Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Medicare Part B Premium Fact SheetDocumento2 pagineMedicare Part B Premium Fact SheetTerry PetersonNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Bylaws of SCGC - 2010Documento17 pagineBylaws of SCGC - 2010Terry PetersonNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- 2010-04-02 - Health Care Reform ArticleDocumento4 pagine2010-04-02 - Health Care Reform ArticleTerry PetersonNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
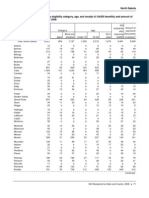
- ND SSI StatsDocumento2 pagineND SSI StatsTerry PetersonNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- IRWE Request TemplateDocumento3 pagineIRWE Request TemplateTerry PetersonNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- IM 5062 ATTACHED CHART 2009 Medicaid Income Level Chart - Effective 04-01-09Documento2 pagineIM 5062 ATTACHED CHART 2009 Medicaid Income Level Chart - Effective 04-01-09Terry Peterson100% (1)
- Fy09 DFC Final RfaDocumento99 pagineFy09 DFC Final RfaTerry Peterson100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- BPQY Release 90508 Final IIDocumento2 pagineBPQY Release 90508 Final IITerry PetersonNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Earnings Release 82508 (1) - MarkDocumento1 paginaEarnings Release 82508 (1) - MarkTerry PetersonNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- BPQY Release 90508 Final IIDocumento2 pagineBPQY Release 90508 Final IITerry PetersonNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Earnings Release 82508 (1) - MarkDocumento1 paginaEarnings Release 82508 (1) - MarkTerry PetersonNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Deeming Chart 2009Documento1 paginaDeeming Chart 2009Terry Peterson100% (3)
- BPQY Release 90808 #1Documento1 paginaBPQY Release 90808 #1Terry PetersonNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Earnings Release 82508 #2Documento1 paginaEarnings Release 82508 #2Terry PetersonNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Risk-Based IA Planning - Important ConsiderationsDocumento14 pagineRisk-Based IA Planning - Important ConsiderationsRajitha LakmalNessuna valutazione finora
- Freelance Contract TemplateDocumento7 pagineFreelance Contract TemplateAkhil PCNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Document 20Documento3 pagineDocument 20api-586815209Nessuna valutazione finora
- Descriptive Na Ly TicsDocumento112 pagineDescriptive Na Ly TicsJay Mart AvanceñaNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- AMCHAM Press ReleaseDocumento1 paginaAMCHAM Press ReleaseAnonymous FnM14a0Nessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Resume (Suyash Garg)Documento1 paginaResume (Suyash Garg)Suyash GargNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- KL1508 KL1516: 8/16-Port Cat 5 High-Density Dual Rail LCD KVM SwitchDocumento5 pagineKL1508 KL1516: 8/16-Port Cat 5 High-Density Dual Rail LCD KVM SwitchnisarahmedgfecNessuna valutazione finora
- University of Nottingham Department of Architecture and Built EnvironmentDocumento43 pagineUniversity of Nottingham Department of Architecture and Built EnvironmentDaniahNessuna valutazione finora
- Digitalisasi Alquran-1 PDFDocumento40 pagineDigitalisasi Alquran-1 PDFMohammad Zildan Pasyha MNessuna valutazione finora
- Astm A 478 - 97Documento2 pagineAstm A 478 - 97neno2405Nessuna valutazione finora
- MC 33199Documento12 pagineMC 33199Abbode HoraniNessuna valutazione finora
- Q3 Week 1 Homeroom Guidance JGRDocumento9 pagineQ3 Week 1 Homeroom Guidance JGRJasmin Goot Rayos50% (4)
- Shear Wall Design PDFDocumento9 pagineShear Wall Design PDFjk.dasgupta100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Blockchain Technology in The Banking SectorDocumento2 pagineBlockchain Technology in The Banking Sectorvaralakshmi aNessuna valutazione finora
- Evaluation of Performance of Container Terminals T PDFDocumento10 pagineEvaluation of Performance of Container Terminals T PDFjohnNessuna valutazione finora
- Pfmar SampleDocumento15 paginePfmar SampleJustin Briggs86% (7)
- Kolodin Agreement For Discipline by ConsentDocumento21 pagineKolodin Agreement For Discipline by ConsentJordan ConradsonNessuna valutazione finora
- E14r50p01 800 MhaDocumento4 pagineE14r50p01 800 Mha'Theodora GeorgianaNessuna valutazione finora
- Tankguard AR: Technical Data SheetDocumento5 pagineTankguard AR: Technical Data SheetAzar SKNessuna valutazione finora
- Longley Rice PropagationDocumento11 pagineLongley Rice Propagationy_m_algbaliNessuna valutazione finora
- All About Ignition Coils: Technical InformationDocumento15 pagineAll About Ignition Coils: Technical InformationTrương Ngọc ThắngNessuna valutazione finora
- Transport Phenomena 18.4.CDocumento3 pagineTransport Phenomena 18.4.CDelyana RatnasariNessuna valutazione finora
- 50 Hotelierstalk MinDocumento16 pagine50 Hotelierstalk MinPadma SanthoshNessuna valutazione finora
- ReleaseNoteRSViewME 5 10 02Documento12 pagineReleaseNoteRSViewME 5 10 02Jose Luis Chavez LunaNessuna valutazione finora
- AFAR Problems PrelimDocumento11 pagineAFAR Problems PrelimLian Garl100% (8)
- Steinway Case - CH 03Documento5 pagineSteinway Case - CH 03Twēéty TuiñkleNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- ANNEX C LIST OF EXCEPTIONS (Non-Disslosure of Information)Documento3 pagineANNEX C LIST OF EXCEPTIONS (Non-Disslosure of Information)ryujinxxcastorNessuna valutazione finora
- CH 2 How LAN and WAN Communications WorkDocumento60 pagineCH 2 How LAN and WAN Communications WorkBeans GaldsNessuna valutazione finora
- 1. Cẩm Nang Sửa Chữa Hệ Thống Điện Xe Honda Civic 2012Documento138 pagine1. Cẩm Nang Sửa Chữa Hệ Thống Điện Xe Honda Civic 2012Ngọc NamNessuna valutazione finora
- UK LL M Thesis - Builders' Liability in UK Law Under TortDocumento16 pagineUK LL M Thesis - Builders' Liability in UK Law Under TortRajan UppiliNessuna valutazione finora