Potrebbero piacerti anche
- Knowledge, Attitude, and Practices About Biomedical Waste Management Among Healthcare Personnel: A Cross-Sectional StudyDocumento5 pagineKnowledge, Attitude, and Practices About Biomedical Waste Management Among Healthcare Personnel: A Cross-Sectional StudyLa RikiNessuna valutazione finora
- 25 Leena EtalDocumento6 pagine25 Leena EtaleditorijmrhsNessuna valutazione finora
- Healthcare waste management in Ethiopian health centersDocumento9 pagineHealthcare waste management in Ethiopian health centersash amenNessuna valutazione finora
- Lampiran Artikel IlmiahDocumento25 pagineLampiran Artikel IlmiahAii CNessuna valutazione finora
- Unsafe Injection Practices IJHAS 2015Documento5 pagineUnsafe Injection Practices IJHAS 2015nagojedaNessuna valutazione finora
- Ajol File Journals - 56 - Articles - 62960 - Submission - Proof - 62960 661 120699 1 10 20101216Documento8 pagineAjol File Journals - 56 - Articles - 62960 - Submission - Proof - 62960 661 120699 1 10 20101216Soliarega BekeleNessuna valutazione finora
- Knowledge and Attitude of Rational Use of Antibiotics Among General Practitioners, Khartoum Locality, SudanDocumento8 pagineKnowledge and Attitude of Rational Use of Antibiotics Among General Practitioners, Khartoum Locality, SudanInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Paparan Kerja Terhadap Jarum Tertusuk Dan Cedera TajamDocumento7 paginePaparan Kerja Terhadap Jarum Tertusuk Dan Cedera Tajamshofia andriNessuna valutazione finora
- Who Core Prescribing Indicators and Its Effects On Quality of Life in Patients With Superficial Fungal InfectionsDocumento11 pagineWho Core Prescribing Indicators and Its Effects On Quality of Life in Patients With Superficial Fungal InfectionsIJAR JOURNALNessuna valutazione finora
- Healthcare Waste Generation and Its Management System THDocumento8 pagineHealthcare Waste Generation and Its Management System THmoosNessuna valutazione finora
- WHO Point Prevalence Survey To Describe The Use of Antimicrobials at A Tertiary Care Center in Pakistan - A Situation Analysis For Establishing An Antimicrobial Stewardship Program - PMCDocumento18 pagineWHO Point Prevalence Survey To Describe The Use of Antimicrobials at A Tertiary Care Center in Pakistan - A Situation Analysis For Establishing An Antimicrobial Stewardship Program - PMCAbubakr AurangzebNessuna valutazione finora
- Self-Medication Pattern of Antibiotics Among The People of Imphal West District of Manipur, IndiaDocumento8 pagineSelf-Medication Pattern of Antibiotics Among The People of Imphal West District of Manipur, IndiaIJAR JOURNALNessuna valutazione finora
- A Study: Biomedical Waste Management in India: Kirti Mishra, Anurag Sharma, Sarita, Shahnaz AyubDocumento4 pagineA Study: Biomedical Waste Management in India: Kirti Mishra, Anurag Sharma, Sarita, Shahnaz AyubIOSRjournalNessuna valutazione finora
- Antibiotics 11 00791 v2Documento16 pagineAntibiotics 11 00791 v2Retno WahyuningrumNessuna valutazione finora
- Biomedical Waste Management A Study of Knowledge Attitude and Practice Among Health Care Personnel at Tertiary Care Hospital in RajkotDocumento7 pagineBiomedical Waste Management A Study of Knowledge Attitude and Practice Among Health Care Personnel at Tertiary Care Hospital in Rajkotparta anantamaNessuna valutazione finora
- Sustainability 09 00604Documento14 pagineSustainability 09 00604Nidhi AshokNessuna valutazione finora
