Potrebbero piacerti anche
- 3 Ae 6 B 4 F 68Documento7 pagine3 Ae 6 B 4 F 68MohammadAhmadNessuna valutazione finora
- Regn. No.: The Employees' Deposit Linked Insurance Scheme 1976Documento2 pagineRegn. No.: The Employees' Deposit Linked Insurance Scheme 1976Tilak RajNessuna valutazione finora
- Constitution of the State of Minnesota — 1876 VersionDa EverandConstitution of the State of Minnesota — 1876 VersionNessuna valutazione finora
- Gloria Allred Victim of Confessed Rape Faces Jail After Attorneys Steal Civil SettlementDocumento7 pagineGloria Allred Victim of Confessed Rape Faces Jail After Attorneys Steal Civil SettlementDeanna WilliamsNessuna valutazione finora
- Petition for Certiorari – Patent Case 01-438 - Federal Rule of Civil Procedure 52(a)Da EverandPetition for Certiorari – Patent Case 01-438 - Federal Rule of Civil Procedure 52(a)Nessuna valutazione finora
- NOTICE OF FILING EXHIBITS FOR 12/22/2020 HEARING S. Schneider BK 11 20-22398Documento18 pagineNOTICE OF FILING EXHIBITS FOR 12/22/2020 HEARING S. Schneider BK 11 20-22398larry-612445Nessuna valutazione finora
- Get a Second Opinion before You Sign: What to do when the Bank says 'No' ? How to survive and thrive with Private Lending.Da EverandGet a Second Opinion before You Sign: What to do when the Bank says 'No' ? How to survive and thrive with Private Lending.Nessuna valutazione finora
- Maxims of LawDocumento22 pagineMaxims of LawtdhouckNessuna valutazione finora
- Constitution of the State of Minnesota — Republican VersionDa EverandConstitution of the State of Minnesota — Republican VersionNessuna valutazione finora
- United States Bankruptcy Court: Southern District of West VirginiaDocumento54 pagineUnited States Bankruptcy Court: Southern District of West VirginiaWVGOP Research100% (1)
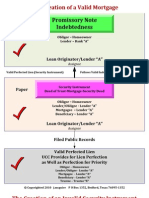
- Creation of FraudDocumento11 pagineCreation of FraudA. Campbell100% (1)
- Order Dismissing Civ. 21-00392, Gary Dubin v. Office of The Disciplinary Counsel, Et Al.Documento11 pagineOrder Dismissing Civ. 21-00392, Gary Dubin v. Office of The Disciplinary Counsel, Et Al.Ian LindNessuna valutazione finora
- SummonsDocumento4 pagineSummonsFranchise AlienNessuna valutazione finora
- KingCast Mortgage Movies Michael Dean Levitz v. MERS and Capital One Preliminary Injunction CH 11 Adversary 18-01000-CMA-13Documento14 pagineKingCast Mortgage Movies Michael Dean Levitz v. MERS and Capital One Preliminary Injunction CH 11 Adversary 18-01000-CMA-13Christopher KingNessuna valutazione finora
- United States Court of Appeals, Tenth CircuitDocumento10 pagineUnited States Court of Appeals, Tenth CircuitScribd Government DocsNessuna valutazione finora
- Plea Agreement, U.S. vs. Baoke ZhangDocumento19 paginePlea Agreement, U.S. vs. Baoke ZhangGeekWireNessuna valutazione finora
- ROWLAND Et Al v. OCWEN LOAN SERVICING, LLC. Et Al Notice of RemovalDocumento6 pagineROWLAND Et Al v. OCWEN LOAN SERVICING, LLC. Et Al Notice of RemovalACELitigationWatchNessuna valutazione finora
- The Succession Act, 1925Documento6 pagineThe Succession Act, 1925Atif RehmanNessuna valutazione finora
- Bank of The United States v. United States, 43 U.S. 711 (1844)Documento33 pagineBank of The United States v. United States, 43 U.S. 711 (1844)Scribd Government DocsNessuna valutazione finora
- N1 Claim Form Against Swansea UniversityDocumento2 pagineN1 Claim Form Against Swansea UniversityJonathan BishopNessuna valutazione finora
- USPS OIG Management Advisory - Benchmarking Mail Distribution To CarriersDocumento15 pagineUSPS OIG Management Advisory - Benchmarking Mail Distribution To CarriersbsheehanNessuna valutazione finora
- Snap Securities Proposed SettlementDocumento32 pagineSnap Securities Proposed SettlementTHROnlineNessuna valutazione finora
