Potrebbero piacerti anche
- Low Back PainDocumento8 pagineLow Back PainLev KalikaNessuna valutazione finora
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentDa EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNessuna valutazione finora
- The Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyDocumento5 pagineThe Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyJORGE MANÇONessuna valutazione finora
- IvdpDocumento89 pagineIvdpFelix SabuNessuna valutazione finora
- Upper Limb OrthosisDocumento83 pagineUpper Limb OrthosisAwaisNessuna valutazione finora
- Wrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Documento63 pagineWrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Mnn SaabNessuna valutazione finora
- Rehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryDocumento11 pagineRehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryTech How AssamNessuna valutazione finora
- Cauda Equina and Conus Medullaris Syndromes Clinical PresentationDocumento9 pagineCauda Equina and Conus Medullaris Syndromes Clinical PresentationhoneyworksNessuna valutazione finora
- Kamars RadiologyDocumento135 pagineKamars RadiologyNayantara Nair100% (1)
- Cinahl Rotator Cuff InjuriesDocumento11 pagineCinahl Rotator Cuff InjurieslizardbeeNessuna valutazione finora
- Cervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension HeadachesDocumento10 pagineCervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension Headachespuchio100% (1)
- Neck PainDocumento1 paginaNeck PainHasan RahmanNessuna valutazione finora
- Total Hip Arthroplasty PDFDocumento10 pagineTotal Hip Arthroplasty PDFWindy ZeniccNessuna valutazione finora
- Brachial Plexus Injury GuideDocumento19 pagineBrachial Plexus Injury GuideAisyah AzaniNessuna valutazione finora
- SpondylodistitisDocumento32 pagineSpondylodistitisNurul Sakinah RosliNessuna valutazione finora
- Low BackDocumento7 pagineLow BackMuhammad FahmyNessuna valutazione finora
- Radial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHDocumento31 pagineRadial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHrajaeasNessuna valutazione finora
- Assessment of Back Pain-BMJDocumento30 pagineAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNessuna valutazione finora
- Orthosisofhandppt 181202162551Documento65 pagineOrthosisofhandppt 181202162551Khageswar SamalNessuna valutazione finora
- Frozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSDocumento6 pagineFrozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSpempekplgNessuna valutazione finora
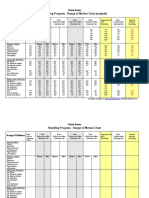
- Standing Program - Range of Motion Chart (Sample) : Client NameDocumento2 pagineStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNessuna valutazione finora
- Spondylolisthesis PDFDocumento121 pagineSpondylolisthesis PDFishak_alsophNessuna valutazione finora
- Low Back Pain: Rezki Amalia NurshalDocumento74 pagineLow Back Pain: Rezki Amalia NurshalRezki Amalia NurshalNessuna valutazione finora
- MSK Us ProtocolsDocumento40 pagineMSK Us Protocolsjamir59Nessuna valutazione finora
- MusculoskeletalDocumento119 pagineMusculoskeletalEdissa PangilinanNessuna valutazione finora
- Scoliosis: Degenerative & IdiopathicDocumento34 pagineScoliosis: Degenerative & IdiopathicClaudia MariscaNessuna valutazione finora
- A Patient's Guide To Radial Tunnel SyndromeDocumento4 pagineA Patient's Guide To Radial Tunnel SyndromeKarunya Vk100% (1)
- Fracture Colles Rehabilitation Advice Following WristDocumento4 pagineFracture Colles Rehabilitation Advice Following WristfaprilisaNessuna valutazione finora
- Clinical Signs - NamedDocumento9 pagineClinical Signs - NamedsprapurNessuna valutazione finora
- Scoliosis (Curved Spine)Documento7 pagineScoliosis (Curved Spine)Chow Mun FaiNessuna valutazione finora
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocumento59 pagineWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNessuna valutazione finora
