Potrebbero piacerti anche
- Acute Cardiac Care PDFDocumento43 pagineAcute Cardiac Care PDFhuong LNessuna valutazione finora
- Role of Physiotherapy in ICUDocumento68 pagineRole of Physiotherapy in ICUprasanna3k100% (2)
- Noninvasive VentilationDocumento6 pagineNoninvasive VentilationEma MagfirahNessuna valutazione finora
- Rapid Sequence Intubation: BackgroundDocumento8 pagineRapid Sequence Intubation: Backgroundmarsh86Nessuna valutazione finora
- Intensive Care Unit (ICU) Manual 2020-21Documento146 pagineIntensive Care Unit (ICU) Manual 2020-21anithaNessuna valutazione finora
- Mechanical VentilatorDocumento9 pagineMechanical VentilatorAnusha Verghese100% (2)
- Laparoscopic CholecystectomyDocumento41 pagineLaparoscopic CholecystectomyLim MelaniNessuna valutazione finora
- Care of Patients With Mechanical VentilatorDocumento4 pagineCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- Optional (AEMT), Optional (Paramedic)Documento76 pagineOptional (AEMT), Optional (Paramedic)Mark ReinhardtNessuna valutazione finora
- Noninvasive Ventilation in Acute Respiratory Failure in AdultsDocumento12 pagineNoninvasive Ventilation in Acute Respiratory Failure in AdultsferrevNessuna valutazione finora
- Ventilator Care 1Documento11 pagineVentilator Care 1Friends ForeverNessuna valutazione finora
- Acapella ProtocolDocumento3 pagineAcapella ProtocolRTdadNessuna valutazione finora
- Laryngofissure TechniqueDocumento5 pagineLaryngofissure TechniqueJamesNessuna valutazione finora
- Ventilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDocumento12 pagineVentilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDellNessuna valutazione finora
- Chapter 29: Nursing Management: Obstructive Pulmonary Diseases Test BankDocumento15 pagineChapter 29: Nursing Management: Obstructive Pulmonary Diseases Test BankBriseidaSolisNessuna valutazione finora
- AnswersDocumento4 pagineAnswersKhadijah AhmedNessuna valutazione finora
- BTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Documento21 pagineBTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Madalina TalpauNessuna valutazione finora
- Id 1300Documento11 pagineId 1300ShadowruneNessuna valutazione finora
- AARC Clinical Practice Guideline: Intermittent Positive Pressure Breathing-2003 Revision & UpdateDocumento7 pagineAARC Clinical Practice Guideline: Intermittent Positive Pressure Breathing-2003 Revision & UpdategiiasNessuna valutazione finora
- Intermittent Positive Pressure Breathing (IPPB) PDFDocumento10 pagineIntermittent Positive Pressure Breathing (IPPB) PDFKellie PacanowskiNessuna valutazione finora
- Mechanical Ventilation and Noninvasive Ventilatory SupportDocumento30 pagineMechanical Ventilation and Noninvasive Ventilatory Supportdr.baselnassarNessuna valutazione finora
- Cpap Use in OSA 2005Documento12 pagineCpap Use in OSA 2005Davi LopesNessuna valutazione finora
- Weaning Ventilator Protocol For LiberationDocumento3 pagineWeaning Ventilator Protocol For LiberationBonny ChristianNessuna valutazione finora
- Adult NebuliserDocumento13 pagineAdult NebuliserBeh Boon CongNessuna valutazione finora
- Authors: Section Editor: Deputy EditorDocumento27 pagineAuthors: Section Editor: Deputy EditorIacriNessuna valutazione finora
- CG00932 High Frequency Oscillatory Ventilation HFOV of Neonates Using SLE5000 Ventilator PDFDocumento5 pagineCG00932 High Frequency Oscillatory Ventilation HFOV of Neonates Using SLE5000 Ventilator PDFNajam Ul QadirNessuna valutazione finora
- Thorax 2016BTS/ICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults Davidson Ii1 Ii35Documento36 pagineThorax 2016BTS/ICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults Davidson Ii1 Ii35danelvNessuna valutazione finora
- ITU Handbook For Non-Anaesthetists 214Documento23 pagineITU Handbook For Non-Anaesthetists 214AtikaNessuna valutazione finora
- Oxygen AdministrationDocumento29 pagineOxygen Administrationjembut300100% (2)