- United States District Court Eastern District of New YorkDocumento4 pagineUnited States District Court Eastern District of New YorkLaw&CrimeNessuna valutazione finora
- Act For The Relief of Sick & DisabledSeamen, July 1798Documento2 pagineAct For The Relief of Sick & DisabledSeamen, July 1798Zach VaughnNessuna valutazione finora
- Capital One, National Association vs. Jacob FrydmanDocumento20 pagineCapital One, National Association vs. Jacob FrydmanJay100% (1)
- 150813bock AmicusbriefDocumento46 pagine150813bock AmicusbriefSamuelNessuna valutazione finora
- AlaAL ZAALIG2011Documento5 pagineAlaAL ZAALIG2011Ala AlzaaligNessuna valutazione finora
- IRS Draft Form 8960Documento2 pagineIRS Draft Form 8960forbesadminNessuna valutazione finora
- Application For Order To Administer Property (Form-Pppr-6)Documento6 pagineApplication For Order To Administer Property (Form-Pppr-6)Benne JamesNessuna valutazione finora
- Affidavit For Criminal Complaint Against Bank of America-8pgsDocumento8 pagineAffidavit For Criminal Complaint Against Bank of America-8pgsJOSHUA TASKNessuna valutazione finora
- For Correspondence To Bob: For Subscription and Renewal Technical Support, Log in Problems, Etc.Documento40 pagineFor Correspondence To Bob: For Subscription and Renewal Technical Support, Log in Problems, Etc.freedom_lover_k0% (1)
- Blue Badge Discount Registration FormDocumento11 pagineBlue Badge Discount Registration FormtrapstarrNessuna valutazione finora
- U S B C: Nited Tates Ankruptcy OurtDocumento4 pagineU S B C: Nited Tates Ankruptcy OurtChapter 11 DocketsNessuna valutazione finora
- Lehman Brothers - Disclosure Statement To Second Amended Joint Chapter 11, Dated June 30, 2011Documento530 pagineLehman Brothers - Disclosure Statement To Second Amended Joint Chapter 11, Dated June 30, 2011bk917Nessuna valutazione finora
- 5 - 23!5!26 California Finance Lenders LawDocumento5 pagine5 - 23!5!26 California Finance Lenders Lawkeith2438Nessuna valutazione finora
- Treasury Secretary Steve Mnuchin Asks Congress To Raise Debt LimitDocumento1 paginaTreasury Secretary Steve Mnuchin Asks Congress To Raise Debt LimitCNBC.comNessuna valutazione finora
- Agency Name: Version: (N) Date: (Mm/dd/yyyy)Documento2 pagineAgency Name: Version: (N) Date: (Mm/dd/yyyy)techcert100% (1)
- Certificate of Payment of Foreign Death Tax: For Paperwork Reduction Act Notice, See The Back of This FormDocumento2 pagineCertificate of Payment of Foreign Death Tax: For Paperwork Reduction Act Notice, See The Back of This FormFrancis Wolfgang UrbanNessuna valutazione finora
- Case 2:21-cv-00732-LA Filed 06/15/21 Page 1 of 30 Document 1Documento30 pagineCase 2:21-cv-00732-LA Filed 06/15/21 Page 1 of 30 Document 1TMJ4 NewsNessuna valutazione finora
- Texas Court of Criminal Appeals Mandamus by Paxton Special Prosecutors June 2017Documento160 pagineTexas Court of Criminal Appeals Mandamus by Paxton Special Prosecutors June 2017lanashadwick100% (1)
- Employment Regulations 1980 (Amended As at 2006)Documento43 pagineEmployment Regulations 1980 (Amended As at 2006)Nelo BuensalidaNessuna valutazione finora
- U S B C: Nited Tates Ankruptcy OurtDocumento4 pagineU S B C: Nited Tates Ankruptcy OurtChapter 11 DocketsNessuna valutazione finora
- The New Direct Tax Code (DTC)Documento18 pagineThe New Direct Tax Code (DTC)aggarwalajay2Nessuna valutazione finora
- C. Pulsifer: 10 Thu 11: 50 Am Family Law FAX 760 863 8707Documento48 pagineC. Pulsifer: 10 Thu 11: 50 Am Family Law FAX 760 863 8707richk7Nessuna valutazione finora
- 77 - Gov - Uscourts.ord.124749.77.0Documento4 pagine77 - Gov - Uscourts.ord.124749.77.0Freeman Lawyer100% (1)
- Leyah Yisrael Ucc Financing StatementDocumento35 pagineLeyah Yisrael Ucc Financing StatementLeyah YisraelNessuna valutazione finora
