Potrebbero piacerti anche
- Arch Width Changes From 6 Weeks To 45 Years of AgeDocumento9 pagineArch Width Changes From 6 Weeks To 45 Years of AgeMafe SalazarNessuna valutazione finora
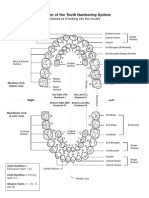
- Diagram of The Tooth Numbering SystemDocumento1 paginaDiagram of The Tooth Numbering Systemsaleh900Nessuna valutazione finora
- Long-Term Spontaneous Changes Following Removal of All First Premolars in Class I Cases With CrowdingDocumento12 pagineLong-Term Spontaneous Changes Following Removal of All First Premolars in Class I Cases With CrowdingElizabeth MesaNessuna valutazione finora
- The Displaced Lower Third Molar: A Literature Review and Suggestions For ManagementDocumento5 pagineThe Displaced Lower Third Molar: A Literature Review and Suggestions For ManagementRajat GuptaNessuna valutazione finora
- Orthodontic treatment's greater impact on adolescents' gingivitisDocumento8 pagineOrthodontic treatment's greater impact on adolescents' gingivitisMárcio LMSNessuna valutazione finora
- Living and radiological anatomy of the head and neck for dental studentsDa EverandLiving and radiological anatomy of the head and neck for dental studentsValutazione: 4 su 5 stelle4/5 (1)
- Brown 1993 Prevalence and Epidemiology PerioDocumento15 pagineBrown 1993 Prevalence and Epidemiology PeriojeremyvoNessuna valutazione finora
- Comparison of Peri-Implant and Periodontal Marginal Soft Tissues in Health and Diseas Perio 2000 Vol 76 PDFDocumento15 pagineComparison of Peri-Implant and Periodontal Marginal Soft Tissues in Health and Diseas Perio 2000 Vol 76 PDFchandana100% (2)
- Glenoid Fossa RemodellingDocumento59 pagineGlenoid Fossa RemodellingArnabNessuna valutazione finora
- Fransson 1996Documento8 pagineFransson 1996Éverton Salgado MonteiroNessuna valutazione finora
- Changes in dentition from finger-sucking therapyDocumento5 pagineChanges in dentition from finger-sucking therapyIsabel Escobar MinotasNessuna valutazione finora
- 2.importance of Pre-Operative HRCT Temporal Bone PDFDocumento5 pagine2.importance of Pre-Operative HRCT Temporal Bone PDFDR K C MALLIKNessuna valutazione finora
- Fundamental Considerations of The Design and Function of Intranasal AntrostomiesDocumento4 pagineFundamental Considerations of The Design and Function of Intranasal AntrostomiessevattapillaiNessuna valutazione finora
- 2018 Article 1362 PDFDocumento5 pagine2018 Article 1362 PDFAuliaMahdaniatiNessuna valutazione finora
- Bishara 1989Documento14 pagineBishara 1989habeebNessuna valutazione finora
- Palatal Expansion in Adults: The Nonsurgical Approach: Point/CounterpointDocumento4 paginePalatal Expansion in Adults: The Nonsurgical Approach: Point/CounterpointjoserodrrNessuna valutazione finora
- Submental Flap Reconstruction for Oral Cavity CancerDocumento3 pagineSubmental Flap Reconstruction for Oral Cavity CancerKaran HarshavardhanNessuna valutazione finora
- Ultrasonic Determination of Gingival Thickness 1996Documento8 pagineUltrasonic Determination of Gingival Thickness 1996João Carlos Bittencourt RibeiroNessuna valutazione finora
- The Mandibuiar Speech Envelope in Subjects With and Without Incisai Tooth WearDocumento6 pagineThe Mandibuiar Speech Envelope in Subjects With and Without Incisai Tooth Wearjinny1_0Nessuna valutazione finora
- Chin Cup Therapy For Mandibular PrognathismDocumento19 pagineChin Cup Therapy For Mandibular PrognathismSreenivasa Krishna ChaitanyaNessuna valutazione finora
- Abstract-The Adverse Effects of Periodontal Disease On Dental Pulp Have Been Debated For ManyDocumento11 pagineAbstract-The Adverse Effects of Periodontal Disease On Dental Pulp Have Been Debated For ManySri RahmawatiNessuna valutazione finora
- Artikel OccipitomentaDocumento12 pagineArtikel OccipitomentaSharon NathaniaNessuna valutazione finora
- Dentoalveolar Effects of Removable vs Fixed Cribs in Open Bite TreatmentDocumento7 pagineDentoalveolar Effects of Removable vs Fixed Cribs in Open Bite TreatmentTesisTraduccionesRuzelNessuna valutazione finora
- Gap ArthroplastyDocumento5 pagineGap ArthroplastyMax FaxNessuna valutazione finora
- BoltonDocumento26 pagineBoltonDryashpal SinghNessuna valutazione finora