- Kumpulan Jurnal InternasionalDocumento15 pagineKumpulan Jurnal InternasionalTIKANessuna valutazione finora
- KNOWLDGEOFSANITORYWORKERSDocumento2 pagineKNOWLDGEOFSANITORYWORKERS083 Sneha KumariNessuna valutazione finora
- Assessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesDocumento9 pagineAssessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesAl ANessuna valutazione finora
- 118815-Article Text-328262-1-10-20150630Documento9 pagine118815-Article Text-328262-1-10-20150630Essay helpNessuna valutazione finora
- 08kharirohijphsjun16 Edit-With-Cover-Page-V2Documento7 pagine08kharirohijphsjun16 Edit-With-Cover-Page-V2Godeliva AdrianiNessuna valutazione finora
- Monitoring The Implementation of The WHO Global Code of Practice On The International Recruitment of Health Personnel: The Case of IndonesiaDocumento63 pagineMonitoring The Implementation of The WHO Global Code of Practice On The International Recruitment of Health Personnel: The Case of IndonesiaFerry EfendiNessuna valutazione finora
- Critical Care Nurses' Knowledge and Practices about Toxicological EmergenciesDocumento16 pagineCritical Care Nurses' Knowledge and Practices about Toxicological EmergenciesSmith MpNessuna valutazione finora
- Sengupta Et Al 2021 Challenges Encountered by Healthcare Providers in Covid 19 Times An Exploratory StudyDocumento18 pagineSengupta Et Al 2021 Challenges Encountered by Healthcare Providers in Covid 19 Times An Exploratory StudyLongjam HerojitNessuna valutazione finora
- JHMI - Volume 3 - Issue 2 - Pages 51-56Documento6 pagineJHMI - Volume 3 - Issue 2 - Pages 51-56elys marselinaNessuna valutazione finora
- Access To Antibiotics in New Delhi, India: Implications For Antibiotic PolicyDocumento13 pagineAccess To Antibiotics in New Delhi, India: Implications For Antibiotic PolicyMahadi Hasan KhanNessuna valutazione finora
- N Engg - Ijget - Biomedical - D. Shreedevi - Dual - IjgmpDocumento11 pagineN Engg - Ijget - Biomedical - D. Shreedevi - Dual - Ijgmpiaset123Nessuna valutazione finora
- Medical Device Landscape For Communicable and Noncommunicable Diseases in Low-Income CountriesDocumento6 pagineMedical Device Landscape For Communicable and Noncommunicable Diseases in Low-Income CountriesSkiil ExNessuna valutazione finora
- Utilization of Primary Health Care Services in Rural and Urban Areas in ShirazDocumento10 pagineUtilization of Primary Health Care Services in Rural and Urban Areas in ShirazNamarig IzzaldinNessuna valutazione finora
- Sarani2015Documento6 pagineSarani2015Mastifa HanasitaNessuna valutazione finora
- Assessment of Healthcare Professional Awareness Towards Haemovigilance (HvPI) Programme of India in South IndiaDocumento5 pagineAssessment of Healthcare Professional Awareness Towards Haemovigilance (HvPI) Programme of India in South IndiaIOSRjournalNessuna valutazione finora
- Weaknesses in ethical review systems and the need for harmonization of international biomedical research standardsDocumento4 pagineWeaknesses in ethical review systems and the need for harmonization of international biomedical research standardsSudhakar DasariNessuna valutazione finora
- His 2Documento253 pagineHis 2Anjum100% (3)
- Sado2017 PDFDocumento5 pagineSado2017 PDFTommy Winahyu PuriNessuna valutazione finora
- Charan2021 Article UseOfComplementaryAndAlternatiDocumento4 pagineCharan2021 Article UseOfComplementaryAndAlternatiMohamad Wahyudin Y. AhmadNessuna valutazione finora
- Assignment With NotesDocumento12 pagineAssignment With NotesAnonymous zXwP003Nessuna valutazione finora
