Potrebbero piacerti anche
- Academic Medical Accelerators Revised2Documento50 pagineAcademic Medical Accelerators Revised2sushmita singhNessuna valutazione finora
- Innovative Radiotherapy Techniques for Prostate CancerDa EverandInnovative Radiotherapy Techniques for Prostate CancerNessuna valutazione finora
- Aapm Report No. 16 Protocol For HeavyDocumento60 pagineAapm Report No. 16 Protocol For HeavyLaurentiu RadoiNessuna valutazione finora
- Neutron Field Inside A PET Cyclotron Vault RoomDocumento7 pagineNeutron Field Inside A PET Cyclotron Vault RoomFelipe Cristobal Rivera RojasNessuna valutazione finora
- Quality Assurance For MRI by AAPMDocumento38 pagineQuality Assurance For MRI by AAPMNikosNessuna valutazione finora
- Nuclear Medicine Tehnologist or Lead Nuclear Medicine TechnologiDocumento2 pagineNuclear Medicine Tehnologist or Lead Nuclear Medicine Technologiapi-78955179Nessuna valutazione finora
- Solutions: Radiation Medicine QaDocumento128 pagineSolutions: Radiation Medicine QaHashir SaeedNessuna valutazione finora
- ICRU Report 10bDocumento115 pagineICRU Report 10bЕвгений ГольдманNessuna valutazione finora
- MammographyDocumento84 pagineMammographyCeles Nilleny UchihaNessuna valutazione finora
- ICRU Report 62 Prescribing Recording and Reporting Photon Beam Therapy (Supplment To ICRU Report 50)Documento62 pagineICRU Report 62 Prescribing Recording and Reporting Photon Beam Therapy (Supplment To ICRU Report 50)Jose Miguel Oyarzun SilvaNessuna valutazione finora
- Icru 78 Proton TherapyDocumento217 pagineIcru 78 Proton TherapyMigue PerezNessuna valutazione finora
- Achytherapy 3HAXAPDocumento464 pagineAchytherapy 3HAXAPIkang FauziNessuna valutazione finora
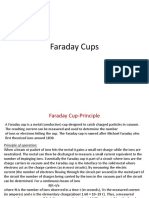
- Faraday CupsDocumento10 pagineFaraday CupsAshish SharmaNessuna valutazione finora
- Senior Radiographer Nuclear MedicineDocumento1 paginaSenior Radiographer Nuclear Medicinetafi66Nessuna valutazione finora
- Manual de Usuario PTW PDFDocumento27 pagineManual de Usuario PTW PDFJorge CifuentesNessuna valutazione finora
- Nuclear Medicine Case StudyDocumento6 pagineNuclear Medicine Case StudyPrashant NagpureNessuna valutazione finora
- AAPM 34 - MRI Acceptance TestDocumento16 pagineAAPM 34 - MRI Acceptance TestmahbodsedNessuna valutazione finora
- 2014 02 28 Item 2 AERB IBA Radiation Safety AspectsDocumento27 pagine2014 02 28 Item 2 AERB IBA Radiation Safety AspectsSUBHANessuna valutazione finora
- FluroscophyDocumento39 pagineFluroscophyfathahillahNessuna valutazione finora
- AAPM-TG53 (Quality Assurance For Clinical RTP)Documento57 pagineAAPM-TG53 (Quality Assurance For Clinical RTP)ΜΡ_Nessuna valutazione finora
- On-Board Imaging System - Board Imaging System HammoudQADocumento120 pagineOn-Board Imaging System - Board Imaging System HammoudQAyumekiNessuna valutazione finora
- QA Procedure For SRS TataDocumento7 pagineQA Procedure For SRS TataMayuri NathNessuna valutazione finora
- Nuclear Medicine GuideDocumento3 pagineNuclear Medicine GuidejeffsunilNessuna valutazione finora
- Truebeam CollimationDocumento6 pagineTruebeam Collimationzhen yongjieNessuna valutazione finora
- myQA Daily Users GuideDocumento87 paginemyQA Daily Users GuideDaniela ZanchiNessuna valutazione finora