- Gresh v. MPayMe Partners - Complaint PDFDocumento32 pagineGresh v. MPayMe Partners - Complaint PDFMark JaffeNessuna valutazione finora
- PRINT in BLACK INK. Ovals Must Be Filled in Completely.Documento2 paginePRINT in BLACK INK. Ovals Must Be Filled in Completely.mik2bgNessuna valutazione finora
- Study Material For This LectureDocumento12 pagineStudy Material For This Lectureosaie100% (1)
- Tax Exempt PDFDocumento2 pagineTax Exempt PDFLj Perrier100% (1)
- Discharge of Debtor - Fleury Chapter 7 BankruptcyDocumento2 pagineDischarge of Debtor - Fleury Chapter 7 Bankruptcyarsmith718100% (1)
- 2010 08 13 Legal Issues - Register of Deeds - FinalDocumento71 pagine2010 08 13 Legal Issues - Register of Deeds - FinalgregmanuelNessuna valutazione finora
- Estate of Ernst N. Petschek, Deceased, Thomas H. Petschek and Asher Lans, Executors v. The Commissioner of Internal Revenue, 738 F.2d 67, 2d Cir. (1984)Documento8 pagineEstate of Ernst N. Petschek, Deceased, Thomas H. Petschek and Asher Lans, Executors v. The Commissioner of Internal Revenue, 738 F.2d 67, 2d Cir. (1984)Scribd Government DocsNessuna valutazione finora
- Securities and Exchange Commission (SEC) - Formadv-NrDocumento2 pagineSecurities and Exchange Commission (SEC) - Formadv-NrhighfinanceNessuna valutazione finora
- Senate Hearing, 112TH Congress - Oversight of The Financial Fraud Enforcement Task ForceDocumento53 pagineSenate Hearing, 112TH Congress - Oversight of The Financial Fraud Enforcement Task ForceScribd Government DocsNessuna valutazione finora
- Alito Denial of Emergency RequestDocumento2 pagineAlito Denial of Emergency RequestAmmoLand Shooting Sports NewsNessuna valutazione finora
- CBS and Postal DepartmentDocumento49 pagineCBS and Postal DepartmentK V Sridharan General Secretary P3 NFPENessuna valutazione finora
- SLM Corp: Prospectus Filed Pursuant To Rule 424 (B) (5) Filed On 01/24/2012Documento70 pagineSLM Corp: Prospectus Filed Pursuant To Rule 424 (B) (5) Filed On 01/24/2012avico510100% (1)
- Hand Seals Guide PDFDocumento3 pagineHand Seals Guide PDFCsc Waters100% (1)
- MailingAffidavit Pardon PDFDocumento1 paginaMailingAffidavit Pardon PDFCsc WatersNessuna valutazione finora
- Commutation Application-Pack PDFDocumento6 pagineCommutation Application-Pack PDFCsc WatersNessuna valutazione finora
- Commutation Application-Pack PDFDocumento6 pagineCommutation Application-Pack PDFCsc WatersNessuna valutazione finora
- WWW Naruto2 ComDocumento11 pagineWWW Naruto2 ComCsc WatersNessuna valutazione finora
- WWW Dragoart ComDocumento6 pagineWWW Dragoart ComCsc WatersNessuna valutazione finora
- Until 1: Lab QuestionsDocumento2 pagineUntil 1: Lab Questionsindy schalkNessuna valutazione finora
- Peter Lance Spy PLAYBOYDocumento7 paginePeter Lance Spy PLAYBOYPeter LanceNessuna valutazione finora
- 10 Zamboanga Del Norte Vs CA, G.R. No. 109853. October 11, 2000Documento3 pagine10 Zamboanga Del Norte Vs CA, G.R. No. 109853. October 11, 2000Perry YapNessuna valutazione finora
- People Vs CoderesDocumento1 paginaPeople Vs CoderesclsNessuna valutazione finora
- Eijansantos Vs SPTF 156, GR No. 203696, June 2, 2014 PDFDocumento12 pagineEijansantos Vs SPTF 156, GR No. 203696, June 2, 2014 PDFIya LumbangNessuna valutazione finora
- CRCJ1000B W13 Syllabus VFDocumento6 pagineCRCJ1000B W13 Syllabus VFJose Li ToNessuna valutazione finora
- George Zimmerman LawsuitDocumento36 pagineGeorge Zimmerman LawsuitPeterBurkeNessuna valutazione finora
- 2 - Valera v. Tuason, JR., GR No. L-1276, 30 April 1948Documento7 pagine2 - Valera v. Tuason, JR., GR No. L-1276, 30 April 1948Jian CerreroNessuna valutazione finora
- R. v. Gadam, (2016) O.J. No. 4316Documento10 pagineR. v. Gadam, (2016) O.J. No. 4316Jordan WeiszNessuna valutazione finora