- EJHM - Volume 81 - Issue 3 - Pages 1621-1627Documento7 pagineEJHM - Volume 81 - Issue 3 - Pages 1621-1627Alexandru Codrin-IonutNessuna valutazione finora
- Bio Medical WasteDocumento6 pagineBio Medical Wastekritishah299750% (6)
- Icmr PharmaDocumento7 pagineIcmr Pharmakavya chagantiNessuna valutazione finora
- Analysis of The Healthcare Waste Management Status in Tehran HospitalsDocumento6 pagineAnalysis of The Healthcare Waste Management Status in Tehran HospitalsHusainNessuna valutazione finora
- Motivation, Supervision, and Adherence To Medical Waste Policy in South Labuhanbatu, North SumateraDocumento6 pagineMotivation, Supervision, and Adherence To Medical Waste Policy in South Labuhanbatu, North Sumaterakristina dewiNessuna valutazione finora
- 2-Article Text-128-2-10-20200328Documento8 pagine2-Article Text-128-2-10-20200328Siti HamsyiahNessuna valutazione finora
- Mental Health Impacts Among HealthDocumento12 pagineMental Health Impacts Among HealthAshish ParajuliNessuna valutazione finora
- Special Issue 1 3Documento129 pagineSpecial Issue 1 3Amit PasiNessuna valutazione finora
- Final EPHA & JOSI IPCDocumento44 pagineFinal EPHA & JOSI IPCephrembz33Nessuna valutazione finora
- Patient Satisfaction With Healthcare Services: A Bangladesh ScenarioDocumento8 paginePatient Satisfaction With Healthcare Services: A Bangladesh ScenarioA. K. MohiuddinNessuna valutazione finora
- Mscano,+jidc 015 1117Documento8 pagineMscano,+jidc 015 1117dr.lakshmiseth5Nessuna valutazione finora
- Health Care Waste Management Practice in A HospitalDocumento5 pagineHealth Care Waste Management Practice in A HospitalRekha SinghNessuna valutazione finora
- Improving The Healthcare Response To Domestic Violence and Abuse in UK Primary Care: Interrupted Time Series Evaluation of A System-Level Training and Support ProgrammeDocumento10 pagineImproving The Healthcare Response To Domestic Violence and Abuse in UK Primary Care: Interrupted Time Series Evaluation of A System-Level Training and Support ProgrammePatrick SanchezNessuna valutazione finora
- Factors Affecting The Physical Activity of Healthcare Workers of Iran University of Medical Sciences: A Qualitative StudyDocumento11 pagineFactors Affecting The Physical Activity of Healthcare Workers of Iran University of Medical Sciences: A Qualitative StudySalvador L. Jr. CruzNessuna valutazione finora
- GJHS 7 341Documento17 pagineGJHS 7 341mandeep kaurNessuna valutazione finora
- Self-Medication Practice and Associated Factors Among Residents in Wuhan, ChinaDocumento10 pagineSelf-Medication Practice and Associated Factors Among Residents in Wuhan, ChinaDanielle De GuzmanNessuna valutazione finora
- P3 Health StatusDocumento9 pagineP3 Health StatusNovita Mariani GlekoNessuna valutazione finora
- Lei 2018 PDFDocumento10 pagineLei 2018 PDFPare KemangNessuna valutazione finora
- Interventions To Improve Hand Hygiene Compliance in Emergency Departments: A Systematic ReviewDocumento13 pagineInterventions To Improve Hand Hygiene Compliance in Emergency Departments: A Systematic ReviewFaozan FikriNessuna valutazione finora
- African Diaspora Satisfaction with Medical Care in IndiaDocumento46 pagineAfrican Diaspora Satisfaction with Medical Care in IndiaDeep ChoudharyNessuna valutazione finora
- Antimicrobial StewardshipDocumento19 pagineAntimicrobial StewardshipFelipe VicenteñoNessuna valutazione finora
