Potrebbero piacerti anche
- Cardio InternetDocumento46 pagineCardio InternetnaimNessuna valutazione finora
- Bleeding During Pregnancy and Nursing Care PlanDocumento17 pagineBleeding During Pregnancy and Nursing Care PlanLizcelle Bihasa86% (7)
- Anatomy and Physiology of The Female Reproductive SystemDocumento34 pagineAnatomy and Physiology of The Female Reproductive Systemruthpebbles100% (2)
- Bleeding in Early PregnancyDocumento4 pagineBleeding in Early Pregnancynur1146Nessuna valutazione finora
- HDP Best 1Documento137 pagineHDP Best 1Fedlu SirajNessuna valutazione finora
- Hypertensive Disorders of PregnancyDocumento70 pagineHypertensive Disorders of PregnancyYibelu BazezewNessuna valutazione finora
- Esophageal Atresia: Name of The Disease Description ManagementDocumento4 pagineEsophageal Atresia: Name of The Disease Description ManagementAle SandraNessuna valutazione finora
- UTI in PregnancyDocumento33 pagineUTI in Pregnancyyusufkiduchu8Nessuna valutazione finora
- Ids Trans and SamplexDocumento93 pagineIds Trans and SamplexPrincess Cate MercadoNessuna valutazione finora
- Hyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDocumento49 pagineHyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDonna LabaniegoNessuna valutazione finora
- Pre EclampsiaDocumento6 paginePre EclampsiaDannyca Kyle BahallaNessuna valutazione finora
- CTG Finding S-GuidelinesDocumento15 pagineCTG Finding S-GuidelinesAyman AlmugaddamiNessuna valutazione finora
- GDIABETUS MELITUS EyobDocumento60 pagineGDIABETUS MELITUS Eyobm.pfortress.ojNessuna valutazione finora
- Nature of IPV, Tjaden and Thoennes, 2000Documento62 pagineNature of IPV, Tjaden and Thoennes, 2000spespNessuna valutazione finora
- Anaemia in PregnancyDocumento15 pagineAnaemia in PregnancyNorshahidah Ieda100% (1)
- Gestational Hypertension: Maternal Health Care-ClinicalDocumento10 pagineGestational Hypertension: Maternal Health Care-ClinicalIbrahim W. HassanNessuna valutazione finora
- Management of Asthma in PregnancyDocumento59 pagineManagement of Asthma in PregnancyakokpanasNessuna valutazione finora
- Anaemia in Pregnancy: by Mr. M. Mwansa RN, RNM, Bsc-NrsDocumento51 pagineAnaemia in Pregnancy: by Mr. M. Mwansa RN, RNM, Bsc-NrsMelody ChilunguNessuna valutazione finora
- AntepartumDocumento128 pagineAntepartumIris Caberte100% (1)
- Anemia in PregnancyDocumento34 pagineAnemia in PregnancyHannah Halim100% (1)
- Notes-Introduction To Research MethodologyDocumento165 pagineNotes-Introduction To Research Methodologymacklinaprotas01Nessuna valutazione finora
- Necrotizing Enterocolitis - 2019Documento10 pagineNecrotizing Enterocolitis - 2019Mischief ManagerNessuna valutazione finora
- Intestinal AtresiaDocumento16 pagineIntestinal AtresiaMalueth AnguiNessuna valutazione finora
- Neonatal Jaundice Cme 3Documento56 pagineNeonatal Jaundice Cme 3Arief NorddinNessuna valutazione finora
- M&D OutlineDocumento6 pagineM&D Outlineyared100% (1)
- Pediatrics NotesDocumento72 paginePediatrics NotesSHEENA MAE DE LOS REYESNessuna valutazione finora
- Hypertension PregnancyDocumento45 pagineHypertension PregnancyMohammed IbraheemNessuna valutazione finora
- Final Exam NotesDocumento24 pagineFinal Exam NotesNicholeGarcesCisnerosNessuna valutazione finora
- OB Chapter 5Documento56 pagineOB Chapter 5Bini JaminNessuna valutazione finora
- 1-Cardiac Disease With PregnancyDocumento46 pagine1-Cardiac Disease With PregnancyDrMohammad KhadrawyNessuna valutazione finora
- Lec#10Documento30 pagineLec#10hani bilalNessuna valutazione finora