- Prevalence of Gingival Recession After Orthodontic Tooth MovementsDocumento9 paginePrevalence of Gingival Recession After Orthodontic Tooth Movementsaleja_garces_1Nessuna valutazione finora
- Paper No 02Documento7 paginePaper No 02Shyam K MaharjanNessuna valutazione finora
- AJODO-2013 Angelieri 144 5 759Documento11 pagineAJODO-2013 Angelieri 144 5 759osama-alali100% (1)
- Read The Following Abstract of The Journal and Answer The QuestionsDocumento3 pagineRead The Following Abstract of The Journal and Answer The QuestionsichaNessuna valutazione finora
- Predictive Variable For The Outcome of Early Functional Treatment of Class III MaloclussionDocumento7 paginePredictive Variable For The Outcome of Early Functional Treatment of Class III MaloclussionLucy UrrunagaNessuna valutazione finora
- Oroantral Communications. A Retrospective Analysis: Josué Hernando, Lorena Gallego, Luis Junquera, Pedro VillarrealDocumento5 pagineOroantral Communications. A Retrospective Analysis: Josué Hernando, Lorena Gallego, Luis Junquera, Pedro VillarrealPla ParichartNessuna valutazione finora
- m3 CrowdingDocumento6 paginem3 CrowdingAndre KurniawanNessuna valutazione finora
- CLASSIC ARTICLE Clinical Measurement and EvaluationDocumento5 pagineCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- Lip BumperDocumento7 pagineLip BumperMiguel JaènNessuna valutazione finora
- Ameloblastoma of The Jaw and Maxillary Bone: Clinical Study and Report of Our ExperienceDocumento7 pagineAmeloblastoma of The Jaw and Maxillary Bone: Clinical Study and Report of Our ExperienceKharismaNisaNessuna valutazione finora
- Effect of Class III Bone Anchor Treatment On Airway: Tung Nguyen Hugo de Clerck Michael Wilson Brent GoldenDocumento6 pagineEffect of Class III Bone Anchor Treatment On Airway: Tung Nguyen Hugo de Clerck Michael Wilson Brent GoldenQickie AmaliaNessuna valutazione finora
- Fifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated ProcedureDocumento11 pagineFifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated Procedurebendot29Nessuna valutazione finora
- Rare Facial Clefts PDFDocumento6 pagineRare Facial Clefts PDFAntoine NinoNessuna valutazione finora
- Bilateral Adenomatoid Odontogenic Tumour of The Maxilla in A 2-Year-Old Female-The Report of A Rare Case and Review of The LiteratureDocumento7 pagineBilateral Adenomatoid Odontogenic Tumour of The Maxilla in A 2-Year-Old Female-The Report of A Rare Case and Review of The LiteratureStephanie LyonsNessuna valutazione finora
- Referat Pleomorphic AdenomaDocumento6 pagineReferat Pleomorphic AdenomaAsrie Sukawatie PutrieNessuna valutazione finora
- Original Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyDocumento7 pagineOriginal Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyAkanshaNessuna valutazione finora
- Read The Following Abstract of The Journal and Answer The QuestionsDocumento4 pagineRead The Following Abstract of The Journal and Answer The QuestionsNada Syafa TitaniaNessuna valutazione finora
- Three Impression Methods for Loose Edentulous MucosaDocumento3 pagineThree Impression Methods for Loose Edentulous MucosaAgus PudiantoNessuna valutazione finora
- AJODO-99 3er Molar Un Dilema PDFDocumento6 pagineAJODO-99 3er Molar Un Dilema PDFJorge Armando LópezNessuna valutazione finora
- Artigo 1 - Do Infant Cleft Dimensions Have An Influence On Occlusal Relations? A Subgroup Analysis Within An RCT of Primary Surgery in Patients With Unilateral Cleft Lip and PalateDocumento11 pagineArtigo 1 - Do Infant Cleft Dimensions Have An Influence On Occlusal Relations? A Subgroup Analysis Within An RCT of Primary Surgery in Patients With Unilateral Cleft Lip and PalateTalmo DiasNessuna valutazione finora
- Exostosis MandibularDocumento6 pagineExostosis MandibularCOne Gomez LinarteNessuna valutazione finora
- ART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDocumento11 pagineART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDiana Paola FontechaNessuna valutazione finora
- AJODO 1993 Mar 203-211 - Taken From The AJO-DO On CD-ROMDocumento20 pagineAJODO 1993 Mar 203-211 - Taken From The AJO-DO On CD-ROMAndré MéndezNessuna valutazione finora
- Analysis of dentofacial vertical proportionsDocumento23 pagineAnalysis of dentofacial vertical proportionssiddarthNessuna valutazione finora