- HIV Patients Retention and Attrition in Care and Determinants in EthiopiaDocumento24 pagineHIV Patients Retention and Attrition in Care and Determinants in EthiopiaDouglas ChukwuNessuna valutazione finora
- Status of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiDocumento8 pagineStatus of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiSagaram ShashidarNessuna valutazione finora
- Adolescent Morbidity Mortality in An Indian Hospital According To ICD (WHO) 10 ClassificationDocumento6 pagineAdolescent Morbidity Mortality in An Indian Hospital According To ICD (WHO) 10 ClassificationfriendsofindiaNessuna valutazione finora
- Leprosy LEM SURVEY 2004 IndiaDocumento75 pagineLeprosy LEM SURVEY 2004 IndiafriendsofindiaNessuna valutazione finora
- Retinoblastoma Childhood Cancer Trend Hospital Registry IndiaDocumento2 pagineRetinoblastoma Childhood Cancer Trend Hospital Registry IndiafriendsofindiaNessuna valutazione finora
- HIV/AIDS Awareness Knowledge Amongst Mothers Residing in Slums of South Delhi, IndiaDocumento1 paginaHIV/AIDS Awareness Knowledge Amongst Mothers Residing in Slums of South Delhi, IndiafriendsofindiaNessuna valutazione finora
- Cold Chain Vaccine Status Delhi IndiaDocumento2 pagineCold Chain Vaccine Status Delhi IndiafriendsofindiaNessuna valutazione finora
- Injection Practices in Urban Dispensary Delhi IndiaDocumento1 paginaInjection Practices in Urban Dispensary Delhi IndiafriendsofindiaNessuna valutazione finora
- Seasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiaDocumento92 pagineSeasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiafriendsofindiaNessuna valutazione finora
- Ophthalmology in Service Training Public Sector NPCB IndiaDocumento3 pagineOphthalmology in Service Training Public Sector NPCB IndiafriendsofindiaNessuna valutazione finora
- Medical Tourism IndiaDocumento3 pagineMedical Tourism IndiafriendsofindiaNessuna valutazione finora
- CATARACT Surgery Season Month Wise Reported Figure in IndiaDocumento5 pagineCATARACT Surgery Season Month Wise Reported Figure in IndiafriendsofindiaNessuna valutazione finora
- Eye DonationEnglishDocumento1 paginaEye DonationEnglishAnonymous x8fY69CrnNessuna valutazione finora
- TB Malnutrition IndiaDocumento2 pagineTB Malnutrition IndiafriendsofindiaNessuna valutazione finora
- Community Ophthalmology IndiaDocumento3 pagineCommunity Ophthalmology IndiafriendsofindiaNessuna valutazione finora
- Vitamin A Supplement Coverage Children Slums Delhi IndiaDocumento5 pagineVitamin A Supplement Coverage Children Slums Delhi IndiafriendsofindiaNessuna valutazione finora
- Blindness Rehabilitation IndiaDocumento6 pagineBlindness Rehabilitation IndiafriendsofindiaNessuna valutazione finora
- National Blindness Control Program of India During 11 Five Year Plan PeriodDocumento2 pagineNational Blindness Control Program of India During 11 Five Year Plan PeriodfriendsofindiaNessuna valutazione finora
- Asthease CapsuleDocumento3 pagineAsthease Capsulehk_scribdNessuna valutazione finora
- Occlusal Variations For Reconstructing The Natural DentitionDocumento5 pagineOcclusal Variations For Reconstructing The Natural DentitionPablo Gutiérrez Da VeneziaNessuna valutazione finora
- Contact IsolationDocumento2 pagineContact IsolationIsworo RukmiNessuna valutazione finora
- Khat Factsheet - 020914 PDFDocumento2 pagineKhat Factsheet - 020914 PDFMohammedOumerNessuna valutazione finora
- 3Documento2 pagine3imtiyazh85100% (1)
- Medicine Lec.9 - Viral Infection IIDocumento42 pagineMedicine Lec.9 - Viral Infection II7fefdfbea1Nessuna valutazione finora
