Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elsevier 1 N08Documento270 pagineElsevier 1 N08criticald0% (1)
- Replikasi, Transkripsi Dan Translasi DnaDocumento19 pagineReplikasi, Transkripsi Dan Translasi DnaEllizabeth LilantiNessuna valutazione finora
- DP1 SL Unit AssessmentDocumento12 pagineDP1 SL Unit AssessmentNihad Gully100% (1)
- Fluorescence Insitu HybridisationDocumento9 pagineFluorescence Insitu Hybridisationtorseeker1100% (1)
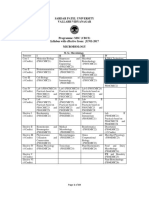
- MSC Microbiology SyllabusDocumento9 pagineMSC Microbiology SyllabusArjun ShethNessuna valutazione finora
- Glycolysis: Glycolysis (From Glycose, An Older TermDocumento3 pagineGlycolysis: Glycolysis (From Glycose, An Older TermProff AhengNessuna valutazione finora
- Chapter 12 DNA and RNA ReviewDocumento6 pagineChapter 12 DNA and RNA ReviewAndrew WatsonNessuna valutazione finora
- 2.2 Cellular Components - Chloroplast, Golgi Apparatus & Lysosomes (Essay Question)Documento2 pagine2.2 Cellular Components - Chloroplast, Golgi Apparatus & Lysosomes (Essay Question)HUSNA 83Nessuna valutazione finora
- Worksheet 2 Cell StructureDocumento4 pagineWorksheet 2 Cell StructurenathanNessuna valutazione finora
- 04-08-09 Athersys Slides (Investor Day - Final)Documento122 pagine04-08-09 Athersys Slides (Investor Day - Final)MattNessuna valutazione finora
- DNA TranslastionDocumento2 pagineDNA TranslastionJoySe Merrera ÜNessuna valutazione finora
- Molecular Biology of The CellDocumento129 pagineMolecular Biology of The CellAndres Sanchez EscobedoNessuna valutazione finora
- Microglia in Alzheimer's Disease: A Target For ImmunotherapyDocumento9 pagineMicroglia in Alzheimer's Disease: A Target For ImmunotherapyCarlos Hutarra DiazNessuna valutazione finora
- Hershey ChaseDocumento1 paginaHershey Chasemkohli64Nessuna valutazione finora
- Post-Translational Modification - WikipediaDocumento62 paginePost-Translational Modification - Wikipediamuskan yadavNessuna valutazione finora
- Forensics 12-13 TestDocumento3 pagineForensics 12-13 Testmemmy3697Nessuna valutazione finora
- Protein Synthesis تصنيع البروتينDocumento12 pagineProtein Synthesis تصنيع البروتينBra himNessuna valutazione finora
- Blacklisted Journals by Malaysia Ministry of Education by Publisher PDFDocumento6 pagineBlacklisted Journals by Malaysia Ministry of Education by Publisher PDFanon_628099982Nessuna valutazione finora
- Tm10. Wan-Tai - Sars Cov2Documento8 pagineTm10. Wan-Tai - Sars Cov22240020002 AFRIDA CAHYA MAHARANINessuna valutazione finora
- 2211-5463 12453 PDFDocumento392 pagine2211-5463 12453 PDFAkash RajNessuna valutazione finora
- Kuliah Umum TransfusiDocumento54 pagineKuliah Umum TransfusiAnton TriyadiNessuna valutazione finora
- Drug Target and Drug Receptor InteractionDocumento42 pagineDrug Target and Drug Receptor InteractionAceng Nunu NNessuna valutazione finora
- Lecture 1 & 2 Bioprocess Technology: SCBT 32113Documento58 pagineLecture 1 & 2 Bioprocess Technology: SCBT 32113AkshayaaRaveeNessuna valutazione finora
- Winston Jonas BrillDocumento4 pagineWinston Jonas BrillNego Gooners GankNessuna valutazione finora
- Fundamentals of Biological MS and Proteomics Carr 5 15 PDFDocumento43 pagineFundamentals of Biological MS and Proteomics Carr 5 15 PDFCarlos Julio Nova LopezNessuna valutazione finora
- Mastermind: WorksheetDocumento25 pagineMastermind: WorksheetMilka RahmanNessuna valutazione finora
- Blotting TechniquesDocumento28 pagineBlotting TechniquesJoshua MuegoNessuna valutazione finora
- Basic Principles of HistologyDocumento10 pagineBasic Principles of HistologyDonto KonoNessuna valutazione finora
- Lecture Note - Introduction To GeneticsDocumento35 pagineLecture Note - Introduction To GeneticsMasni Shah NingNessuna valutazione finora
- Intro To Workshop All in PersonDocumento17 pagineIntro To Workshop All in PersonYanelisa PulaniNessuna valutazione finora