- RSL-D-RS-7.0-SEG-EN-1.0-2017-12-08 RayStation 7 System Environment Guidelines PDFDocumento42 pagineRSL-D-RS-7.0-SEG-EN-1.0-2017-12-08 RayStation 7 System Environment Guidelines PDFAndres MoyaNessuna valutazione finora
- Thesis On TWTDocumento181 pagineThesis On TWTarshad aliNessuna valutazione finora
- Cyclotron Training - Part 1 - BasicsDocumento31 pagineCyclotron Training - Part 1 - BasicsHariNessuna valutazione finora
- Basic Considerations in Nuclear MedicineDocumento12 pagineBasic Considerations in Nuclear Medicinechberg13Nessuna valutazione finora
- F-18 NaFDocumento47 pagineF-18 NaFLadipo Temitope AyodejiNessuna valutazione finora
- Brachy PDFDocumento67 pagineBrachy PDFPhys YarmoukNessuna valutazione finora
- Chapter 3 - Introduction To Nuclear MedicineDocumento4 pagineChapter 3 - Introduction To Nuclear MedicineunknownxemNessuna valutazione finora
- Huq CT SimulatorDocumento65 pagineHuq CT SimulatorEskadmas BelayNessuna valutazione finora
- Icru 82Documento67 pagineIcru 82Aditya DisdusNessuna valutazione finora
- Radiation TherapyDocumento69 pagineRadiation TherapyRamesh BabuNessuna valutazione finora
- Stonelith V5Documento9 pagineStonelith V5Wistara Zavier Wahyu100% (1)
- Cherenkov RadiationDocumento17 pagineCherenkov RadiationMayank GargNessuna valutazione finora
- Radiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)Documento208 pagineRadiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)Eskadmas BelayNessuna valutazione finora
- Beam Modification FinalDocumento50 pagineBeam Modification Finalapi-3726116100% (5)
- Body MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveDocumento19 pagineBody MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveaegysabetterwayNessuna valutazione finora
- 3D Dose Computation AlgorithmsDocumento10 pagine3D Dose Computation AlgorithmsHashir SaeedNessuna valutazione finora
- Qa PhysicsDocumento4 pagineQa PhysicstuNessuna valutazione finora
- Dosimetric Effects of Using Generalized Equivalent Uniform Dose (gEUD) in Plan OptimizationDocumento60 pagineDosimetric Effects of Using Generalized Equivalent Uniform Dose (gEUD) in Plan OptimizationolgaNessuna valutazione finora
- Iaea TRS 430Documento302 pagineIaea TRS 430Alvaro Hermosilla ManríquezNessuna valutazione finora
- Nuclear Medicine Instrumentation QC GUIDELINES Maria Lyra Et Al 2007Documento69 pagineNuclear Medicine Instrumentation QC GUIDELINES Maria Lyra Et Al 2007knno87Nessuna valutazione finora
- Task Group No. 43-U1Documento44 pagineTask Group No. 43-U1fazli.samarNessuna valutazione finora
- Independent Dose Calculations Concepts and ModelsDocumento104 pagineIndependent Dose Calculations Concepts and ModelsMuhammad Nauman UsmaniNessuna valutazione finora
- Medical Physics ResourcesDocumento10 pagineMedical Physics ResourceschanderNessuna valutazione finora
- Aapm TG 142 PDFDocumento47 pagineAapm TG 142 PDFAde RianaNessuna valutazione finora
- Haris Linear AcceleratorDocumento66 pagineHaris Linear AcceleratorHarisrahmanNessuna valutazione finora
- CT Basics - Part 1Documento27 pagineCT Basics - Part 1bahadirerNessuna valutazione finora
- Icrp 135Documento144 pagineIcrp 135Roshi_11Nessuna valutazione finora
- Radiology Lectures On UdemyDocumento1 paginaRadiology Lectures On UdemySrirupa BiswasNessuna valutazione finora
