Potrebbero piacerti anche
- Kardiogenik SyokDocumento43 pagineKardiogenik SyokGalih Arief Harimurti WawolumajaNessuna valutazione finora
- Patofisiologi Shock CardiogenicDocumento44 paginePatofisiologi Shock CardiogenicGalih Arief Harimurti Wawolumaja100% (1)
- Cardiogenic ShockDocumento49 pagineCardiogenic Shockmaibejose0% (1)
- ShockDocumento64 pagineShockAnusha VergheseNessuna valutazione finora
- Pharmacotherapy - Heart Failure - Dr. Mohammed KamalDocumento62 paginePharmacotherapy - Heart Failure - Dr. Mohammed KamalMohammed KamalNessuna valutazione finora
- Shock Tugas Anestesi ViliaDocumento81 pagineShock Tugas Anestesi ViliaviliaNessuna valutazione finora
- Taufan Arif, S.Kep., NS., M.KepDocumento85 pagineTaufan Arif, S.Kep., NS., M.KepputriNessuna valutazione finora
- ShockDocumento36 pagineShockJohnryan NdiranguNessuna valutazione finora
- Mi CaseDocumento5 pagineMi CaseffaaNessuna valutazione finora
- Atrial Fibrilation GauDocumento39 pagineAtrial Fibrilation GauRANA MOHAMMED HAMOOD AL-HADEQNessuna valutazione finora
- Lecture 8Documento7 pagineLecture 8Grafu Andreea AlexandraNessuna valutazione finora
- 3 ShockDocumento12 pagine3 ShockAiden JosephatNessuna valutazione finora
- Ischemic Heart DiseaseDocumento67 pagineIschemic Heart Diseasealfaz lakhani80% (5)
- Although Shock Has Been Recognised For Over 100 YearsDocumento4 pagineAlthough Shock Has Been Recognised For Over 100 YearsRusty HoganNessuna valutazione finora
- Heart FailureDocumento77 pagineHeart FailureJudy Anne PatricioNessuna valutazione finora
- ShockDocumento22 pagineShockAbdul MajidNessuna valutazione finora
- BAU PTR-Neurology-Lecture 11-StrokeDocumento133 pagineBAU PTR-Neurology-Lecture 11-Strokeerfan mohammadiNessuna valutazione finora
- ShockDocumento9 pagineShockapocruNessuna valutazione finora
- Ntroduction To The Physical ExaminationDocumento4 pagineNtroduction To The Physical ExaminationAngelica NenitaNessuna valutazione finora
- Lec 3Documento17 pagineLec 3Yousef El3alamey0% (1)
- Shock 20231122 213304 0000Documento32 pagineShock 20231122 213304 0000Mikella E. PAGNAMITANNessuna valutazione finora
- Acquired Central Nervous System Vascular Disorders-1Documento39 pagineAcquired Central Nervous System Vascular Disorders-1Jake MillerNessuna valutazione finora
- Athero 2 Dr. Raquid 2021Documento93 pagineAthero 2 Dr. Raquid 2021oreaNessuna valutazione finora
- The Next Sequel: Scarring My HeartDocumento56 pagineThe Next Sequel: Scarring My Heartshmily_0810Nessuna valutazione finora
- PPP v3Documento771 paginePPP v3Steven Lam100% (1)
- Cardiology-6 CADDocumento20 pagineCardiology-6 CADMahmoud RamadanNessuna valutazione finora
- Cardiovascular DisordersDocumento20 pagineCardiovascular DisordersHampson MalekanoNessuna valutazione finora
- Curs 9 Myocarditis CardiomyopathyDocumento41 pagineCurs 9 Myocarditis CardiomyopathyIliescu DenisaNessuna valutazione finora
- 6.0 IDS ShockDocumento4 pagine6.0 IDS ShockEdalyn CapiliNessuna valutazione finora
- Clinical Neurology Answers OnlyDocumento68 pagineClinical Neurology Answers Onlyanas kNessuna valutazione finora
- ShockDocumento18 pagineShocksantokh108Nessuna valutazione finora
- ShockDocumento63 pagineShockAhmedNessuna valutazione finora
- HTN and CHFDocumento29 pagineHTN and CHFkiflomNessuna valutazione finora
- Heart Failure and Pulmonary EdemaDocumento60 pagineHeart Failure and Pulmonary EdemaYosra —Nessuna valutazione finora
- Stroke: Clinical Presentation and Anatomical LocalizationDocumento36 pagineStroke: Clinical Presentation and Anatomical LocalizationYusuf JoganNessuna valutazione finora
