Potrebbero piacerti anche
- Assessment of Head and NeckDocumento11 pagineAssessment of Head and Neckjacnpoy100% (2)
- Assessment of The Head and NeckDocumento4 pagineAssessment of The Head and NeckA R F I J U LNessuna valutazione finora
- Checklist Assessment of The Eyes and Visual Acuity2021 22Documento3 pagineChecklist Assessment of The Eyes and Visual Acuity2021 22Trisha SabaNessuna valutazione finora
- NYU PGY-2 Ophthalmology Basics Guide: D1 (3) .GifDocumento27 pagineNYU PGY-2 Ophthalmology Basics Guide: D1 (3) .GiftraceyNessuna valutazione finora
- Proforma For Thesis of Master of Suregry (Ophthalmology) Deen Dayal Upadhyaya University, Gorakhpur U.PDocumento18 pagineProforma For Thesis of Master of Suregry (Ophthalmology) Deen Dayal Upadhyaya University, Gorakhpur U.PSumit Kumar GuptaNessuna valutazione finora
- Devgan Phaco Fundamentals B.-1Documento29 pagineDevgan Phaco Fundamentals B.-1asish75100% (3)
- Performing Physical Assessment of The EyeDocumento14 paginePerforming Physical Assessment of The Eyezyrine jhen100% (1)
- Assessment of The EyesDocumento32 pagineAssessment of The EyesArlyn Mendenilla100% (1)
- The EyeDocumento8 pagineThe Eyezyrine jhen100% (1)
- Head To Toe AssessmentDocumento22 pagineHead To Toe AssessmentNessa Layos MorilloNessuna valutazione finora
- Assessment of The EyesDocumento32 pagineAssessment of The EyesArlyn MendenillaNessuna valutazione finora
- Breast Health Assessment Final2Documento17 pagineBreast Health Assessment Final2Petra Sarran100% (1)
- Eye and Vision DisordersDocumento19 pagineEye and Vision DisordersTeena Duray100% (3)
- Eye AssessmentDocumento123 pagineEye Assessmentjaypee01100% (1)
- (Murag Ga Tinan - Away Ra Ta Ani Na Part From # 1-4) : Appearance and BehaviourDocumento3 pagine(Murag Ga Tinan - Away Ra Ta Ani Na Part From # 1-4) : Appearance and BehaviourKaissa GomezNessuna valutazione finora
- Ear AssessmentDocumento5 pagineEar AssessmentJake Amor100% (3)
- Assessment of Skin, Hair and Nails FinaleDocumento7 pagineAssessment of Skin, Hair and Nails FinaleCristine SyNessuna valutazione finora
- HEAD TO TOE ASSESSMENT With PatientDocumento8 pagineHEAD TO TOE ASSESSMENT With PatientCristoper BodionganNessuna valutazione finora
- Assessing The Heart and Neck VesselsDocumento6 pagineAssessing The Heart and Neck VesselsA R F I J U LNessuna valutazione finora
- Session 5 - Assessment Techniques in Clinical SettingDocumento18 pagineSession 5 - Assessment Techniques in Clinical SettingCres Padua QuinzonNessuna valutazione finora
- Skin, Hair and Nails Ok - CompressedDocumento67 pagineSkin, Hair and Nails Ok - CompressedFelya Elsa Pratiwi KurniaNessuna valutazione finora
- Physical AssessmentDocumento24 paginePhysical AssessmentKathleen Felipe DantesNessuna valutazione finora
- HA Breast & AxillaDocumento27 pagineHA Breast & AxillaDarran Earl GowingNessuna valutazione finora
- Gandulfo - Physical AssessmentDocumento3 pagineGandulfo - Physical AssessmentReese Alessandra GandulfoNessuna valutazione finora
- Compartment Syndrome: Return To TopDocumento3 pagineCompartment Syndrome: Return To TopSania Kamal BalweelNessuna valutazione finora
- PALPATION QUESTIONS: Any Pain With That? Tenderness?Documento11 paginePALPATION QUESTIONS: Any Pain With That? Tenderness?Yolly Anne HipolitoNessuna valutazione finora
- Nursing Is An ArtDocumento6 pagineNursing Is An ArtJo PigarNessuna valutazione finora
- Wound DressingDocumento9 pagineWound Dressingapi-3722051100% (2)
- Therapeutic Communication TechniquesDocumento2 pagineTherapeutic Communication TechniquesReginette Pisalbo Chan100% (1)
- Assesment of NewbornDocumento74 pagineAssesment of NewbornRaghu RajanNessuna valutazione finora