- Torrevillas Vs Judge NavidadDocumento2 pagineTorrevillas Vs Judge NavidadAngela De LeonNessuna valutazione finora
- Attorney Will Claiborne Abusive Litigation LetterDocumento23 pagineAttorney Will Claiborne Abusive Litigation Lettersavannahnow.com100% (1)
- Bs Lesson GovernmentDocumento5 pagineBs Lesson GovernmentKy HydeNessuna valutazione finora
- Lynching in America: A Tool of RacismDocumento3 pagineLynching in America: A Tool of Racismtjfeeny100% (2)
- 20th Century Fox Film Corporation V CADocumento2 pagine20th Century Fox Film Corporation V CAKrys Martinez100% (1)
- People Vs Manes & (Palonte Vs SavellanoDocumento3 paginePeople Vs Manes & (Palonte Vs SavellanoCel DelabahanNessuna valutazione finora
- The Ocas Report and RecommendationDocumento3 pagineThe Ocas Report and RecommendationcyhaaangelaaaNessuna valutazione finora
- State Ex Rel. Stoyanoff v. Berkeley 458 S.W.2d 305 (1970)Documento1 paginaState Ex Rel. Stoyanoff v. Berkeley 458 S.W.2d 305 (1970)Nicole IbayNessuna valutazione finora
- Maximilien RobespierreDocumento26 pagineMaximilien RobespierreValpo ValparaisoNessuna valutazione finora
- SAMPLE Exam Evidence NEW 2019 PDFDocumento19 pagineSAMPLE Exam Evidence NEW 2019 PDFS.k.raghavNessuna valutazione finora
- Personal Reviewer - 7610Documento6 paginePersonal Reviewer - 7610Sarah CruzNessuna valutazione finora
- Demonological TheoryDocumento2 pagineDemonological TheoryBhenjo Hernandez BaronaNessuna valutazione finora
- Rule 126 Search and Seizure Report Group 7Documento36 pagineRule 126 Search and Seizure Report Group 7Ronnie MagsinoNessuna valutazione finora
- RA 9262 Anti Violence Against Woment andDocumento35 pagineRA 9262 Anti Violence Against Woment andAtty Xe CastleNessuna valutazione finora
- USDC - DKT 25 - Errata - Filed by Calif Supreme CT in Support of Motion To DismissDocumento3 pagineUSDC - DKT 25 - Errata - Filed by Calif Supreme CT in Support of Motion To DismissHonor in JusticeNessuna valutazione finora
- The Saga of Satyendra Dubey. Case I/PveDocumento3 pagineThe Saga of Satyendra Dubey. Case I/PveCrazily RightNessuna valutazione finora
- Group Pink: Unlawful Assembly: No. Name Student IdDocumento16 pagineGroup Pink: Unlawful Assembly: No. Name Student IdInaz IdNessuna valutazione finora
- United States v. Hitson Simon A/K/A "Sacko", 995 F.2d 1236, 3rd Cir. (1993)Documento17 pagineUnited States v. Hitson Simon A/K/A "Sacko", 995 F.2d 1236, 3rd Cir. (1993)Scribd Government DocsNessuna valutazione finora
- People v. HernandezDocumento1 paginaPeople v. HernandezAiress Canoy Casimero100% (1)
- Perth Amboy OPRA FormDocumento2 paginePerth Amboy OPRA FormThe Citizens CampaignNessuna valutazione finora
- Central Investigation & Security Services LTDDocumento2 pagineCentral Investigation & Security Services LTDPradeep PanigrahiNessuna valutazione finora
- Broken: The most shocking childhood story ever told. An inspirational author who survived it.Da EverandBroken: The most shocking childhood story ever told. An inspirational author who survived it.Valutazione: 5 su 5 stelle5/5 (45)
- Hell Put to Shame: The 1921 Murder Farm Massacre and the Horror of America's Second SlaveryDa EverandHell Put to Shame: The 1921 Murder Farm Massacre and the Horror of America's Second SlaveryValutazione: 2.5 su 5 stelle2.5/5 (3)
- The Bigamist: The True Story of a Husband's Ultimate BetrayalDa EverandThe Bigamist: The True Story of a Husband's Ultimate BetrayalValutazione: 4.5 su 5 stelle4.5/5 (104)
- The Girls Are Gone: The True Story of Two Sisters Who Vanished, the Father Who Kept Searching, and the Adults Who Conspired to Keep the Truth HiddenDa EverandThe Girls Are Gone: The True Story of Two Sisters Who Vanished, the Father Who Kept Searching, and the Adults Who Conspired to Keep the Truth HiddenValutazione: 3.5 su 5 stelle3.5/5 (36)