- Original Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarDocumento5 pagineOriginal Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarjaslinshalinNessuna valutazione finora
- 2014 A Prospective Study of Clinical Outcomes Related To Third Molar Removal or RetentionDocumento7 pagine2014 A Prospective Study of Clinical Outcomes Related To Third Molar Removal or RetentionkaarlaamendezNessuna valutazione finora
- Evaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFDocumento4 pagineEvaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFVictor HernandezNessuna valutazione finora
- Jurnal in EnglishDocumento5 pagineJurnal in Englishyeni_arnasNessuna valutazione finora
- Stability of Extraction Space Closure: Original ArticleDocumento7 pagineStability of Extraction Space Closure: Original ArticleSoe San KyawNessuna valutazione finora
- NPWT OmphaloceleDocumento5 pagineNPWT OmphaloceleMirna Lestari SinurayaNessuna valutazione finora
- Thyroglossal Duct Cyst StudyDocumento7 pagineThyroglossal Duct Cyst StudyAurel OctavianNessuna valutazione finora
- Class 11 Elastics and Extractions and Temporomandibular Disorders - A Longitudinal Prospective StudyDocumento5 pagineClass 11 Elastics and Extractions and Temporomandibular Disorders - A Longitudinal Prospective StudyValery V JaureguiNessuna valutazione finora
- Treatment Algorithm For Ameloblastoma RRDocumento30 pagineTreatment Algorithm For Ameloblastoma RRpanjidrgNessuna valutazione finora
- 11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The LiteratureDocumento11 pagine11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The Literaturekochikaghochi100% (1)
- Differential Premolar ExtractionDocumento7 pagineDifferential Premolar Extractionplazari07Nessuna valutazione finora
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementDa EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNessuna valutazione finora
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideDa EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNessuna valutazione finora
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementDa EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNessuna valutazione finora
- Review FrenectomyDocumento6 pagineReview FrenectomyNyitnyit KunyitNessuna valutazione finora
- Edwards 1977 Diastema and FrenumDocumento20 pagineEdwards 1977 Diastema and FrenumjeremyvoNessuna valutazione finora
- 11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The LiteratureDocumento11 pagine11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The Literaturekochikaghochi100% (1)
- Albandar 2002 Epidemiology North AmericaDocumento39 pagineAlbandar 2002 Epidemiology North AmericajeremyvoNessuna valutazione finora
- Grassi 1987 Perio Pocket Healing Following ExtractionDocumento7 pagineGrassi 1987 Perio Pocket Healing Following ExtractionjeremyvoNessuna valutazione finora
- Ibbott 1986 Extractions in PerioDocumento3 pagineIbbott 1986 Extractions in PeriojeremyvoNessuna valutazione finora
- Kugelberg 1985 Periodontal Healing After Exo WisdomDocumento12 pagineKugelberg 1985 Periodontal Healing After Exo WisdomjeremyvoNessuna valutazione finora
- Kao 2009 Strategic Extraction PerioDocumento7 pagineKao 2009 Strategic Extraction PeriojeremyvoNessuna valutazione finora
- PeriodonticsDocumento17 paginePeriodonticsKrishan GuliaNessuna valutazione finora
- Corn 1969 Extractions PerioDocumento28 pagineCorn 1969 Extractions PeriojeremyvoNessuna valutazione finora
- Meng 1999 Aap Annals Perio EndoDocumento6 pagineMeng 1999 Aap Annals Perio EndojeremyvoNessuna valutazione finora
- Donos 2012 Teeth Vs Implants DilemmaDocumento22 pagineDonos 2012 Teeth Vs Implants DilemmajeremyvoNessuna valutazione finora
- Cobb 2009 Is Prevalence of Perio in DeclineDocumento12 pagineCobb 2009 Is Prevalence of Perio in DeclinejeremyvoNessuna valutazione finora
- Albandar 2002 Global Epidemiology OverviewDocumento4 pagineAlbandar 2002 Global Epidemiology OverviewjeremyvoNessuna valutazione finora
- 473Documento8 pagine473Kamonrat LimNessuna valutazione finora
- Vandenberghe 2007 Cone Beam Perio DiagnosisDocumento7 pagineVandenberghe 2007 Cone Beam Perio DiagnosisjeremyvoNessuna valutazione finora