- Detecting and Measuring Radiation Lect 4Documento22 pagineDetecting and Measuring Radiation Lect 4Tonyo LinaNessuna valutazione finora
- Fluroscopy & Iitv SystemDocumento87 pagineFluroscopy & Iitv SystemMunish DograNessuna valutazione finora
- Advances in Medical Linear Accelerator TechnologyDocumento22 pagineAdvances in Medical Linear Accelerator TechnologyNawel MorjanNessuna valutazione finora
- Data Teknis EKG Fukuda Denshi FX-7542Documento2 pagineData Teknis EKG Fukuda Denshi FX-7542darmayunitaNessuna valutazione finora
- Accelerator Design For Proton Therapy: OutlineDocumento8 pagineAccelerator Design For Proton Therapy: OutlineriomjNessuna valutazione finora
- Cancer Center: Tomotherapy'S Implementation of Image-Guided Adaptive Radiation TherapyDocumento94 pagineCancer Center: Tomotherapy'S Implementation of Image-Guided Adaptive Radiation TherapyMalu Paras LacsonNessuna valutazione finora
- Final Qa ChartDocumento20 pagineFinal Qa Chartapi-280277788Nessuna valutazione finora
- Planning Strategies For Inter-Fractional Robustness in Pancreatic Patients Treated With Scanned Carbon TherapyDocumento9 paginePlanning Strategies For Inter-Fractional Robustness in Pancreatic Patients Treated With Scanned Carbon TherapyVania BatistaNessuna valutazione finora
- RStudio ExercicesDocumento8 pagineRStudio ExercicesVania BatistaNessuna valutazione finora
- Dosimetric Consequences of Pencil Beam Width Variations in Scanned Beam Particle TherapyDocumento16 pagineDosimetric Consequences of Pencil Beam Width Variations in Scanned Beam Particle TherapyVania BatistaNessuna valutazione finora
- The Demons AlgorithmDocumento12 pagineThe Demons AlgorithmVania BatistaNessuna valutazione finora
- Booklet n3 Physics For ClinrtDocumento166 pagineBooklet n3 Physics For Clinrtjts99athotmaildotcomNessuna valutazione finora
- AAPM Task 43Documento29 pagineAAPM Task 43Vania BatistaNessuna valutazione finora
- Asme Interpre Sec Vii D 1Documento60 pagineAsme Interpre Sec Vii D 1Mayrita Nicol Aranibar TiconaNessuna valutazione finora
- Ramzan Timetable Grade IX-ADocumento1 paginaRamzan Timetable Grade IX-AMBJNessuna valutazione finora
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Documento12 pagineDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Iqioo RedefiniNessuna valutazione finora
- Enhanced Degradation of Persistent Pharmaceuticals Found in Wastewater Treatment Ef Uents Using Tio2 Nanobelt PhotocatalystsDocumento14 pagineEnhanced Degradation of Persistent Pharmaceuticals Found in Wastewater Treatment Ef Uents Using Tio2 Nanobelt PhotocatalystsSourav SutradharNessuna valutazione finora
- Modelling and Simulation of The Three-Phase Induction Motor Using SimulinkDocumento10 pagineModelling and Simulation of The Three-Phase Induction Motor Using SimulinkÁron FehérNessuna valutazione finora
- APFF 1896 Introduction of 750W MotorDocumento7 pagineAPFF 1896 Introduction of 750W MotorjakaNessuna valutazione finora
- Shreyas Pawale ResumeDocumento1 paginaShreyas Pawale ResumeRahulRajGoldyNessuna valutazione finora
- BME473 Homework 4Documento6 pagineBME473 Homework 4telatoyoNessuna valutazione finora