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansDa EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansValutazione: 4 su 5 stelle4/5 (17)
- If You Tell: A True Story of Murder, Family Secrets, and the Unbreakable Bond of SisterhoodDa EverandIf You Tell: A True Story of Murder, Family Secrets, and the Unbreakable Bond of SisterhoodValutazione: 4.5 su 5 stelle4.5/5 (1800)
- Tinseltown: Murder, Morphine, and Madness at the Dawn of HollywoodDa EverandTinseltown: Murder, Morphine, and Madness at the Dawn of HollywoodNessuna valutazione finora
- Restless Souls: The Sharon Tate Family's Account of Stardom, the Manson Murders, and a Crusade for JusticeDa EverandRestless Souls: The Sharon Tate Family's Account of Stardom, the Manson Murders, and a Crusade for JusticeNessuna valutazione finora
- Perfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthDa EverandPerfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthValutazione: 3.5 su 5 stelle3.5/5 (68)
- Nicole Brown Simpson: The Private Diary of a Life InterruptedDa EverandNicole Brown Simpson: The Private Diary of a Life InterruptedValutazione: 3.5 su 5 stelle3.5/5 (16)
- What the Dead Know: Learning About Life as a New York City Death InvestigatorDa EverandWhat the Dead Know: Learning About Life as a New York City Death InvestigatorValutazione: 4.5 su 5 stelle4.5/5 (70)
- Bind, Torture, Kill: The Inside Story of BTK, the Serial Killer Next DoorDa EverandBind, Torture, Kill: The Inside Story of BTK, the Serial Killer Next DoorValutazione: 3.5 su 5 stelle3.5/5 (77)
- The Gardner Heist: The True Story of the World's Largest Unsolved Art TheftDa EverandThe Gardner Heist: The True Story of the World's Largest Unsolved Art TheftNessuna valutazione finora
- Bloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyDa EverandBloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyValutazione: 4 su 5 stelle4/5 (8)
- Double Lives: True Tales of the Criminals Next DoorDa EverandDouble Lives: True Tales of the Criminals Next DoorValutazione: 4 su 5 stelle4/5 (34)
- Witness: For the Prosecution of Scott PetersonDa EverandWitness: For the Prosecution of Scott PetersonValutazione: 3 su 5 stelle3/5 (44)
- Altamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayDa EverandAltamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayValutazione: 4 su 5 stelle4/5 (25)
- Diamond Doris: The True Story of the World's Most Notorious Jewel ThiefDa EverandDiamond Doris: The True Story of the World's Most Notorious Jewel ThiefValutazione: 3.5 su 5 stelle3.5/5 (18)
- For the Thrill of It: Leopold, Loeb, and the Murder That Shocked Jazz Age ChicagoDa EverandFor the Thrill of It: Leopold, Loeb, and the Murder That Shocked Jazz Age ChicagoValutazione: 4 su 5 stelle4/5 (97)
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIDa EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIValutazione: 4 su 5 stelle4/5 (20)
- Perversion of Justice: The Jeffrey Epstein StoryDa EverandPerversion of Justice: The Jeffrey Epstein StoryValutazione: 4.5 su 5 stelle4.5/5 (10)
- Cold-Blooded: A True Story of Love, Lies, Greed, and MurderDa EverandCold-Blooded: A True Story of Love, Lies, Greed, and MurderValutazione: 4 su 5 stelle4/5 (53)
- To the Bridge: A True Story of Motherhood and MurderDa EverandTo the Bridge: A True Story of Motherhood and MurderValutazione: 4 su 5 stelle4/5 (73)
- Blood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyDa EverandBlood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyValutazione: 3 su 5 stelle3/5 (57)
- In the Name of the Children: An FBI Agent's Relentless Pursuit of the Nation's Worst PredatorsDa EverandIn the Name of the Children: An FBI Agent's Relentless Pursuit of the Nation's Worst PredatorsValutazione: 4.5 su 5 stelle4.5/5 (240)