- Pack 1999 Endo Perio PDFDocumento4 paginePack 1999 Endo Perio PDFjeremyvoNessuna valutazione finora
- Monsour 2008 Radiography ImplantsDocumento15 pagineMonsour 2008 Radiography ImplantsjeremyvoNessuna valutazione finora
- Dahlen 2002 Micro Abscess and Perio EndoDocumento34 pagineDahlen 2002 Micro Abscess and Perio EndojeremyvoNessuna valutazione finora
- Periodontology 2000 La Controversia Endodoncia PeriodonciaDocumento8 paginePeriodontology 2000 La Controversia Endodoncia PeriodonciaEdos De la Barra100% (2)
- Misch 2006 Cone Beam DiagnosisDocumento6 pagineMisch 2006 Cone Beam DiagnosisjeremyvoNessuna valutazione finora
- Albrektsson Foreign Body ReactionDocumento11 pagineAlbrektsson Foreign Body ReactionjeremyvoNessuna valutazione finora
- محاضرة الدكتور وسام الجنابيDocumento2 pagineمحاضرة الدكتور وسام الجنابيtath9076Nessuna valutazione finora
- History of Dental HygieneDocumento3 pagineHistory of Dental HygieneDara Pangestika Dwi AnggraeniNessuna valutazione finora
- Principles of Endodontic SurgeryDocumento29 paginePrinciples of Endodontic SurgeryCristina Ene100% (3)
- Fissure TongueDocumento2 pagineFissure Tonguebundahara zoomNessuna valutazione finora
- 22 CE CreditsDocumento11 pagine22 CE CreditsAhmed BadrNessuna valutazione finora
- Lec.3 Survying in ProsthodonticDocumento14 pagineLec.3 Survying in ProsthodonticSarah SafiraNessuna valutazione finora
- Pulpal Diseases: Batul Bohra Jinal Bhanushali Neha BharwadDocumento63 paginePulpal Diseases: Batul Bohra Jinal Bhanushali Neha BharwadKhyati RachchhNessuna valutazione finora
- The Influence of Extrinsic Coloration Factors On CompositesDocumento8 pagineThe Influence of Extrinsic Coloration Factors On CompositesDeasireeNessuna valutazione finora
- 0002 9416 (58) 90024 1Documento12 pagine0002 9416 (58) 90024 1Durga VoraNessuna valutazione finora
- Dental adhesive techniquesDocumento40 pagineDental adhesive techniquesIuliana MîrzaNessuna valutazione finora
- Multiple Choice Question (MCQ) Exam: 15 Sample QuestionsDocumento4 pagineMultiple Choice Question (MCQ) Exam: 15 Sample QuestionsAnkita AgarwallNessuna valutazione finora
- Bicon Short Implant 2Documento6 pagineBicon Short Implant 2Bicon Implant InaNessuna valutazione finora
- Pedo Papers (Feb21 To July12)Documento36 paginePedo Papers (Feb21 To July12)thenmozhi thenmozhiNessuna valutazione finora
- Effects of Restorative Procedure On Um PerioDocumento38 pagineEffects of Restorative Procedure On Um PerioFourthMolar.comNessuna valutazione finora
- Wala RidgeDocumento6 pagineWala Ridgekatherine100% (1)
- Oral Pathology QuestionsDocumento19 pagineOral Pathology QuestionsBhoomikaNessuna valutazione finora
- Tufts - PathDocumento29 pagineTufts - PathRami SalhaNessuna valutazione finora
- Oral Histology Quiz - True False (AmCoFam)Documento35 pagineOral Histology Quiz - True False (AmCoFam)AmericanCornerFamily88% (8)
- Anatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Documento4 pagineAnatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Purnama SyahbaniNessuna valutazione finora
- Mouth Care For An Unconcious Patient (2201)Documento5 pagineMouth Care For An Unconcious Patient (2201)Maggie LiNessuna valutazione finora
- Delayed Molar Development and Eruption CaseDocumento3 pagineDelayed Molar Development and Eruption CaseNadya PurwantyNessuna valutazione finora
- Preparation of AbutmentDocumento3 paginePreparation of AbutmentSiti FerianiNessuna valutazione finora
- Marginal Gingiva: ArcuateDocumento1 paginaMarginal Gingiva: ArcuateIrene QuimsonNessuna valutazione finora
- All-Ceramic Restorations - : ZR-DiamondsDocumento2 pagineAll-Ceramic Restorations - : ZR-DiamondsDemmy WijayaNessuna valutazione finora
- Cogs ShafeesDocumento20 pagineCogs ShafeesMariyamNessuna valutazione finora
- Sirona 3D Summit ProgramDocumento8 pagineSirona 3D Summit Programjeff_way100% (3)
- Patients' Perceptions and Concerns About Orthodontic TreatmentDocumento9 paginePatients' Perceptions and Concerns About Orthodontic TreatmentSkAliHassanNessuna valutazione finora
- Consequences of Implant Design: Archie A. Jones, DDS, David L. Cochran, PHD, DdsDocumento1 paginaConsequences of Implant Design: Archie A. Jones, DDS, David L. Cochran, PHD, Ddsdr parveen bathlaNessuna valutazione finora