Potrebbero piacerti anche
- Evidence For A Rapid Release of Carbon at The Paleocene-Eocene Thermal MaximumDocumento6 pagineEvidence For A Rapid Release of Carbon at The Paleocene-Eocene Thermal MaximumJohn StrohlNessuna valutazione finora
- Solar Initiative July 2015 Fact SheetDocumento9 pagineSolar Initiative July 2015 Fact SheetJohn StrohlNessuna valutazione finora
- Local Food Systems Panel Draft White PaperDocumento23 pagineLocal Food Systems Panel Draft White PaperJohn StrohlNessuna valutazione finora
- Foods For The Gerson DietDocumento6 pagineFoods For The Gerson DietKAMAL BEHLNessuna valutazione finora
- Final Presentation BhutanDocumento25 pagineFinal Presentation BhutanJohn StrohlNessuna valutazione finora
- Savory Spiced Lamb PieDocumento4 pagineSavory Spiced Lamb PieJohn StrohlNessuna valutazione finora
- Food System Challenges for Health and SustainabilityDocumento27 pagineFood System Challenges for Health and SustainabilityJohn StrohlNessuna valutazione finora
- Building Sustainable Farms, Ranches, & CommunitiesDocumento88 pagineBuilding Sustainable Farms, Ranches, & CommunitiesJohn StrohlNessuna valutazione finora
- The Placebo EffectDocumento2 pagineThe Placebo EffectJohn StrohlNessuna valutazione finora
- Cooking For The Gerson TherapyDocumento4 pagineCooking For The Gerson TherapyJohn StrohlNessuna valutazione finora
- Chicken Tortilla SoupDocumento6 pagineChicken Tortilla SoupJohn StrohlNessuna valutazione finora
- 4 1⁄2 Inch Metal Cutting Bandsaw Assembly GuideDocumento15 pagine4 1⁄2 Inch Metal Cutting Bandsaw Assembly GuideJohn StrohlNessuna valutazione finora
- Ancient Amazonian Healing Secrets Revealed in New eBookDocumento29 pagineAncient Amazonian Healing Secrets Revealed in New eBookjoel100% (1)
- ConOps Grants - GovDocumento23 pagineConOps Grants - GovJohn StrohlNessuna valutazione finora
- Homelessness Risk AnalysisDocumento1 paginaHomelessness Risk AnalysisJohn StrohlNessuna valutazione finora
- Mapping Business ProcessDocumento11 pagineMapping Business ProcessJohn StrohlNessuna valutazione finora
- Homelessness Risk AnalysisDocumento1 paginaHomelessness Risk AnalysisJohn StrohlNessuna valutazione finora
- Classifications SchemaDocumento54 pagineClassifications SchemaJohn StrohlNessuna valutazione finora
- Orientation Booklet 2012Documento26 pagineOrientation Booklet 2012John StrohlNessuna valutazione finora
- Industrial Hemp Double DividendDocumento11 pagineIndustrial Hemp Double DividendJohn StrohlNessuna valutazione finora
- Ohio Senior Farmers Market Program ApplicationDocumento2 pagineOhio Senior Farmers Market Program ApplicationJohn StrohlNessuna valutazione finora
- Vocal Trainer VT 12 BrochureDocumento3 pagineVocal Trainer VT 12 BrochureJohn StrohlNessuna valutazione finora
- Retirement Consumption: Insights From A SurveyDocumento27 pagineRetirement Consumption: Insights From A SurveyJohn StrohlNessuna valutazione finora
- Why Being The Most Connected Is A Vanity Metric - ForbesDocumento7 pagineWhy Being The Most Connected Is A Vanity Metric - ForbesJohn StrohlNessuna valutazione finora
- CMM Methanol ProductionDocumento3 pagineCMM Methanol ProductionJohn StrohlNessuna valutazione finora
- Getting Started With ENVI: ENVI Versions 4.7 and 4.7 SP1 December, 2009 EditionDocumento234 pagineGetting Started With ENVI: ENVI Versions 4.7 and 4.7 SP1 December, 2009 EditionJohn StrohlNessuna valutazione finora
- GFSC Community-Village Project - Project SkeletonDocumento22 pagineGFSC Community-Village Project - Project SkeletonJohn StrohlNessuna valutazione finora