- Anaesthesia For Thoracic Surgery: DR Fazal H KhanDocumento4 pagineAnaesthesia For Thoracic Surgery: DR Fazal H KhanAdeebMutawaNessuna valutazione finora
- Critical Care Therapy and Respiratory Care Section: 1.0 DescriptionDocumento7 pagineCritical Care Therapy and Respiratory Care Section: 1.0 DescriptionLenny Ronalyn QuitorianoNessuna valutazione finora
- Therapeutics - para COVID - Junho 2020 - HavardDocumento28 pagineTherapeutics - para COVID - Junho 2020 - HavardRenato GrinbaumNessuna valutazione finora
- Nebuliser - Care of Your NebuliserDocumento13 pagineNebuliser - Care of Your NebuliserRahulNargotraNessuna valutazione finora
- Jerath2020 Article InhalationalVolatile-basedSedaDocumento4 pagineJerath2020 Article InhalationalVolatile-basedSedasncr.gnyNessuna valutazione finora
- Physiotherapy Guidelines For Manual HyperinflationDocumento5 paginePhysiotherapy Guidelines For Manual HyperinflationAhmed Abd Elrauf100% (2)
- Critical Care Therapy and Respiratory Care Section: 1.0 DescriptionDocumento7 pagineCritical Care Therapy and Respiratory Care Section: 1.0 DescriptionStefano Ignacio Valenzano FigueroaNessuna valutazione finora
- Summary of The Physiologically Difficult Airway - André FerreiraDocumento2 pagineSummary of The Physiologically Difficult Airway - André FerreiracedivadeniaNessuna valutazione finora
- Manual Hyperinflation MhiDocumento5 pagineManual Hyperinflation Mhijainy12Nessuna valutazione finora
- Induced SputumDocumento6 pagineInduced Sputumnh2411Nessuna valutazione finora
- Failure of Weaning:: According To The European Respiratory Society (ERS) Task ForceDocumento12 pagineFailure of Weaning:: According To The European Respiratory Society (ERS) Task ForceAmr El Taher0% (1)
- Federal Democratic Republic of Ethiopia Ministry of HealthDocumento43 pagineFederal Democratic Republic of Ethiopia Ministry of HealthdagemNessuna valutazione finora
- 4.-Rapid Sequence Intubation in Adults - Uptodate PDFDocumento14 pagine4.-Rapid Sequence Intubation in Adults - Uptodate PDFkendramura100% (1)
- NIV TeachingDocumento12 pagineNIV TeachingZahraa Al-MayahiNessuna valutazione finora
- DefaultDocumento37 pagineDefaultBayan Abu AlrubNessuna valutazione finora
- Weaning IndicesDocumento28 pagineWeaning IndicesSri HarshaNessuna valutazione finora
- Copd BipapDocumento9 pagineCopd BipapjabeedNessuna valutazione finora
- Papazian2022 Article PronePositionInMechanicallyVenDocumento4 paginePapazian2022 Article PronePositionInMechanicallyVenA. RaufNessuna valutazione finora
- Oxygen TherapyDocumento85 pagineOxygen Therapyvictoria.nickola3404Nessuna valutazione finora
- Comparison Sheet Based On 2010 AHA Guidelines For CPR and ECC BLS ChangesDocumento5 pagineComparison Sheet Based On 2010 AHA Guidelines For CPR and ECC BLS ChangesCupit NubillisNessuna valutazione finora
- Sas 6Documento5 pagineSas 6Rodesa MigarNessuna valutazione finora
- Kali Bichromicum 30C For COPD 2005Documento8 pagineKali Bichromicum 30C For COPD 2005Dr. Nancy MalikNessuna valutazione finora
- Early Initiation MV 2017 - DR - TrisnaDocumento34 pagineEarly Initiation MV 2017 - DR - TrisnaHappy ShalalaNessuna valutazione finora
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Documento7 pagineManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNessuna valutazione finora
- Mechanical Ventilation: Standard Weaning Criteria (Respiratory Therapy)Documento6 pagineMechanical Ventilation: Standard Weaning Criteria (Respiratory Therapy)S3DOSHA osmanNessuna valutazione finora
- SEC5 BodyDocumento15 pagineSEC5 BodyAdel HamadaNessuna valutazione finora
- Vap Care Bundle FinalDocumento4 pagineVap Care Bundle FinalMother of Mercy Hospital -Tacloban Inc.Nessuna valutazione finora
- Average Volume-Assured Pressure Support - StatPearls - NCBI BookshelfDocumento8 pagineAverage Volume-Assured Pressure Support - StatPearls - NCBI BookshelfmohammedNessuna valutazione finora