- Examination and Investigation of The Cardiovascular System (CVS)Documento27 pagineExamination and Investigation of The Cardiovascular System (CVS)Jake MillerNessuna valutazione finora
- Alteration in Perfusion 2Documento28 pagineAlteration in Perfusion 2Atteya Mogote AbdullahNessuna valutazione finora
- Topic:: Unstable AnginaDocumento44 pagineTopic:: Unstable AnginaApurba100% (1)
- IschemicHeartDisease LectureDocumento64 pagineIschemicHeartDisease LectureFerdinand RobertNessuna valutazione finora
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocumento31 pagineHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNessuna valutazione finora
- Stroke: DR Abdirahman AbibDocumento40 pagineStroke: DR Abdirahman AbibMahad IbrahemNessuna valutazione finora
- 115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p53Documento1 pagina115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p53MuhNatsirNessuna valutazione finora
- Trauma and Its ComplicationsDocumento80 pagineTrauma and Its Complicationsjoe BouGhazaliNessuna valutazione finora
- ShockDocumento53 pagineShockHassan Ahmed100% (3)
- Copstead-Kirkhorn: Pathophysiology, 4 Edition: Disease Profiles Cardiogenic ShockDocumento2 pagineCopstead-Kirkhorn: Pathophysiology, 4 Edition: Disease Profiles Cardiogenic ShockadadanNessuna valutazione finora
- Pathophysiology of Pericardial DiseaseDocumento36 paginePathophysiology of Pericardial DiseaseivaniNessuna valutazione finora
- ShockDocumento2 pagineShockYousef El3alameyNessuna valutazione finora
- Electrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosisDocumento38 pagineElectrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosislorhenzsoNessuna valutazione finora
- Pemicu 6 Eko Blok KGDDocumento128 paginePemicu 6 Eko Blok KGDEko SiswantoNessuna valutazione finora
- Cardiac TemponadeDocumento18 pagineCardiac TemponadeDIVYA GANGWAR100% (1)
- Prof Univ DR Ion C.Tintoiu FESC Centrul de Cardiologie Al Armatei Universitatea Titu MaiorescuDocumento719 pagineProf Univ DR Ion C.Tintoiu FESC Centrul de Cardiologie Al Armatei Universitatea Titu MaiorescuVioleta Malina Bîrsan HodivoianuNessuna valutazione finora
- Stroke UgDocumento76 pagineStroke Ug74. Shravani VNessuna valutazione finora
- Shock and Circulatory FailureDocumento8 pagineShock and Circulatory FailureOktaviana Sari DewiNessuna valutazione finora
- Syncope: Global Cerebral Blood FlowDocumento7 pagineSyncope: Global Cerebral Blood FlowChananNessuna valutazione finora
- Neurosurgery: UnprotectedDocumento39 pagineNeurosurgery: UnprotectedMaulana Taufik100% (2)
- Stroke CMEDocumento34 pagineStroke CMEKeren Karunya SingamNessuna valutazione finora
- 8.syncope & PresyncopeDocumento11 pagine8.syncope & PresyncopeIbrahim RamizNessuna valutazione finora
- Cardiac Emergencies Cne DelhiDocumento109 pagineCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- Cardiology DR Osama MahmoudDocumento138 pagineCardiology DR Osama MahmoudIsmail Habib100% (4)
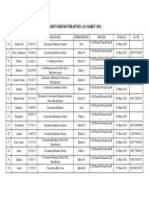
- Pasien Khemoterapi Bulan Maret 2012Documento1 paginaPasien Khemoterapi Bulan Maret 2012Putri Nurul HidayahNessuna valutazione finora
- Pasien Khemoterapi Bulan Maret 2012Documento1 paginaPasien Khemoterapi Bulan Maret 2012Putri Nurul HidayahNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaPutri Nurul HidayahNessuna valutazione finora
- Obst Sleep Apnea 060515Documento7 pagineObst Sleep Apnea 060515Putri Nurul HidayahNessuna valutazione finora
- Gagal Ginjal KronikDocumento20 pagineGagal Ginjal KronikFendy SuyantoNessuna valutazione finora
- A.R.I Well D-ONE® - InstructionsDocumento9 pagineA.R.I Well D-ONE® - InstructionsHari YantoNessuna valutazione finora
