Potrebbero piacerti anche
- Industrial TrainingDocumento21 pagineIndustrial TrainingVinamra MittalNessuna valutazione finora
- Price Schedule - Industrial Gases 49009Documento22 paginePrice Schedule - Industrial Gases 49009AloneNessuna valutazione finora
- Gas Cylinder SafetyDocumento5 pagineGas Cylinder SafetyS C GaurNessuna valutazione finora
- Cylinder Filling PlantDocumento67 pagineCylinder Filling PlantPassmore Dube100% (1)
- Industrial GasesDocumento776 pagineIndustrial GasesvasucristalNessuna valutazione finora
- High-Purity Oxygen Production Using Mixed Ionic-Electronic Conduc PDFDocumento108 pagineHigh-Purity Oxygen Production Using Mixed Ionic-Electronic Conduc PDFJason MandelaNessuna valutazione finora
- Biomedical New Hire OrientationDocumento29 pagineBiomedical New Hire OrientationBEJOYNessuna valutazione finora
- Medical GasDocumento39 pagineMedical GasFrancisco M. Ramos100% (1)
- Medical and Laboratory Gas Pipeline Design Part 1Documento3 pagineMedical and Laboratory Gas Pipeline Design Part 1karunaNessuna valutazione finora
- CALGAZ Test Gases Calibration Gas PDFDocumento33 pagineCALGAZ Test Gases Calibration Gas PDFdavidjoe77Nessuna valutazione finora
- Endex Fittings CatalougeDocumento64 pagineEndex Fittings Catalougeeslam mahfouzNessuna valutazione finora
- ANSI Pipe Marking StandardsDocumento2 pagineANSI Pipe Marking StandardsSupawat RangsiwongNessuna valutazione finora
- VV PPM C AaaaaaaaaaDocumento32 pagineVV PPM C AaaaaaaaaaAlessio DeOsimoNessuna valutazione finora
- Biogas SystemsDocumento8 pagineBiogas SystemsvedpathakNessuna valutazione finora
- Price Schedule - CUAGAS2016 Industrial GasesDocumento7 paginePrice Schedule - CUAGAS2016 Industrial GasesAloneNessuna valutazione finora
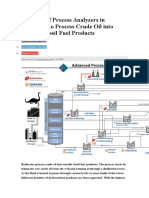
- Analyzers in RefineriesDocumento5 pagineAnalyzers in RefineriesGuillermoNessuna valutazione finora
- 13X DatasheetDocumento3 pagine13X Datasheetdrizzt299Nessuna valutazione finora
- Oxygen Cylinder Safety: Do NotDocumento1 paginaOxygen Cylinder Safety: Do NotMahammadNessuna valutazione finora
- Elsmt01d 0604Documento3 pagineElsmt01d 0604danorcNessuna valutazione finora
- Pneumatic NotesDocumento5 paginePneumatic NoteskanscseNessuna valutazione finora
- Uses and Applications of AmmoniaDocumento5 pagineUses and Applications of AmmoniaSohail Asghar100% (2)
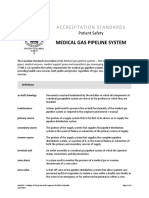
- NHMSFP As Medical Gas Pipeline SystemDocumento4 pagineNHMSFP As Medical Gas Pipeline SystemVijayakumar Madhaiyan0% (1)
- HeatingDocumento134 pagineHeatingraju1559405Nessuna valutazione finora
- Natural Gas TransportationDocumento13 pagineNatural Gas TransportationEsther ChungNessuna valutazione finora
- Medical GasDocumento67 pagineMedical Gassantosh100% (2)
- Robatherm Medical EngDocumento11 pagineRobatherm Medical EngSamiYousifNessuna valutazione finora
- Industrial Boiler Engineering ManualDocumento26 pagineIndustrial Boiler Engineering ManualnoxleekNessuna valutazione finora
- 147 20 Safe Practices Guide For Cryogenic Air Separation PlantsDocumento86 pagine147 20 Safe Practices Guide For Cryogenic Air Separation PlantsJose ChiriNessuna valutazione finora
- Chemistry e Brochure17 6956Documento16 pagineChemistry e Brochure17 6956Trebor ZurcNessuna valutazione finora