- Bustamante, Anjaneth C. Bsrtp-3ADocumento13 pagineBustamante, Anjaneth C. Bsrtp-3AMite giteNessuna valutazione finora
- Volume 1 CorrectedDocumento145 pagineVolume 1 Corrected897829Nessuna valutazione finora
- Mechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaDocumento55 pagineMechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaElaine IsalosNessuna valutazione finora
- Mechanical VentilationDocumento40 pagineMechanical VentilationPratik SahooNessuna valutazione finora
- Acute Respiratory Distress Syndrome Ventilator Management Strategies For AdultsDocumento36 pagineAcute Respiratory Distress Syndrome Ventilator Management Strategies For Adultsleokadiobarroso.rjNessuna valutazione finora
- Essentials in Lung TransplantationDa EverandEssentials in Lung TransplantationAllan R. GlanvilleNessuna valutazione finora
- BIRADSDocumento94 pagineBIRADSSergio MoralesNessuna valutazione finora
- Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Documento7 pagineBasic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Rizki YuliantoNessuna valutazione finora
- CUVASLARDocumento21 pagineCUVASLARKristal MartinezNessuna valutazione finora
- Operative ObstetricsDocumento4 pagineOperative Obstetricssarguss14100% (3)
- Dr. Shailesh Shevale SynopsisDocumento29 pagineDr. Shailesh Shevale Synopsisshewale59Nessuna valutazione finora
- He Pat EctomyDocumento4 pagineHe Pat Ectomysharjil chaudhryNessuna valutazione finora
- Presentation For Rotary Club of Dhaka BurigangaDocumento44 paginePresentation For Rotary Club of Dhaka Burigangaprince323Nessuna valutazione finora
- Dog Dissection ProcedureDocumento20 pagineDog Dissection ProcedureChristine Joyce NavarroNessuna valutazione finora
- MS UrologyDocumento73 pagineMS UrologyZeeshan AliNessuna valutazione finora
- Family Planning: Natural MethodDocumento5 pagineFamily Planning: Natural MethodAngelaNessuna valutazione finora
- Radiology Report 2300985Documento4 pagineRadiology Report 2300985JyotiNessuna valutazione finora
- Ulcerative ColitisDocumento18 pagineUlcerative ColitisKyle Ü D. CunanersNessuna valutazione finora
- 1843 FullDocumento123 pagine1843 FullKevin KnightsNessuna valutazione finora
- سويرولاكبلا ةلمحل يعاعشلإا ريوصتلا ناحتما Radiography Technology Bachelor Degree (Bsc Exam Number: (Bsc-C)Documento8 pagineسويرولاكبلا ةلمحل يعاعشلإا ريوصتلا ناحتما Radiography Technology Bachelor Degree (Bsc Exam Number: (Bsc-C)Nuhad Bou MoslehNessuna valutazione finora
- Description:: Materials/ Equipment NeededDocumento6 pagineDescription:: Materials/ Equipment NeededMarc Renz R. ChanNessuna valutazione finora
- UntitledDocumento2 pagineUntitledAelysa PabloNessuna valutazione finora
- Neck TrianglesDocumento6 pagineNeck TrianglesJay-arh SebusaNessuna valutazione finora
- Budget Plan Wound ClinicDocumento4 pagineBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- ER & CCU ProtocolDocumento14 pagineER & CCU ProtocolatinafansifNessuna valutazione finora
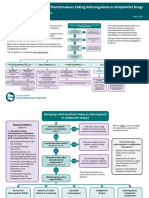
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocumento5 pagineSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNessuna valutazione finora
- Fabian VentilatorDocumento17 pagineFabian VentilatorRohana AnaNessuna valutazione finora
- Mechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalDocumento1 paginaMechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalscudchssNessuna valutazione finora
- Regenerative Peripheral Nerve Interface Surgery .27Documento9 pagineRegenerative Peripheral Nerve Interface Surgery .27Magdalena MajNessuna valutazione finora
- RENR MOCK EXAMINATION 2 2018. Question SheetDocumento24 pagineRENR MOCK EXAMINATION 2 2018. Question SheetSasha UterNessuna valutazione finora
- Prolapsed Intervertebral DiscDocumento12 pagineProlapsed Intervertebral DiscElvisNessuna valutazione finora
- AuscultationDocumento41 pagineAuscultationAnonymous ZUaUz1wwNessuna valutazione finora