- Human-Animal Bonds 1:the Relational Significance of Companion AnimalsDocumento20 pagineHuman-Animal Bonds 1:the Relational Significance of Companion AnimalsJohn StrohlNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Medical RealDocumento1 paginaMedical Realapi-252555369Nessuna valutazione finora
- Mrs. Manjushree NayakDocumento3 pagineMrs. Manjushree NayakAkashNachraniNessuna valutazione finora
- Doccument PDFDocumento2 pagineDoccument PDFDigvijay NagareNessuna valutazione finora
- Antenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DDocumento32 pagineAntenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DzaaaidaNessuna valutazione finora
- November 2017Documento12 pagineNovember 2017Cornwall and Isles of Scilly LMCNessuna valutazione finora
- Asma AmbreenDocumento1 paginaAsma Ambreenambreenasma33Nessuna valutazione finora
- Dental Career PathsDocumento4 pagineDental Career Pathsrd8Nessuna valutazione finora
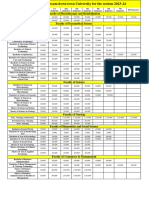
- Fees Structure Assam Down Town University For The Session 2023 2Documento2 pagineFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaNessuna valutazione finora
- 1) Community PharmacyDocumento17 pagine1) Community PharmacyDr. Zirwa AsimNessuna valutazione finora
- Ayushman Bharat PMJAY Branding GuidelinesDocumento10 pagineAyushman Bharat PMJAY Branding GuidelinesalkaNessuna valutazione finora
- RPRH Accomplishment Report 1stsem2022Documento9 pagineRPRH Accomplishment Report 1stsem2022Rose Martinez BayNessuna valutazione finora
- Case Study Project: Elective - Healthcare & Hospital ManagementDocumento2 pagineCase Study Project: Elective - Healthcare & Hospital ManagementlucasNessuna valutazione finora
- Cns 736 Assignment 2Documento2 pagineCns 736 Assignment 2api-664836263Nessuna valutazione finora
- Sederer Expert Report Publicly FiledDocumento157 pagineSederer Expert Report Publicly FiledBrit StackNessuna valutazione finora
- Philippine Clinical Practice Guidelines On The Diagnosis andDocumento83 paginePhilippine Clinical Practice Guidelines On The Diagnosis andREnren ConsolNessuna valutazione finora
- Asanthe Case WorkingsDocumento9 pagineAsanthe Case Workingsazhar hussainNessuna valutazione finora
- Report On Patient Satisfaction and Waiting TimeDocumento35 pagineReport On Patient Satisfaction and Waiting TimeRohit SharmaNessuna valutazione finora
- Post Mortem CareDocumento2 paginePost Mortem Carebea pegadNessuna valutazione finora
- NCMB317 RUBRICS Mental Status ExaminationDocumento1 paginaNCMB317 RUBRICS Mental Status Examinationkpbalay5921pamNessuna valutazione finora
- UIC NetworklistDocumento563 pagineUIC NetworklistKriti KumariNessuna valutazione finora
- Soft Copy of Activity Manual Supply Chain Management MedicineDocumento40 pagineSoft Copy of Activity Manual Supply Chain Management MedicineRyanNessuna valutazione finora
- Selection List 174316Documento860 pagineSelection List 174316kishor rathodNessuna valutazione finora
- Gongadze ClinTher.13pdfDocumento2 pagineGongadze ClinTher.13pdfEdisher TsivtsivadzeNessuna valutazione finora
- AILYNDocumento98 pagineAILYNArvin EstebanNessuna valutazione finora
- Blockchain in Healthcare: Guangjian Huang, Abdullah Al FoysalDocumento14 pagineBlockchain in Healthcare: Guangjian Huang, Abdullah Al Foysalshubham thkNessuna valutazione finora
- PHAP311 Reviewer Short BondpaperDocumento11 paginePHAP311 Reviewer Short Bondpaperlingadanne1103Nessuna valutazione finora
- Reaction Paper On COVID-19Documento2 pagineReaction Paper On COVID-19Kiarana Fleischer67% (3)
- Introduction To SOAP NotesDocumento23 pagineIntroduction To SOAP Notestsaokw83% (6)
- NEW m1m2 Reporting FormDocumento24 pagineNEW m1m2 Reporting FormDeyeck Verga100% (8)
- Suvarnaprashana Therapy in Children ConcDocumento3 pagineSuvarnaprashana Therapy in Children ConcBhavana GangurdeNessuna valutazione finora