Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Terapi Dengue Dengan SteroidDocumento10 pagineTerapi Dengue Dengan Steroiddr.cintaNessuna valutazione finora
- Medical Student at Islamic University of Indonesia 2. Medical Student at Islamic University of IndonesiaDocumento1 paginaMedical Student at Islamic University of Indonesia 2. Medical Student at Islamic University of Indonesiadr.cintaNessuna valutazione finora
- Lipofilm Microemulsion Effectiveness in Dry EyeDocumento5 pagineLipofilm Microemulsion Effectiveness in Dry Eyedr.cintaNessuna valutazione finora
- Sign and Symptoms of Coronary-SyndromeDocumento11 pagineSign and Symptoms of Coronary-SyndromeRatna Pusvita Effendy'sNessuna valutazione finora
- CA Worksheet 3Documento2 pagineCA Worksheet 3dr.cintaNessuna valutazione finora
- 5 19 WHO ReferenceDocumento2 pagine5 19 WHO ReferenceSidney Pereira CostaNessuna valutazione finora
- Gambaran Tingkat Depresi Pada Pasien Gagal Ginjal KronikDocumento19 pagineGambaran Tingkat Depresi Pada Pasien Gagal Ginjal KronikGupiesNessuna valutazione finora
- xT1 - 462007059 - Daftar PustakaDocumento0 paginexT1 - 462007059 - Daftar Pustakadr.cintaNessuna valutazione finora
- Samsung SCDocumento3 pagineSamsung SCdr.cintaNessuna valutazione finora
- Cover CDDocumento1 paginaCover CDdr.cintaNessuna valutazione finora
- 5801 PeritonitisDocumento19 pagine5801 Peritonitisdr.cintaNessuna valutazione finora
- Is Schizoaffective Disorder A Distinct Categorical Diagnosis? A Critical Review of The LiteratureDocumento22 pagineIs Schizoaffective Disorder A Distinct Categorical Diagnosis? A Critical Review of The Literaturedr.cintaNessuna valutazione finora
- Gambaran Tingkat Depresi Pada Pasien Gagal Ginjal KronikDocumento19 pagineGambaran Tingkat Depresi Pada Pasien Gagal Ginjal KronikGupiesNessuna valutazione finora
- Peran Pemimpin Sebagai Pemberdaya Dan Motivator Anggota Di Direktorat Reserse Narkoba Polda Jawa TengahDocumento8 paginePeran Pemimpin Sebagai Pemberdaya Dan Motivator Anggota Di Direktorat Reserse Narkoba Polda Jawa Tengahdr.cintaNessuna valutazione finora
- Nausea y Vomito Inducidos Por Opioides Que HacerDocumento10 pagineNausea y Vomito Inducidos Por Opioides Que HacersukmaadityaputraNessuna valutazione finora
- Mallampati Airway ClassificationDocumento6 pagineMallampati Airway ClassificationAnthony Osemudiamen OseghaleNessuna valutazione finora
- Remission in Schizophrenia: One-Year Italian Prospective Study of Risperidone Long-Acting Injectable (RLAI) in Patients With Schizophrenia or Schizoaffective DisorderDocumento11 pagineRemission in Schizophrenia: One-Year Italian Prospective Study of Risperidone Long-Acting Injectable (RLAI) in Patients With Schizophrenia or Schizoaffective Disorderdr.cintaNessuna valutazione finora
- Relationship Between Intraoperative Mean Arterial.10Documento9 pagineRelationship Between Intraoperative Mean Arterial.10dr.cintaNessuna valutazione finora
- 5 19 WHO ReferenceDocumento2 pagine5 19 WHO ReferenceSidney Pereira CostaNessuna valutazione finora
- Fifteen-Year Follow-Up of ICD-10 Schizoaffective Disorders Compared With Schizophrenia and Affective DisordersDocumento9 pagineFifteen-Year Follow-Up of ICD-10 Schizoaffective Disorders Compared With Schizophrenia and Affective Disordersdr.cintaNessuna valutazione finora
- IPAQ English Self-Admin ShortDocumento3 pagineIPAQ English Self-Admin ShortDavid Curtis MintahNessuna valutazione finora
- BMI Chart for Boys Ages 5-19Documento1 paginaBMI Chart for Boys Ages 5-19Justitia LantuNessuna valutazione finora
- Research: Cite This Article As: BMJ, Doi:10.1136/bmj.38881.382755.2f (Published 6 July 2006)Documento6 pagineResearch: Cite This Article As: BMJ, Doi:10.1136/bmj.38881.382755.2f (Published 6 July 2006)dr.cintaNessuna valutazione finora
- RIKSA ADITYA PRAMUDITA. Risk Factor of Obesity at Elementary SchoolDocumento1 paginaRIKSA ADITYA PRAMUDITA. Risk Factor of Obesity at Elementary Schooldr.cintaNessuna valutazione finora
- Abstract TV PrestasiDocumento2 pagineAbstract TV Prestasidr.cintaNessuna valutazione finora
- Pediatrics 2006 2563 9Documento12 paginePediatrics 2006 2563 9dr.cintaNessuna valutazione finora