- Diagnosis of Paraprotein DiseasesDocumento29 pagineDiagnosis of Paraprotein DiseasesScarlettMLVNessuna valutazione finora
- Bloodborne Pathogens Program: Western Oklahoma State College Employee Training HandbookDocumento35 pagineBloodborne Pathogens Program: Western Oklahoma State College Employee Training HandbookKashaNessuna valutazione finora
- Hepato-Biliary System and Their DisordersDocumento131 pagineHepato-Biliary System and Their DisordersIton BumatayNessuna valutazione finora
- Chapter 1Documento38 pagineChapter 1synap5esNessuna valutazione finora
- Answer Sheet: Name: Test: 70minDocumento3 pagineAnswer Sheet: Name: Test: 70minThanh TâmNessuna valutazione finora
- F U R D C GDocumento33 pagineF U R D C GGiosué Reyes HernandezNessuna valutazione finora
- BMBL-5th EditionDocumento421 pagineBMBL-5th EditionBryan OngNessuna valutazione finora
- Nicky - Human Milk BankDocumento2 pagineNicky - Human Milk BankKaye Tubungbanua - MatunogNessuna valutazione finora
- Gale Mein Dard Khansi Kharash Aur Infection Ka Ilaj Ke UpayDocumento3 pagineGale Mein Dard Khansi Kharash Aur Infection Ka Ilaj Ke UpayGovindNessuna valutazione finora
- Ontimmunol09 01837Documento17 pagineOntimmunol09 01837akshayajainaNessuna valutazione finora
- Diagnostic Imaging ChestDocumento1.485 pagineDiagnostic Imaging ChestMạnh Đình Nguyễn100% (1)
- Date Report Date Name Age/Sex Lab No. Reg. No. Panel Name Slide No. Ref. Dr. Report StatusDocumento2 pagineDate Report Date Name Age/Sex Lab No. Reg. No. Panel Name Slide No. Ref. Dr. Report StatusSaurabh SinghNessuna valutazione finora
- Nano Today: Marcel Alexander Heinrich, Byron Martina, Jai PrakashDocumento21 pagineNano Today: Marcel Alexander Heinrich, Byron Martina, Jai Prakashvishal makadiaNessuna valutazione finora
- CDCDocumento116 pagineCDCRam BasanyNessuna valutazione finora
- Differences Between Staphylococcus and Streptococcus - Microbiology NotesDocumento3 pagineDifferences Between Staphylococcus and Streptococcus - Microbiology NotesSareeya ShreNessuna valutazione finora
- Common Tropical Disease in ThailandDocumento84 pagineCommon Tropical Disease in ThailandDr.Sathaporn KunnathumNessuna valutazione finora
- Parasites & People - Host Parasite Relationship - RumalaDocumento40 pagineParasites & People - Host Parasite Relationship - RumalamicroperadeniyaNessuna valutazione finora
- Biodfence Product InsertDocumento2 pagineBiodfence Product Insertapi-235072265Nessuna valutazione finora
- The Selection and Use of Essential in Vitro Diagnostics: WHO Technical Report SeriesDocumento380 pagineThe Selection and Use of Essential in Vitro Diagnostics: WHO Technical Report SeriesJOSHITHANessuna valutazione finora
- 13.approach To Upper Respiratory Tract InfectionsDocumento3 pagine13.approach To Upper Respiratory Tract InfectionsRed DevilNessuna valutazione finora
- DengvaxiaDocumento1 paginaDengvaxiaAce Bryan Niño LlesolNessuna valutazione finora
- Premarital SexDocumento6 paginePremarital SexArcon AlvarNessuna valutazione finora
- Jurnal SleDocumento2 pagineJurnal SlePratidina Dwinda HENessuna valutazione finora
- Path GitDocumento18 paginePath Gitvnair112Nessuna valutazione finora
- Lecture6 Intro, Classification of ParasitesDocumento38 pagineLecture6 Intro, Classification of ParasitesJumar Villegas100% (1)
- Chapter 3 Infection Control: Phlebotomy, 5e (Booth)Documento13 pagineChapter 3 Infection Control: Phlebotomy, 5e (Booth)Carol Reed100% (1)
- Sapphire Insect Transfection KitDocumento1 paginaSapphire Insect Transfection KitAlleleBiotechNessuna valutazione finora
- Hand Foot Mouth Disease (HFMD) For TeachersDocumento2 pagineHand Foot Mouth Disease (HFMD) For Teachersalbeny j.pNessuna valutazione finora