- 5 BS 5345 P3 Elect - Apparatus.explosive PDFDocumento16 pagine5 BS 5345 P3 Elect - Apparatus.explosive PDFSathishkumar PragasamNessuna valutazione finora
- Gases and Gases Blends PraxairDocumento18 pagineGases and Gases Blends PraxairAllen RosonNessuna valutazione finora
- Medical Gas System - Installer Orientation NotesDocumento8 pagineMedical Gas System - Installer Orientation NoteszampacaanasNessuna valutazione finora
- Presentation ATEX 114 at Opening KiwaExVisonDocumento18 paginePresentation ATEX 114 at Opening KiwaExVisonÖzlem ÖzkiliçNessuna valutazione finora
- Specialty Gas Catalog PDFDocumento204 pagineSpecialty Gas Catalog PDFsan.lorenzNessuna valutazione finora
- EIGA StandardsDocumento4 pagineEIGA StandardsGnaniar IlangoNessuna valutazione finora
- Foaming Tendencies of Oil TestsDocumento8 pagineFoaming Tendencies of Oil TestsJustin EvansNessuna valutazione finora
- Thesis On Energy Conservation On Plant UtilitesDocumento98 pagineThesis On Energy Conservation On Plant UtilitesAvinash Rai100% (1)
- Smoke Extraction Fans - 20100830174123Documento10 pagineSmoke Extraction Fans - 20100830174123Kristaps PuļķisNessuna valutazione finora
- Oxygen Plant Specification (50Nm3)Documento6 pagineOxygen Plant Specification (50Nm3)Win MinNessuna valutazione finora
- 28 08 2015lasanod Hospital Water Supply Design ReportDocumento5 pagine28 08 2015lasanod Hospital Water Supply Design ReportsubxaanalahNessuna valutazione finora
- Design and Application of Ammonia Heat PumpDocumento8 pagineDesign and Application of Ammonia Heat PumptasysatNessuna valutazione finora
- Catalogo Trox PDFDocumento500 pagineCatalogo Trox PDFBenjamín AlainNessuna valutazione finora
- SFPE 04-19-17 Fire Suppression Systems For DoD HangarsDocumento44 pagineSFPE 04-19-17 Fire Suppression Systems For DoD HangarsBagus Prambudi100% (1)
- 08252016122551manual of Procedure PDFDocumento305 pagine08252016122551manual of Procedure PDFSuyog patilNessuna valutazione finora
- DENAIR Oxygen Generator and Nitrogen Generator CatalogueDocumento8 pagineDENAIR Oxygen Generator and Nitrogen Generator CatalogueIngeniería AplicacionesNessuna valutazione finora
- Avoiding Explosions by Means of Inerting SystemsDocumento14 pagineAvoiding Explosions by Means of Inerting SystemsRicky Menon100% (1)
- Understanding Ambient Air Vaporizer Made Easier Now - INOXCVADocumento11 pagineUnderstanding Ambient Air Vaporizer Made Easier Now - INOXCVAGilberto YoshidaNessuna valutazione finora
- Conditioning and Distribution of Compressed AirDocumento19 pagineConditioning and Distribution of Compressed AirKCNessuna valutazione finora
- Prince Rupert Natural Gas Transmission Compressor Station Basics Factsheet TranscanadaDocumento2 paginePrince Rupert Natural Gas Transmission Compressor Station Basics Factsheet TranscanadaShaho Abdulqader MohamedaliNessuna valutazione finora
- EIGA 151 Prevention of Excessive Pressure During Filling of Cryogenic VesselsDocumento14 pagineEIGA 151 Prevention of Excessive Pressure During Filling of Cryogenic VesselsFilipNessuna valutazione finora
- Microplasma OzonatorDocumento16 pagineMicroplasma Ozonatoranurag jhaNessuna valutazione finora
- CFPA E Guideline No 26 2010 FDocumento30 pagineCFPA E Guideline No 26 2010 Fdvs99Nessuna valutazione finora
