcoNessuna valutazione finora
- Class Presentation On 1. Human Becoming Theory and 2. Health As Expanding Consciousness TheoryDocumento60 pagineClass Presentation On 1. Human Becoming Theory and 2. Health As Expanding Consciousness TheoryBheru LalNessuna valutazione finora
- Nursing TheoryDocumento12 pagineNursing TheorydrsabuegNessuna valutazione finora
- 3 Determinants of LearningDocumento6 pagine3 Determinants of LearningKenNessuna valutazione finora
- A. Nursing in IndiaDocumento118 pagineA. Nursing in IndiaAnuchithra RadhakrishnanNessuna valutazione finora
- Faye Glenn Abdellah Ppt. PresentationDocumento14 pagineFaye Glenn Abdellah Ppt. PresentationRhyne AsuncionNessuna valutazione finora
- Kolcaba's Theory of ComfortDocumento1 paginaKolcaba's Theory of ComfortDanette Mae RocNessuna valutazione finora
- Nursing As An Art: CaringDocumento58 pagineNursing As An Art: CaringZeus CabungcalNessuna valutazione finora
- Ida Jean OrlandoDocumento32 pagineIda Jean OrlandoVinia A. VillanuevaNessuna valutazione finora
- PROFESSIONALISM in The Community Health NurseDocumento35 paginePROFESSIONALISM in The Community Health NurseKristin Jones100% (1)
- Virginia HendersonDocumento18 pagineVirginia Hendersonthoughts ofloveNessuna valutazione finora
- Futuristic NursingDocumento11 pagineFuturistic NursingRoxana Mihaela MâțuNessuna valutazione finora
- Rozzano LocsinDocumento12 pagineRozzano LocsinTANYA CUBENessuna valutazione finora
- A Report On Imogene KingDocumento17 pagineA Report On Imogene KingRibelyne loise AquisioNessuna valutazione finora
- History of NursingDocumento8 pagineHistory of NursingNazareth Narisma PatindolNessuna valutazione finora
- Caring and The Professional Practice of NursingDocumento4 pagineCaring and The Professional Practice of NursingGalihPioNessuna valutazione finora
- Orem's and Levine'TheoryDocumento15 pagineOrem's and Levine'TheoryTrisha Bawa100% (2)
- Health Promotion ModelDocumento12 pagineHealth Promotion ModelMarjorie BelanteNessuna valutazione finora
- Factors Affecting Student Nurses' Willingness To Care For Patients With HIV AIDSDocumento14 pagineFactors Affecting Student Nurses' Willingness To Care For Patients With HIV AIDSGabz GabbyNessuna valutazione finora
- Joyce Travelbee - Human-to-Human Relationship ModelDocumento3 pagineJoyce Travelbee - Human-to-Human Relationship ModelVictoria Castillo TamayoNessuna valutazione finora
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionDa EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionNessuna valutazione finora
- Faye Glenn AbdellahDocumento31 pagineFaye Glenn AbdellahMikz JocomNessuna valutazione finora
- Neumans TheoryDocumento26 pagineNeumans Theoryimam trisutrisnoNessuna valutazione finora
- Behavioral System Model by Dorothy JohnsonDocumento2 pagineBehavioral System Model by Dorothy JohnsonyoeanneNessuna valutazione finora
- Module 1 Lesson 1Documento37 pagineModule 1 Lesson 1John Dave V. Villarmente100% (1)
- Psy - Nursing Care Plan - Therapeutic CommunicationDocumento6 paginePsy - Nursing Care Plan - Therapeutic CommunicationCarmen Angela DusaranNessuna valutazione finora
- Reed Self-Transcendence TheoryDocumento2 pagineReed Self-Transcendence TheoryTrae StewartNessuna valutazione finora
- Unit 1 Intro Chap I Chap 2Documento75 pagineUnit 1 Intro Chap I Chap 2Aurora Mae Amores100% (1)
- PDF DocumentDocumento36 paginePDF DocumentSuji MerlineNessuna valutazione finora
- Reflection From Orem's TheoryDocumento2 pagineReflection From Orem's Theoryริดิ พูตราNessuna valutazione finora
- Theories of Nursing PracticeDocumento2 pagineTheories of Nursing PracticeShanilyn BiongNessuna valutazione finora