- Pediatrics 2001 423 6Documento6 paginePediatrics 2001 423 6dr.cintaNessuna valutazione finora
- Kritis YuniDocumento10 pagineKritis YuniDhede MahmudahNessuna valutazione finora
- Validation of A Risk Stratification Index and Risk.12Documento16 pagineValidation of A Risk Stratification Index and Risk.12dr.cintaNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- PF AssignmentDocumento5 paginePF AssignmentRushikesh MahajanNessuna valutazione finora
- A Study of Nutritional Assessment of Newly Diagnos PDFDocumento7 pagineA Study of Nutritional Assessment of Newly Diagnos PDFKaushik SahaNessuna valutazione finora
- 259233085-Reader-s-Digest-International-February-2015 (Subrayado) PDFDocumento130 pagine259233085-Reader-s-Digest-International-February-2015 (Subrayado) PDFClaudia Mela OrtizNessuna valutazione finora
- DevelopmentDocumento22 pagineDevelopmentTapas BanerjeeNessuna valutazione finora
- Cardiovascular Disease BrochureDocumento2 pagineCardiovascular Disease BrochureKawooya Ismael100% (1)
- PracticalsDocumento29 paginePracticalsRitik PatelNessuna valutazione finora
- Introduction To Physical Education and Physical FitnessDocumento6 pagineIntroduction To Physical Education and Physical Fitnessjansel pallasigueNessuna valutazione finora
- ESPEN Guideline Clinical Nutrition in SurgeryDocumento28 pagineESPEN Guideline Clinical Nutrition in SurgeryekalospratamaNessuna valutazione finora
- Mna Mini English PDFDocumento1 paginaMna Mini English PDFNadi SyahNessuna valutazione finora
- Fitness AssessmentDocumento29 pagineFitness AssessmentSanjanaa ZadNessuna valutazione finora
- The Amen Solution by Daniel G. Amen MD - ExcerptDocumento40 pagineThe Amen Solution by Daniel G. Amen MD - ExcerptCrown Publishing Group75% (12)
- Physical Education 1 Lecture Notes – Week 5Documento11 paginePhysical Education 1 Lecture Notes – Week 5Lucky GeminaNessuna valutazione finora
- Wellness Final PaperDocumento5 pagineWellness Final Paperapi-482557062Nessuna valutazione finora
- Trese Family A Family Case AnalysisDocumento33 pagineTrese Family A Family Case AnalysisCatherine AquinoNessuna valutazione finora
- Introduction To Yoga and Yogic Practices IgnouDocumento17 pagineIntroduction To Yoga and Yogic Practices IgnouDarshan GowdilluNessuna valutazione finora
- Waist Height Ratio - The Bulk-or-Cut Cheat-Sheet (Public)Documento8 pagineWaist Height Ratio - The Bulk-or-Cut Cheat-Sheet (Public)Shashvat ChitranshNessuna valutazione finora
- Cardio GuideDocumento121 pagineCardio GuideBaciu DianaNessuna valutazione finora
- Managing CholesterolDocumento16 pagineManaging CholesterolGiannis Karp100% (2)
- AlimiDocumento10 pagineAlimiAhmad FarisNessuna valutazione finora
- Importance of Nutrition in Nursing EducationDocumento247 pagineImportance of Nutrition in Nursing EducationShikinah LaroyaNessuna valutazione finora
- F4 SC Nota Bab 3 Techniques of Measuring The Parameters of Body HealthDocumento13 pagineF4 SC Nota Bab 3 Techniques of Measuring The Parameters of Body HealthJIanyun ChanNessuna valutazione finora
- NIH Public Access: Prolapse Symptoms in Overweight and Obese Women Before and After Weight LossDocumento12 pagineNIH Public Access: Prolapse Symptoms in Overweight and Obese Women Before and After Weight LossArdin TodingNessuna valutazione finora
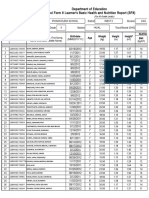
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Documento4 pagineDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Roxan DosdosNessuna valutazione finora
- Physical Fitness Test Score CardDocumento2 paginePhysical Fitness Test Score CardDafchen Nio MahasolNessuna valutazione finora
- PHYSICAL EDUCAT-WPS OfficeDocumento9 paginePHYSICAL EDUCAT-WPS OfficeMark Joel FortunatoNessuna valutazione finora
- Understanding Development GoalsDocumento15 pagineUnderstanding Development GoalsHimangshu KarNessuna valutazione finora
- PFT Score CardDocumento1 paginaPFT Score CardManilyn SuarezNessuna valutazione finora
- HTH668 Chp.6 - Hospitality Strategic ManagementDocumento5 pagineHTH668 Chp.6 - Hospitality Strategic ManagementDanial D'Haqim M.NNessuna valutazione finora
- Cerebral Palsy Presentation 2Documento13 pagineCerebral Palsy Presentation 2api-664219351Nessuna valutazione finora