- Oil Refinery - Energy EducationDocumento3 pagineOil Refinery - Energy Educationmbw000012378Nessuna valutazione finora
- ATEXDocumento42 pagineATEXBledarNessuna valutazione finora
- Honeywell CS10XE Evaporative Air Cooler English - Instructions - ManualDocumento21 pagineHoneywell CS10XE Evaporative Air Cooler English - Instructions - Manualaljh71100% (2)
- MVS Hydrogen Generator Product CatalogueDocumento4 pagineMVS Hydrogen Generator Product CatalogueRachit VemulaNessuna valutazione finora
- PGS8 ORGANIC PEROXIDES: STORAGE English June 2012Documento115 paginePGS8 ORGANIC PEROXIDES: STORAGE English June 2012Максим Хило100% (1)
- OSHA Requirements ChlorineDocumento5 pagineOSHA Requirements Chlorineedsanchez021452Nessuna valutazione finora
- Industry AbbreviationsDocumento39 pagineIndustry Abbreviationsrafik1995Nessuna valutazione finora
- OSHA Accident InvestigationDocumento8 pagineOSHA Accident InvestigationNeel VaderaNessuna valutazione finora
- Facilities Management Strategic PlanDocumento13 pagineFacilities Management Strategic PlanRahman OlaitanNessuna valutazione finora
- 7 Video Lessons To Turn Geeks, Nerds, The Elderly, Obese and Mobility Disabled Into Bodybuilders - Finally PostedDocumento3 pagine7 Video Lessons To Turn Geeks, Nerds, The Elderly, Obese and Mobility Disabled Into Bodybuilders - Finally PostedPR.com 2Nessuna valutazione finora
- What Your Health and Safety Committee Will DoDocumento3 pagineWhat Your Health and Safety Committee Will DoRahman OlaitanNessuna valutazione finora
- All CumbriaDocumento67 pagineAll CumbriaRahman OlaitanNessuna valutazione finora
- HowToWriteObjectivesOutcomes PDFDocumento0 pagineHowToWriteObjectivesOutcomes PDFJay Sunga VillanNessuna valutazione finora
- How To Make Fitness A Reality, Not A Drama in The June Issue of Healthcare GlobalDocumento2 pagineHow To Make Fitness A Reality, Not A Drama in The June Issue of Healthcare GlobalPR.com 2Nessuna valutazione finora
- HardwareSheet On A+Documento4 pagineHardwareSheet On A+Rahman OlaitanNessuna valutazione finora
- Author: Dr. Krishna N. Sharma E-MailDocumento56 pagineAuthor: Dr. Krishna N. Sharma E-Mailmalmane91% (11)
- Author: Dr. Krishna N. Sharma E-MailDocumento56 pagineAuthor: Dr. Krishna N. Sharma E-Mailmalmane91% (11)
- VacancyDocumento11 pagineVacancyRahman OlaitanNessuna valutazione finora
- Useful Key Performance Indicators For Maintenance PDFDocumento8 pagineUseful Key Performance Indicators For Maintenance PDFfumerojr5164Nessuna valutazione finora
- Healthcare Bullnose Cylinder Instruction Guide Leaflet - 07409 - 85739Documento3 pagineHealthcare Bullnose Cylinder Instruction Guide Leaflet - 07409 - 85739Rahman OlaitanNessuna valutazione finora
- 640-822 ICND1 Exam TopicsDocumento4 pagine640-822 ICND1 Exam TopicsZoltan LedererNessuna valutazione finora
- Performance Indicators For MaintenanceDocumento5 paginePerformance Indicators For MaintenanceBNessuna valutazione finora
- Medical Gases WorkbookDocumento32 pagineMedical Gases WorkbookRahman OlaitanNessuna valutazione finora
- Performance Indicators For MaintenanceDocumento5 paginePerformance Indicators For MaintenanceBNessuna valutazione finora
- Medical Gases WorkbookDocumento32 pagineMedical Gases WorkbookRahman OlaitanNessuna valutazione finora