- TractionDocumento79 pagineTractionKoRnflakes100% (9)
- Clinical Teaching Plan FormatDocumento12 pagineClinical Teaching Plan FormatEmerald ArcenaNessuna valutazione finora
- Anus, Rectum, and Prostate AssessmentDocumento24 pagineAnus, Rectum, and Prostate AssessmentLyn Mende100% (1)
- Steps For Donning Doffing PPEDocumento2 pagineSteps For Donning Doffing PPEAlfhathinNessuna valutazione finora
- Physical AssessmentDocumento24 paginePhysical Assessmentmayla_jordan3666Nessuna valutazione finora
- 2020thoraxlungs Neckheart VesselsDocumento171 pagine2020thoraxlungs Neckheart VesselsFaith madayagNessuna valutazione finora
- Assessing Breasts and AxillaeDocumento32 pagineAssessing Breasts and AxillaeBai-Rhema Marmay100% (1)
- Eyes AssessmentDocumento23 pagineEyes AssessmentAra AlibasaNessuna valutazione finora
- Skin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxDocumento92 pagineSkin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxAT4-11 HUMSS 2 CEDRICK ILAO100% (1)
- Test CN I (Olfactory)Documento3 pagineTest CN I (Olfactory)frechel kimNessuna valutazione finora
- Head To Toe AssessmentDocumento56 pagineHead To Toe AssessmentmisshieNessuna valutazione finora
- Capillary Blood Glucose TestingDocumento4 pagineCapillary Blood Glucose TestingJUVIELY PREMACIONessuna valutazione finora
- Peri CareDocumento13 paginePeri Careguy2dieforNessuna valutazione finora
- Physical AssessmentDocumento90 paginePhysical AssessmentReann LeeNessuna valutazione finora
- Partial Head To Toe Assess TranscriptDocumento9 paginePartial Head To Toe Assess TranscriptgraceNessuna valutazione finora
- Skin, Hair, and Nails AssessmentDocumento44 pagineSkin, Hair, and Nails Assessmentعمر حليم omar haleem100% (1)
- Cataract-Case Study - ADOMPINGDocumento8 pagineCataract-Case Study - ADOMPINGboogeyman6dimakutaNessuna valutazione finora
- Physical Assessment (Normal Findings)Documento31 paginePhysical Assessment (Normal Findings)Rinki SinghNessuna valutazione finora
- Assessment of The Integumentary SystemDocumento21 pagineAssessment of The Integumentary SystemSheila Mae Panis100% (1)
- Wesleyan University-Philippines: Performance Evaluation Tool NCM 101 - Health Assessment DirectionsDocumento5 pagineWesleyan University-Philippines: Performance Evaluation Tool NCM 101 - Health Assessment DirectionsLauren CarlosIINessuna valutazione finora
- Review of Systems For Current Health Problems (Health Assessment)Documento5 pagineReview of Systems For Current Health Problems (Health Assessment)younggirldavid100% (1)
- Assessment of The EyesDocumento9 pagineAssessment of The Eyesmarkkkkkkkheeess100% (3)
- Colostomy CareDocumento15 pagineColostomy CareMahmoud Sherif100% (1)
- Health Assessment Complete 2Documento14 pagineHealth Assessment Complete 2kimberly100% (1)
- Administering Oral MedicationsDocumento5 pagineAdministering Oral MedicationsAda Gay Olandia SerencioNessuna valutazione finora
- Assessing Heart and Central VesselsDocumento34 pagineAssessing Heart and Central VesselsGemmalene Pacleb100% (1)
- Behavior and Mental StatusDocumento41 pagineBehavior and Mental StatusGokul Poudel100% (1)
- PTERYGIUMDocumento33 paginePTERYGIUMdiana0% (1)
- Assessing Breast and AxillaeDocumento23 pagineAssessing Breast and AxillaeGemmalene PaclebNessuna valutazione finora
- Assessing AbdomenDocumento33 pagineAssessing Abdomenjaypee01Nessuna valutazione finora
- Assessing Appearance and Mental StatusDocumento12 pagineAssessing Appearance and Mental StatusAaron Perez SubidaNessuna valutazione finora
- Eye, Ear, Nose and Throat Assessment and Disorders Final PPT, NursingDocumento489 pagineEye, Ear, Nose and Throat Assessment and Disorders Final PPT, NursingFirifan Diriba100% (1)