- Preparation and Education for Parenthood: A Pathway to Understanding the Carer's Role in Infant EducationDa EverandPreparation and Education for Parenthood: A Pathway to Understanding the Carer's Role in Infant EducationValutazione: 5 su 5 stelle5/5 (1)
- Abdellah's TheoryDocumento14 pagineAbdellah's Theoryanon_387100722100% (1)
- St. Anthony'S College - Nursing Department: Theoretical Foundations in NursingDocumento86 pagineSt. Anthony'S College - Nursing Department: Theoretical Foundations in NursingCandido Kenneth JohnNessuna valutazione finora
- Betty Neuman Final SlidesDocumento19 pagineBetty Neuman Final Slidesreymart bolagaoNessuna valutazione finora
- TFN Theories OutlineDocumento6 pagineTFN Theories Outlineleviona halfNessuna valutazione finora
- WSC Customer Service Guide Nov2012Documento58 pagineWSC Customer Service Guide Nov2012catislandbigredNessuna valutazione finora
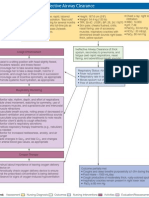
- Concept Map: Ineffective Airway ClearanceDocumento1 paginaConcept Map: Ineffective Airway ClearanceNikki Beverly G. BacaleNessuna valutazione finora
- Adult Nursing Practicum VerbalDocumento2 pagineAdult Nursing Practicum VerbalcatislandbigredNessuna valutazione finora
- PneumoniaDocumento9 paginePneumoniaManuel SalamancaNessuna valutazione finora
- Physical AssessmentDocumento10 paginePhysical AssessmentcatislandbigredNessuna valutazione finora
- The BahamasDocumento66 pagineThe BahamascatislandbigredNessuna valutazione finora
- New Nanda 2012 To 2014Documento11 pagineNew Nanda 2012 To 2014catislandbigredNessuna valutazione finora
- How To Write An AnalysisDocumento2 pagineHow To Write An AnalysiscatislandbigredNessuna valutazione finora
- Sims Life StoryDocumento1 paginaSims Life StorycatislandbigredNessuna valutazione finora
- What Is Schizophrenia?Documento4 pagineWhat Is Schizophrenia?catislandbigredNessuna valutazione finora
- Attribution TheoryDocumento2 pagineAttribution TheorycatislandbigredNessuna valutazione finora
- Flow of Aqueous Humor of The EyeDocumento1 paginaFlow of Aqueous Humor of The EyecatislandbigredNessuna valutazione finora
- Nursing Care Plans For Delusional DisorderDocumento4 pagineNursing Care Plans For Delusional Disorderkirill61195% (22)
- Wound Care Teaching Plan Sample PDFDocumento1 paginaWound Care Teaching Plan Sample PDFcatislandbigredNessuna valutazione finora
- Surgical Asepsis 3 in The or - HTMDocumento67 pagineSurgical Asepsis 3 in The or - HTMcatislandbigredNessuna valutazione finora
- New Nanda 2012 To 2014Documento11 pagineNew Nanda 2012 To 2014catislandbigredNessuna valutazione finora
- Cholinergics and AnticholinergicsDocumento5 pagineCholinergics and AnticholinergicscatislandbigredNessuna valutazione finora
- Brochure How To BreastfeedDocumento2 pagineBrochure How To BreastfeedEmman Acosta Domingcil100% (1)
- A Teachers Guide To HydrocephalusDocumento29 pagineA Teachers Guide To HydrocephaluscatislandbigredNessuna valutazione finora
- Below Knee Amputation, BKADocumento1 paginaBelow Knee Amputation, BKAcatislandbigred100% (2)
- Cranial NervesDocumento2 pagineCranial NervescatislandbigredNessuna valutazione finora
- Intravenous Therapy PDFDocumento4 pagineIntravenous Therapy PDFcatislandbigredNessuna valutazione finora
- Nodal Analysis Collection 2Documento21 pagineNodal Analysis Collection 2Manoj ManmathanNessuna valutazione finora
- Fabric DefectsDocumento30 pagineFabric Defectsaparna_ftNessuna valutazione finora
- Service Manual: NISSAN Automobile Genuine AM/FM Radio 6-Disc CD Changer/ Cassette DeckDocumento26 pagineService Manual: NISSAN Automobile Genuine AM/FM Radio 6-Disc CD Changer/ Cassette DeckEduardo Reis100% (1)