- High Risk Antepartum Nursing Care 4Documento51 pagineHigh Risk Antepartum Nursing Care 4Wendy EvansNessuna valutazione finora
- Evidence Based Practice ProcessDocumento29 pagineEvidence Based Practice ProcessDrmirfat AlkashifNessuna valutazione finora
- Hypertension Disorder in PregnancyDocumento42 pagineHypertension Disorder in Pregnancyholly girlchy JastinNessuna valutazione finora
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDocumento9 pagineAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongNessuna valutazione finora
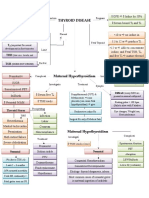
- Thyroid DiseaseDocumento1 paginaThyroid DiseaseZiyadNessuna valutazione finora
- Pedia HandoutsDocumento40 paginePedia HandoutsMarius Clifford BilledoNessuna valutazione finora
- Child Diseases SGA and LGADocumento30 pagineChild Diseases SGA and LGACrapster GamingNessuna valutazione finora
- Cardiac Disease in PregnancyDocumento86 pagineCardiac Disease in PregnancyAustine OdhiamboNessuna valutazione finora
- Obstetics Simplified El-MowafiDocumento515 pagineObstetics Simplified El-Mowafiapi-370504650% (2)
- Concept MapDocumento4 pagineConcept MapDud AccNessuna valutazione finora
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocumento10 pagine(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanNessuna valutazione finora
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocumento3 pagineHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Pediatrics Modern Day AnalysisDocumento144 paginePediatrics Modern Day AnalysisDaniyal AzmatNessuna valutazione finora
- PIHDocumento4 paginePIHAngelica Floreza DullasNessuna valutazione finora
- Fetal Skull &pelvis NewDocumento80 pagineFetal Skull &pelvis NewsameerNessuna valutazione finora
- Autoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsDocumento47 pagineAutoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsGalih Putra RanggaNessuna valutazione finora
- Female PathologyDocumento16 pagineFemale Pathologymiguel cuevasNessuna valutazione finora
- Lecture 01 - CVSDocumento45 pagineLecture 01 - CVSHeeb WardaNessuna valutazione finora
- Cardiac Disease in PregnancyDocumento44 pagineCardiac Disease in PregnancyNariska Cooper100% (1)
- AnaemiaDocumento71 pagineAnaemiaREETHUNessuna valutazione finora
- Asthma and Rhinitis During PregnancyDocumento175 pagineAsthma and Rhinitis During PregnancyAndika Wima PratamaNessuna valutazione finora
- Handout Nrg203 (LD)Documento31 pagineHandout Nrg203 (LD)Kyle DoloritosNessuna valutazione finora
- Esophageal AtresiaDocumento4 pagineEsophageal Atresiafidc_0428Nessuna valutazione finora
- Necrotizing EnterocolitisDocumento36 pagineNecrotizing EnterocolitisMahad Maxamed AxmedNessuna valutazione finora
- Heart FailureDocumento1 paginaHeart FailureTrisha VergaraNessuna valutazione finora
- Breech Presentation-Pritiss Nair Group 2Documento45 pagineBreech Presentation-Pritiss Nair Group 2asmeralda99Nessuna valutazione finora
- OB Hematologic DiseasesDocumento2 pagineOB Hematologic DiseasespreciousjemNessuna valutazione finora
- Antepartum HaemorrhageDocumento33 pagineAntepartum HaemorrhageMedy WedhanggaNessuna valutazione finora
- Antepartum HemorrhageDocumento43 pagineAntepartum HemorrhageFedlu SirajNessuna valutazione finora
- 3 OB 3 - Obstetrical Hemorrhage PDFDocumento14 pagine3 OB 3 - Obstetrical Hemorrhage PDFIrene FranzNessuna valutazione finora
- Bleeding in Late PregnancyDocumento20 pagineBleeding in Late Pregnancyعبدالحكيم عمر عامر بن الزوعNessuna valutazione finora
- Maternity MOH 333 PDFDocumento4 pagineMaternity MOH 333 PDFMajivaNessuna valutazione finora
