Potrebbero piacerti anche
- Peripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFDocumento9 paginePeripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFAngela PagliusoNessuna valutazione finora
- Peripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFDocumento9 paginePeripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFAngela PagliusoNessuna valutazione finora
- C MaxwellDocumento4 pagineC MaxwellAngela PagliusoNessuna valutazione finora
- The Acumoxa Treatment of Shoulder Impingement SyndromeDocumento8 pagineThe Acumoxa Treatment of Shoulder Impingement SyndromeAngela PagliusoNessuna valutazione finora
- Pens Ta 01132004Documento9 paginePens Ta 01132004Angela PagliusoNessuna valutazione finora
- Agopuntura Per StrokeDocumento14 pagineAgopuntura Per StrokeAngela PagliusoNessuna valutazione finora
- J J Rad Oncol 3 2 029-2Documento4 pagineJ J Rad Oncol 3 2 029-2Angela PagliusoNessuna valutazione finora
- SMW 10163 PDFDocumento9 pagineSMW 10163 PDFAngela PagliusoNessuna valutazione finora
- 0100 7203 Rbgo 37 03 00105Documento5 pagine0100 7203 Rbgo 37 03 00105Angela PagliusoNessuna valutazione finora
- Deciphering - Pse .2012Documento11 pagineDeciphering - Pse .2012Angela PagliusoNessuna valutazione finora
- 2006 ICAET SmallDocumento32 pagine2006 ICAET SmallAngela PagliusoNessuna valutazione finora
- Panjabi Stabilizing System PDFDocumento8 paginePanjabi Stabilizing System PDFAngela PagliusoNessuna valutazione finora
- Electromedicine - The Other Side of PhysiologyDocumento11 pagineElectromedicine - The Other Side of PhysiologyAngela PagliusoNessuna valutazione finora
- Electromedicine - The Other Side of PhysiologyDocumento11 pagineElectromedicine - The Other Side of PhysiologyAngela PagliusoNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Assessing Musculoskeletal System: FEU - Institute of Nursing Health AssessmentDocumento13 pagineAssessing Musculoskeletal System: FEU - Institute of Nursing Health AssessmentJancee Harri Leynes MelendresNessuna valutazione finora
- Riva 44' RIVARAMA - Lady MDocumento15 pagineRiva 44' RIVARAMA - Lady MskoiperNessuna valutazione finora
- Mansions of Madness Second Editon Rules ReferenceDocumento24 pagineMansions of Madness Second Editon Rules ReferenceGeorge AlexandrisNessuna valutazione finora
- 4AT Automatic TransDocumento126 pagine4AT Automatic TransdrNessuna valutazione finora
- 5 Elements Qi GongDocumento1 pagina5 Elements Qi GongBill HonakerNessuna valutazione finora
- Fitness His Edition JulyAugust 2017Documento84 pagineFitness His Edition JulyAugust 2017Afzal FeerestaNessuna valutazione finora
- MC Hammer - U Can't Touch ThisDocumento2 pagineMC Hammer - U Can't Touch ThiscanalemptyrockNessuna valutazione finora
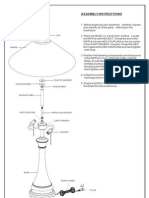
- Assembly Instructions: FinialDocumento1 paginaAssembly Instructions: Finialdayshift5Nessuna valutazione finora
- General Merit List BS 4 Years Criminology Replica 202127Documento16 pagineGeneral Merit List BS 4 Years Criminology Replica 202127Ch bilal Ch bilalNessuna valutazione finora
- Modul1 Bahasa Inggris Kelas 6 KD 3.1 - 4.1Documento18 pagineModul1 Bahasa Inggris Kelas 6 KD 3.1 - 4.1Festya AfrianiNessuna valutazione finora
- Collective Past Board Exam Questionnaire (PROFESSIONAL PRACTICE)Documento5 pagineCollective Past Board Exam Questionnaire (PROFESSIONAL PRACTICE)Erwin AriolaNessuna valutazione finora
- Transmission NoiseDocumento5 pagineTransmission Noiseأحمد دعبس100% (1)
- Angles Formed by Parallel Lines and TransversalDocumento36 pagineAngles Formed by Parallel Lines and TransversalHanna Grace Honrade100% (1)
- Installation Tutorial For Console Customs Ps4 Truefire-Flex Rapid Fire ModDocumento10 pagineInstallation Tutorial For Console Customs Ps4 Truefire-Flex Rapid Fire ModfabiobonadiaNessuna valutazione finora
- Resistance TrainingDocumento4 pagineResistance TrainingRuchelle Denice Demaisip IINessuna valutazione finora
- Past Simple - Past Continuous WorksheetDocumento3 paginePast Simple - Past Continuous WorksheetJeison Ardila100% (1)
- 2880132-CC Free Battle DemoDocumento7 pagine2880132-CC Free Battle DemoKacperNessuna valutazione finora
- CB Golf 2010 2011Documento89 pagineCB Golf 2010 2011mail_markhawleyNessuna valutazione finora
- Skull Thoracic Cage (Ribs and Sternum) Facial Bones Cranium: Chapter 7 - The SkeletonDocumento45 pagineSkull Thoracic Cage (Ribs and Sternum) Facial Bones Cranium: Chapter 7 - The SkeletonSoua YangNessuna valutazione finora
- Sports Magazine FF2Documento124 pagineSports Magazine FF2Ayaz Ahmed KhanNessuna valutazione finora
- Knight Endings Knight Has Restricted MobilityDocumento33 pagineKnight Endings Knight Has Restricted Mobilitygauchao100% (1)
- 350 EXC-F USA 2012: Spare Parts Manual: EngineDocumento28 pagine350 EXC-F USA 2012: Spare Parts Manual: EnginecharlesNessuna valutazione finora
- Champ Handbook v1 Amtgard WestmarchDocumento40 pagineChamp Handbook v1 Amtgard WestmarchLacey ArvinNessuna valutazione finora
- Janome 6260QCDocumento20 pagineJanome 6260QCbianchifanNessuna valutazione finora
- Phed04020-Module 2 - BasketballDocumento25 paginePhed04020-Module 2 - BasketballEdnalyn BalicoNessuna valutazione finora
- Set ArtrosoDocumento8 pagineSet ArtrosoDaniela Carvallo BarriosNessuna valutazione finora
- Just Uploaded To DownloadDocumento4 pagineJust Uploaded To DownloadZachyboiNessuna valutazione finora
- Mazda Fn4A-El 4 Speed Ford 4F27E 4 Speed Fnr5 5 SpeedDocumento5 pagineMazda Fn4A-El 4 Speed Ford 4F27E 4 Speed Fnr5 5 SpeedJulio Bit IxcameyNessuna valutazione finora
- Motorcyslist Training Course: Student HandbookDocumento98 pagineMotorcyslist Training Course: Student Handbookivillacortaav2009Nessuna valutazione finora
- 2009 Pure Polaris Catalog: Atv / Side X Side Accessories & ApparelDocumento254 pagine2009 Pure Polaris Catalog: Atv / Side X Side Accessories & Apparelproton666live.ruNessuna valutazione finora