- Lumbar Radiculopathy Medback Castillo Mendez EDITEDDocumento12 pagineLumbar Radiculopathy Medback Castillo Mendez EDITEDSteve ColbertNessuna valutazione finora
- Genu Recurvatum SyndromDocumento7 pagineGenu Recurvatum SyndromRoxana RascaNessuna valutazione finora
- Lumbar Spine AssesmentDocumento8 pagineLumbar Spine AssesmentPavithra SivanathanNessuna valutazione finora
- Ankle Examination Orthopaedics McraeDocumento6 pagineAnkle Examination Orthopaedics McraeHafizah HoshniNessuna valutazione finora
- Musculoskeletal TraumaDocumento103 pagineMusculoskeletal TraumaJona Kristin EnclunaNessuna valutazione finora
- Peripheral Nerve Blocks Lower ExtremityDocumento53 paginePeripheral Nerve Blocks Lower ExtremityArief Hariyadi SantosoNessuna valutazione finora
- Hand PDFDocumento179 pagineHand PDFRadenSiwi Bagus HadhiningratNessuna valutazione finora
- Principles of Tendon Transfer in The Hand and ForearmDocumento9 paginePrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiNessuna valutazione finora
- Cervical DisordersDocumento89 pagineCervical DisordersAbdallah Samir Mostafa٢٠١٩٠٢١٥٩Nessuna valutazione finora
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Assessment of Posture: Prepared By: Floriza P. de Leon, PTRPDocumento17 pagineAssessment of Posture: Prepared By: Floriza P. de Leon, PTRPFloriza de Leon100% (1)
- Management L Low Back PainDocumento7 pagineManagement L Low Back PainelsyamelindaNessuna valutazione finora
- Lumbar Spine AssessmentDocumento26 pagineLumbar Spine Assessmentyoyo_pt2007100% (1)
- Fractures of Spine and Pelvis2007Documento70 pagineFractures of Spine and Pelvis2007api-19916399Nessuna valutazione finora
- Juvenile Idiopathic ArthritisDocumento14 pagineJuvenile Idiopathic ArthritisClaudiaCazacuNessuna valutazione finora
- Carpal Tunnel Syndrome JAAOS 2007 PDFDocumento12 pagineCarpal Tunnel Syndrome JAAOS 2007 PDFStefano Pareschi PasténNessuna valutazione finora
- Tendon TransferDocumento1 paginaTendon TransferPandi Smart VjNessuna valutazione finora
- Cervical Spine EvaluationDocumento9 pagineCervical Spine EvaluationS.Muhaymen HussainNessuna valutazione finora
- B 756 Vertebris GB III10Documento44 pagineB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- 87 Slides Fundamentals in Orthopedic Surgery 2019Documento88 pagine87 Slides Fundamentals in Orthopedic Surgery 2019Mark Samuel Tanchoco100% (1)
- The Wrist Common Injuries and ManagementDocumento36 pagineThe Wrist Common Injuries and ManagementDan RollorataNessuna valutazione finora
- Spine Fractures and Spinal Cord InjuryDocumento54 pagineSpine Fractures and Spinal Cord InjuryAloy PudeNessuna valutazione finora
- Beighton Hypermobility ScoreDocumento2 pagineBeighton Hypermobility ScoreVishal RautNessuna valutazione finora
- Spondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisDocumento36 pagineSpondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisneareastspineNessuna valutazione finora
- Ultrasound Guided Lower Limb Blocks Tony AllenDocumento39 pagineUltrasound Guided Lower Limb Blocks Tony Allenrepre64Nessuna valutazione finora
- Week 1 and 2 PCP Workbook QuestionsDocumento4 pagineWeek 1 and 2 PCP Workbook Questionsapi-479717740100% (1)
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsValutazione: 4 su 5 stelle4/5 (2)
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementDa EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementNessuna valutazione finora
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Leprosy PDFDocumento19 pagineLeprosy PDFsteffiecruz06Nessuna valutazione finora
- Coronary Artery DiseaseDocumento5 pagineCoronary Artery Diseasesteffiecruz06Nessuna valutazione finora
- Cardiac RehabDocumento37 pagineCardiac Rehabsteffiecruz06Nessuna valutazione finora
- Overuse SyndromeDocumento20 pagineOveruse Syndromesteffiecruz06Nessuna valutazione finora
- Delayed Onset Muscle Soreness (Doms)Documento2 pagineDelayed Onset Muscle Soreness (Doms)steffiecruz06Nessuna valutazione finora