- FCADocumento34 pagineFCAElvira BasilioNessuna valutazione finora
- Philippine Health Care Providers Vs Commissioner of Internal Revenue 554 SCRA 411Documento9 paginePhilippine Health Care Providers Vs Commissioner of Internal Revenue 554 SCRA 411Clarinda MerleNessuna valutazione finora
- Contents - Part 1: 1 Infection Control Strategy 1-1Documento51 pagineContents - Part 1: 1 Infection Control Strategy 1-1Arie KusumodewiNessuna valutazione finora
- Terapi Seft Spiritual Emotional Freedom TechniqueDocumento7 pagineTerapi Seft Spiritual Emotional Freedom TechniqueWiwik AristianiNessuna valutazione finora
- Name: Ala Sami Mahmoud Abusohyon Nationality: Jordanian: ObjectiveDocumento4 pagineName: Ala Sami Mahmoud Abusohyon Nationality: Jordanian: Objectiveamr ahmedNessuna valutazione finora
- NCP DRDocumento3 pagineNCP DRRhuwelyn Parantar PilapilNessuna valutazione finora
- JHSPH Prospectus WebDocumento76 pagineJHSPH Prospectus WebAyodeji SamuelsNessuna valutazione finora
- 2.3 Ferry Indriasmoko - CCA Overview Jogja 8AUG19Documento12 pagine2.3 Ferry Indriasmoko - CCA Overview Jogja 8AUG19Netty HerawatiNessuna valutazione finora
- PPT-cigarette SQUID GAME TEMPLATEDocumento26 paginePPT-cigarette SQUID GAME TEMPLATERuby Ann TerolNessuna valutazione finora
- M. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingDocumento11 pagineM. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingMallika JoonNessuna valutazione finora
- Essential Newborn Care: The DOH/WHO ProtocolDocumento21 pagineEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubNessuna valutazione finora
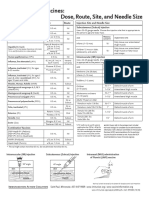
- Injection Site and Needle Size Vaccine Dose RouteDocumento1 paginaInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNessuna valutazione finora
- Fetal Echocardiography: Scope, Cardiac Development & AbnormalitiesDocumento28 pagineFetal Echocardiography: Scope, Cardiac Development & Abnormalitiesmerin sunilNessuna valutazione finora
- Six SigmaDocumento4 pagineSix SigmaPrateik BhasinNessuna valutazione finora
- Lesson 1 Physical FitnessDocumento9 pagineLesson 1 Physical FitnessLIMOS JR. ROMEO P.Nessuna valutazione finora
- Chapter 24: Injury Prevention and Child Maltreatment Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocumento2 pagineChapter 24: Injury Prevention and Child Maltreatment Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNessuna valutazione finora
- Santi-Total Thesis Title - Upto June 2017Documento37 pagineSanti-Total Thesis Title - Upto June 2017SRIKANTA MAJINessuna valutazione finora
- Metformin Use in Polycystic Ovary Syndrome (PCOS)Documento2 pagineMetformin Use in Polycystic Ovary Syndrome (PCOS)matasatuNessuna valutazione finora
- CV Maggies - HungDocumento4 pagineCV Maggies - HungDoni HardiansyahNessuna valutazione finora
- Kaviyarasan Visitor PassDocumento7 pagineKaviyarasan Visitor PassTRISTAR TEKZONENessuna valutazione finora
- Dermatology Secrets Plus 4th Edition ReviewDocumento1 paginaDermatology Secrets Plus 4th Edition ReviewYoga Adi0% (2)
- Mapeh 4Documento4 pagineMapeh 4Joanna Mae ArmasNessuna valutazione finora
- Mission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstDocumento20 pagineMission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstJayeshAgrawalNessuna valutazione finora
- Ordering Lab Tests: Alphabetical List of TestsDocumento3 pagineOrdering Lab Tests: Alphabetical List of TestsDjdjjd SiisusNessuna valutazione finora