- (CO5) Chemical EquilibriumDocumento35 pagine(CO5) Chemical EquilibriumAya Evangelista AlmandresNessuna valutazione finora
- Daftar Pustaka Tugas Akhir Planetarium Dan ObservatoriumDocumento4 pagineDaftar Pustaka Tugas Akhir Planetarium Dan ObservatoriumAzurieMegNessuna valutazione finora
- 1927 06 The Electric ArcDocumento16 pagine1927 06 The Electric ArcdeyvimaycolNessuna valutazione finora
- The Epoxy BookDocumento37 pagineThe Epoxy BookEvTech PhilNessuna valutazione finora
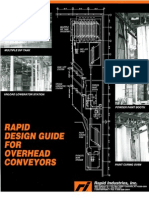
- Design GuideDocumento30 pagineDesign Guiderapidindustries100% (6)
- Analysis of VOltage and Power Interactions in Multi-Infeed HVDC SystemsDocumento9 pagineAnalysis of VOltage and Power Interactions in Multi-Infeed HVDC SystemstinazdrilicNessuna valutazione finora
- Intro To Auto Control PDFDocumento15 pagineIntro To Auto Control PDFJacksonWilliamRyderNessuna valutazione finora
- Reed Cog Psych 1972Documento26 pagineReed Cog Psych 1972Abhinav JhaNessuna valutazione finora
- Blast Resistant Design With Structural Steel PDFDocumento6 pagineBlast Resistant Design With Structural Steel PDFMatthieuNessuna valutazione finora
- Fieldwork No. 6 Laying of A Symmetrical Parabolic Curve Using Transit and TapeDocumento4 pagineFieldwork No. 6 Laying of A Symmetrical Parabolic Curve Using Transit and TapeRyana Camille RoldanNessuna valutazione finora
- (Lab Report Operation Unit) Experiment 3: Separation of An Ordinary Binary Mixture Consisting of Acetic Acid and Water by Using Simple Batch Distillation Technique.Documento8 pagine(Lab Report Operation Unit) Experiment 3: Separation of An Ordinary Binary Mixture Consisting of Acetic Acid and Water by Using Simple Batch Distillation Technique.Fazsroul100% (9)
- Homeopathic Materia Medica PDFDocumento216 pagineHomeopathic Materia Medica PDFRavi Ranjan Jha100% (1)
- Basic Concepts Electrical CircuitsDocumento38 pagineBasic Concepts Electrical CircuitslakshmiraniNessuna valutazione finora
- A Study of Verbs Compounded With Aus, Ein, Etc., As Contrasted With Those Compounded With Heraus, Hinaus, Herain, Hinein, EtcDocumento152 pagineA Study of Verbs Compounded With Aus, Ein, Etc., As Contrasted With Those Compounded With Heraus, Hinaus, Herain, Hinein, EtcEnkindooNessuna valutazione finora
- (COMPLETE) Ring Ball and Penetration Test PDFDocumento10 pagine(COMPLETE) Ring Ball and Penetration Test PDFAthirah DinataNessuna valutazione finora
- Acoustic Emission March 2004 - Back To BasicsDocumento16 pagineAcoustic Emission March 2004 - Back To BasicsfndandanNessuna valutazione finora
- BioisosterismDocumento22 pagineBioisosterismpurnima singhNessuna valutazione finora
- Amulet 9-Waverider TextDocumento240 pagineAmulet 9-Waverider Text20170775Nessuna valutazione finora
- CNC Router CalculationsDocumento4 pagineCNC Router Calculationsmorteza nourooziNessuna valutazione finora
- Numerical Inversion of Laplace Transforms in MatlabDocumento4 pagineNumerical Inversion of Laplace Transforms in MatlabErza ScarletNessuna valutazione finora
- Projects Titles For Protection - W2017Documento3 pagineProjects Titles For Protection - W2017Ahmad AbunassarNessuna valutazione finora
- Rr211402 Mechanics of SolidsDocumento8 pagineRr211402 Mechanics of SolidsSrinivasa Rao GNessuna valutazione finora