- Eye and Ear Assessment and DisordersDocumento374 pagineEye and Ear Assessment and DisordersFirifan DiribaNessuna valutazione finora
- Cranial Nerve Examination OSCE GuideDocumento26 pagineCranial Nerve Examination OSCE GuideAbdullah Basheer AL-AnaziNessuna valutazione finora
- October 2017 Ophthalmic PearlsDocumento3 pagineOctober 2017 Ophthalmic PearlsShafa KhansaNessuna valutazione finora
- Red Eye With Normal VisionDocumento58 pagineRed Eye With Normal VisionDiskaAstariniNessuna valutazione finora
- Sense Organ Ear Eye and Skin NoteDocumento29 pagineSense Organ Ear Eye and Skin NoteAnkit SubediNessuna valutazione finora
- Eye Pathology: Dr. Jusuf FantoniDocumento8 pagineEye Pathology: Dr. Jusuf Fantonitutor tujuhNessuna valutazione finora
- Dr. Sadiqa Stelzner, M.D., FACS Is Honored by The Top 100 Registry As A Top 100 Doctor in The Field of OphthalmologyDocumento3 pagineDr. Sadiqa Stelzner, M.D., FACS Is Honored by The Top 100 Registry As A Top 100 Doctor in The Field of OphthalmologyPR.comNessuna valutazione finora
- Vision-SanDiego (1) - 231013 - 141100Documento10 pagineVision-SanDiego (1) - 231013 - 141100fernyz2886Nessuna valutazione finora
- Blepharoplasty ComplicationsDocumento12 pagineBlepharoplasty ComplicationsMaría Alejandra Rojas MontenegroNessuna valutazione finora
- Pediatric Ophthamology 2005Documento835 paginePediatric Ophthamology 2005Jomar100% (1)
- Image Formation and Detection: Earlier in Lesson 6Documento2 pagineImage Formation and Detection: Earlier in Lesson 6leonNessuna valutazione finora
- Eye Med SummaryDocumento2 pagineEye Med SummaryparthaNessuna valutazione finora
- The Ocular Trauma Score: Robert ScottDocumento2 pagineThe Ocular Trauma Score: Robert ScottBruno ZanchettaNessuna valutazione finora
- Ocular Penetrans Trauma and It EditDocumento11 pagineOcular Penetrans Trauma and It EditTamsilNessuna valutazione finora
- اخطاء انكسار 6Documento2 pagineاخطاء انكسار 6Hassan AljaberiNessuna valutazione finora
- Amity International School, Noida CH. 10. The Human Eye and The Colorful World RESOURCE SHEET: 1Documento3 pagineAmity International School, Noida CH. 10. The Human Eye and The Colorful World RESOURCE SHEET: 1dreAdNessuna valutazione finora
- 14.kuliah-Histologi MataDocumento35 pagine14.kuliah-Histologi MataRahmat NugrohoNessuna valutazione finora
- Lippincott's Illustrated ReviewsDocumento1 paginaLippincott's Illustrated Reviewsrahma pandaNessuna valutazione finora
- Fundus Autofluorescence and Optical Coherence TomoDocumento4 pagineFundus Autofluorescence and Optical Coherence TomoAndi Tiara S. AdamNessuna valutazione finora
- Toùm Taét: Muïc ÑíchDocumento17 pagineToùm Taét: Muïc ÑíchBS Hong HaNessuna valutazione finora
- Vision Therapy PDFDocumento72 pagineVision Therapy PDF4nsan4o4luNessuna valutazione finora
- Eye Exercise FAQDocumento59 pagineEye Exercise FAQCaroline BrandtNessuna valutazione finora
- Glaucoma NotesDocumento39 pagineGlaucoma NotesMuhammad SabirNessuna valutazione finora
- Jurnal Penelitian DR EkoDocumento1 paginaJurnal Penelitian DR EkoEko WidayantoNessuna valutazione finora
- Edst 6216 Annotated BibliographyDocumento9 pagineEdst 6216 Annotated Bibliographyapi-365942457Nessuna valutazione finora
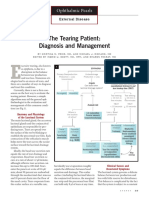
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocumento3 pagineThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9Nessuna valutazione finora
- What Are Causes of BlindnessDocumento20 pagineWhat Are Causes of BlindnesssohaibNessuna valutazione finora
- Optical DispensingDocumento10 pagineOptical DispensingAwais A.Nessuna valutazione finora