- Male Reproductive System and Female Reproductive SystemDocumento2 pagineMale Reproductive System and Female Reproductive SystemChristian Ezekiel LagmayNessuna valutazione finora
- Management of Breech Presentation: Green-Top Guideline No. 20bDocumento27 pagineManagement of Breech Presentation: Green-Top Guideline No. 20bSastra WijayaNessuna valutazione finora
- Gyne Past Papers Update 5Documento139 pagineGyne Past Papers Update 5Misbah KaleemNessuna valutazione finora
- Obstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONDocumento59 pagineObstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONmaezu100% (2)
- Primigravida Mothers Knowledge andDocumento10 paginePrimigravida Mothers Knowledge andJamby VivasNessuna valutazione finora
- Medical Narrative Report On Child DeliveryDocumento3 pagineMedical Narrative Report On Child DeliveryMelona BenidoNessuna valutazione finora
- DLP - Menstrual CycleDocumento5 pagineDLP - Menstrual CycleRigel Del CastilloNessuna valutazione finora
- SP BRDocumento10 pagineSP BRElinor Christy BaggaoNessuna valutazione finora
- Preterm Premature Rupture of Membranes (PPROM) : Why Focus On PPROM?Documento4 paginePreterm Premature Rupture of Membranes (PPROM) : Why Focus On PPROM?sasoyNessuna valutazione finora
- Lecture 1 Family PlanningDocumento84 pagineLecture 1 Family PlanningAlfie Adam Ramillano100% (4)
- College of Our Lady of Mt. Carmel: Midwifery DepartmentDocumento10 pagineCollege of Our Lady of Mt. Carmel: Midwifery DepartmentMA. JYRELL BONITONessuna valutazione finora
- Uterine ProlapseDocumento6 pagineUterine ProlapseIndah Rizki Haksapani Nasution100% (1)
- Prevention of Maternal To Child Transmission of Hiv-Recent AdvancesDocumento41 paginePrevention of Maternal To Child Transmission of Hiv-Recent AdvancesSumit LakhanpalNessuna valutazione finora
- Morbidly Adherent PlacentaDocumento5 pagineMorbidly Adherent PlacentaDara Mayang SariNessuna valutazione finora
- Oral Contraceptive InstructionsDocumento2 pagineOral Contraceptive Instructionsmiracle jefferyNessuna valutazione finora
- Group E ACTIVITY PROPOSALDocumento19 pagineGroup E ACTIVITY PROPOSALCommunity BNessuna valutazione finora
- Ob-Gyne: Obstetric History and PEDocumento6 pagineOb-Gyne: Obstetric History and PEPorori BookshopNessuna valutazione finora
- Maternal and Child ReviewerDocumento330 pagineMaternal and Child ReviewerMiles Brianne Lymer A. OlvidoNessuna valutazione finora
- C 16Documento15 pagineC 16Nichole LopezNessuna valutazione finora
- Form 1Documento5 pagineForm 1Fuiyee YapNessuna valutazione finora
- Maternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewDocumento23 pagineMaternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewasfwegereNessuna valutazione finora
- Upaya Pemenuhan Kebutuhan Istirahat Tidur Pada Ibu Postpartum Dengan PreeklampsiaDocumento12 pagineUpaya Pemenuhan Kebutuhan Istirahat Tidur Pada Ibu Postpartum Dengan PreeklampsiaAwi PomouNessuna valutazione finora
- 07 - Partograph - GLG20140212Documento50 pagine07 - Partograph - GLG20140212Geline Joy D. SamillanoNessuna valutazione finora
- Week 24 Abnormal Uterine BleedingDocumento6 pagineWeek 24 Abnormal Uterine BleedingGhazal KangoNessuna valutazione finora
- Sectio Caesarea (SC) Dengan Tingkat Kemandirian Pasien DiDocumento7 pagineSectio Caesarea (SC) Dengan Tingkat Kemandirian Pasien DiNurulNessuna valutazione finora
- Instruments in Obstetrics and Gynecology.Documento60 pagineInstruments in Obstetrics and Gynecology.Saurabh Gautam100% (2)
- Anatomy and PhysiologyDocumento3 pagineAnatomy and PhysiologyJade AltarejosNessuna valutazione finora