- Policy Implementation NotesDocumento17 paginePolicy Implementation NoteswubeNessuna valutazione finora
- Mastering American EnglishDocumento120 pagineMastering American Englishmarharnwe80% (10)
- Actara (5 24 01) PDFDocumento12 pagineActara (5 24 01) PDFBand Dvesto Plus CrepajaNessuna valutazione finora
- Detailed Lesson Plan in Mathematics (Pythagorean Theorem)Documento6 pagineDetailed Lesson Plan in Mathematics (Pythagorean Theorem)Carlo DascoNessuna valutazione finora
- La La Mei Seaside Resto BAR: Final PlateDocumento4 pagineLa La Mei Seaside Resto BAR: Final PlateMichael Ken FurioNessuna valutazione finora
- EIL 6-51-0051-Rev 06 - 1.1kv-Xlpe - Dimension Cat - B Armour-BbpDocumento2 pagineEIL 6-51-0051-Rev 06 - 1.1kv-Xlpe - Dimension Cat - B Armour-BbpShubham BaderiyaNessuna valutazione finora
- Vicente BSC2-4 WhoamiDocumento3 pagineVicente BSC2-4 WhoamiVethinaVirayNessuna valutazione finora
- Data SheetDocumento14 pagineData SheetAnonymous R8ZXABkNessuna valutazione finora
- Libel Arraignment Pre Trial TranscriptDocumento13 pagineLibel Arraignment Pre Trial TranscriptAnne Laraga LuansingNessuna valutazione finora
- 1Documento14 pagine1Cecille GuillermoNessuna valutazione finora
- MGT403 Slide All ChaptersDocumento511 pagineMGT403 Slide All Chaptersfarah aqeelNessuna valutazione finora
- Risk Management: Questions and AnswersDocumento5 pagineRisk Management: Questions and AnswersCentauri Business Group Inc.Nessuna valutazione finora
- ADP G2 Spreadsheet Loader Data Entry: End-User GuideDocumento48 pagineADP G2 Spreadsheet Loader Data Entry: End-User Guideraokumar250% (2)
- Embedded System Lab ManualDocumento67 pagineEmbedded System Lab Manualsaim100% (1)
- BSBSTR602 Project PortfolioDocumento16 pagineBSBSTR602 Project Portfoliocruzfabricio0Nessuna valutazione finora
- EQUIP9-Operations-Use Case ChallengeDocumento6 pagineEQUIP9-Operations-Use Case ChallengeTushar ChaudhariNessuna valutazione finora
- Rules of Bursa Malaysia Securities Clearing 2019Documento11 pagineRules of Bursa Malaysia Securities Clearing 2019Evelyn SeethaNessuna valutazione finora
- Trading Rules To Successful ProfitsDocumento89 pagineTrading Rules To Successful ProfitsOuattaraNessuna valutazione finora
- The Abcs of Edi: A Comprehensive Guide For 3Pl Warehouses: White PaperDocumento12 pagineThe Abcs of Edi: A Comprehensive Guide For 3Pl Warehouses: White PaperIgor SangulinNessuna valutazione finora
- SchedulingDocumento47 pagineSchedulingKonark PatelNessuna valutazione finora
- Aryan Civilization and Invasion TheoryDocumento60 pagineAryan Civilization and Invasion TheorySaleh Mohammad Tarif 1912343630Nessuna valutazione finora
- HAI ROBOTICS Introduction ENV2022.0829 MarketingDocumento40 pagineHAI ROBOTICS Introduction ENV2022.0829 MarketingKit WooNessuna valutazione finora
- Study of Employees Performance Appraisal System in Hindustan Unilever LimitedDocumento9 pagineStudy of Employees Performance Appraisal System in Hindustan Unilever LimitedSimranjitNessuna valutazione finora
- New Regular and Irregular Verb List and Adjectives 1-Ix-2021Documento11 pagineNew Regular and Irregular Verb List and Adjectives 1-Ix-2021MEDALITH ANEL HUACRE SICHANessuna valutazione finora
- Evolution of Management AccountingDocumento35 pagineEvolution of Management AccountingNuqiah Fathiah Seri100% (1)
- Video ObservationDocumento8 pagineVideo Observationapi-532202065Nessuna valutazione finora
- Basics of Petroleum GeologyDocumento23 pagineBasics of Petroleum GeologyShahnawaz MustafaNessuna valutazione finora