- Chronic Fatigue Syndrome PDFDocumento22 pagineChronic Fatigue Syndrome PDFsteffiecruz06Nessuna valutazione finora
- FibromyalgiaDocumento20 pagineFibromyalgiasteffiecruz06Nessuna valutazione finora
- Chronic PainDocumento38 pagineChronic Painsteffiecruz06Nessuna valutazione finora
- XL MulticalDocumento2 pagineXL MulticalĐào Huy VănNessuna valutazione finora
- Icmr-National Institute For Research in Tuberculosis-ChennaiDocumento27 pagineIcmr-National Institute For Research in Tuberculosis-Chennaidhanya sriNessuna valutazione finora
- Retinal Diseases - 5Documento2 pagineRetinal Diseases - 5AkicaNessuna valutazione finora
- Lyme, CF ProtocolDocumento36 pagineLyme, CF ProtocolTheresa Dale100% (1)
- Dengue Case SolutionDocumento9 pagineDengue Case SolutionPRASHANT GUPTA0% (1)
- Serological Diagnosis of Infectious DiseasesDocumento38 pagineSerological Diagnosis of Infectious DiseasesPurple basketNessuna valutazione finora
- KIT Volume XXI No 1 April 2009 PropDocumento16 pagineKIT Volume XXI No 1 April 2009 PropKITexBruderhofCCINessuna valutazione finora
- CA MammaeDocumento30 pagineCA MammaeAlfiany SahrNessuna valutazione finora
- 2005 Coxe Cooper Avian FluDocumento37 pagine2005 Coxe Cooper Avian Flupep59Nessuna valutazione finora
- Endodontic MicrobiologyDocumento9 pagineEndodontic MicrobiologySarah KahilNessuna valutazione finora
- RBI Sees 9.5 PC GDP Contraction in FY21: India S Active Covid-19 Cases Fall Below 9 LakhDocumento12 pagineRBI Sees 9.5 PC GDP Contraction in FY21: India S Active Covid-19 Cases Fall Below 9 LakhGauravNessuna valutazione finora
- Handbook of African Swine Fever in Wild BoarDocumento111 pagineHandbook of African Swine Fever in Wild BoarMayeth MacedaNessuna valutazione finora
- Zygomatic Implants PDFDocumento18 pagineZygomatic Implants PDFgirl33Nessuna valutazione finora
- Ajit Kulkarni - LachesisDocumento8 pagineAjit Kulkarni - LachesisAntonio Andres BergesNessuna valutazione finora
- Flesh-Eating BacteriaDocumento3 pagineFlesh-Eating BacteriaEdward McSweegan, PhD100% (2)
- Fastest way to travel from Misamis Occidental to Camiguin islandDocumento3 pagineFastest way to travel from Misamis Occidental to Camiguin islandNina Romina NavaltaNessuna valutazione finora
- General Veterinary Parasitology and Helminthology PDFDocumento253 pagineGeneral Veterinary Parasitology and Helminthology PDFLakshmi75% (4)
- Micro-Blading PPT GBDocumento55 pagineMicro-Blading PPT GBMarina Koza100% (4)
- STIs Part ADocumento3 pagineSTIs Part AMihaela EneNessuna valutazione finora
- Executive Summary Per Barangay in A Semester For CHN For FacultyDocumento5 pagineExecutive Summary Per Barangay in A Semester For CHN For FacultyAmira Fatmah QuilapioNessuna valutazione finora
- 15 Leave PDFDocumento12 pagine15 Leave PDFKarthiga SelviNessuna valutazione finora
- Integrated Helminth Control Program (IHCP) : Date VenueDocumento31 pagineIntegrated Helminth Control Program (IHCP) : Date VenueAnonymous100% (2)
- Daftar Pustaka: Dermatology, 2Documento3 pagineDaftar Pustaka: Dermatology, 2Kusmantoro HidayatNessuna valutazione finora
- Kisi Soal BHS Inggris KLS Xii Pas GanjilDocumento4 pagineKisi Soal BHS Inggris KLS Xii Pas Ganjilirawan dwi putraNessuna valutazione finora
- Contact Lens Complications and ManagementDocumento10 pagineContact Lens Complications and Managementstrawberry8832850% (2)
- Participatory LectureDocumento5 pagineParticipatory LectureThandiMtungwaNessuna valutazione finora
- Word Formation 2417Documento8 pagineWord Formation 2417Adam BrzostekNessuna valutazione finora
- Cystic Fibrosis Signs and Symptoms ExplainedDocumento3 pagineCystic Fibrosis Signs and Symptoms ExplainedsakthiprimeNessuna valutazione finora
- Cardiovascular Health DrillsDocumento10 pagineCardiovascular Health DrillsnotadagNessuna valutazione finora
- Making System Dynamics Cool II: New Hot Teaching and Testing Cases of Increasing ComplexityDocumento29 pagineMaking System Dynamics Cool II: New Hot Teaching and Testing Cases of Increasing ComplexityAdrian HNessuna valutazione finora