Potrebbero piacerti anche
- Orientation To AnesthesiaDocumento28 pagineOrientation To AnesthesiaDebi SumarliNessuna valutazione finora
- Individual Drug ResponseDocumento21 pagineIndividual Drug ResponseDebi SumarliNessuna valutazione finora
- Bacterial Classification, Structure and FunctionDocumento8 pagineBacterial Classification, Structure and FunctionDebi SumarliNessuna valutazione finora
- Paket Umrah 2015 OkDocumento13 paginePaket Umrah 2015 OkDebi SumarliNessuna valutazione finora
- Pendekatan Differential Diagnosis AsitesDocumento5 paginePendekatan Differential Diagnosis AsitesDebi SumarliNessuna valutazione finora
- Model of Visually Evoked Cortical Potentials: J. Kremláček, M. Kuba, J. HolčíkDocumento10 pagineModel of Visually Evoked Cortical Potentials: J. Kremláček, M. Kuba, J. HolčíkDebi SumarliNessuna valutazione finora
- UnderstandingAnesthesia1 1 2Documento144 pagineUnderstandingAnesthesia1 1 2marina_shawkyNessuna valutazione finora
- Art:10.1007/s00540 012 1411 9Documento6 pagineArt:10.1007/s00540 012 1411 9Debi SumarliNessuna valutazione finora
- IndianJAnaesth55131-1167084 001927Documento5 pagineIndianJAnaesth55131-1167084 001927Debi SumarliNessuna valutazione finora
- Evaluation of Propofol Anesthesia in Morbidly Obese Children and AdolescentsDocumento9 pagineEvaluation of Propofol Anesthesia in Morbidly Obese Children and AdolescentsDebi SumarliNessuna valutazione finora
- IndianJAnaesth57162-8611173 235511Documento4 pagineIndianJAnaesth57162-8611173 235511Debi SumarliNessuna valutazione finora
- Ectopic Pregnancy Treatment & ManagementDocumento12 pagineEctopic Pregnancy Treatment & ManagementDebi SumarliNessuna valutazione finora
- IndianJAnaesth57146-8612955 235529Documento6 pagineIndianJAnaesth57146-8612955 235529Debi SumarliNessuna valutazione finora
- Testing Visual Acuity in Children and Non-Verbal AdultsDocumento13 pagineTesting Visual Acuity in Children and Non-Verbal AdultsDebi SumarliNessuna valutazione finora
- Cervical Cancer Differential DiagnosesDocumento8 pagineCervical Cancer Differential DiagnosesDebi SumarliNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Batiquin v. Court of AppealsDocumento9 pagineBatiquin v. Court of AppealsEnzo PerezNessuna valutazione finora
- Short Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSDocumento29 pagineShort Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSErkoNessuna valutazione finora
- Life History of Dr.J.T. KentDocumento13 pagineLife History of Dr.J.T. KentPrathibha MadikiNessuna valutazione finora
- Katerina P Reilly ResumeDocumento2 pagineKaterina P Reilly Resumeapi-286221742Nessuna valutazione finora
- ASEA Athletics VT StudyDocumento5 pagineASEA Athletics VT Studyalien asterixNessuna valutazione finora
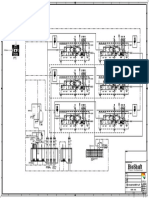
- P&ID - STP-Yanbu SWCC (6units)Documento1 paginaP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiNessuna valutazione finora
- A Nursing Case Study On: Alzheimer's DiseaseDocumento22 pagineA Nursing Case Study On: Alzheimer's DiseaseJesslee Llanes100% (4)
- PolycythemiaDocumento22 paginePolycythemiaIrman DinejadNessuna valutazione finora
- NCP AnxietyDocumento1 paginaNCP AnxietyUnang MagnayeNessuna valutazione finora
- Psychological Approaches To Bipolar Disorders: A Theoretical CritiqueDocumento22 paginePsychological Approaches To Bipolar Disorders: A Theoretical CritiqueGary CadfaelNessuna valutazione finora
- Thyroid Disease OutlineDocumento3 pagineThyroid Disease OutlinePaige BarniniNessuna valutazione finora
- Episiotomy and SuturingDocumento5 pagineEpisiotomy and SuturingAnila SajeshNessuna valutazione finora
- Cyst Theory ClassDocumento310 pagineCyst Theory ClasswakoNessuna valutazione finora
- DPA Fact Sheet Portugal Decriminalization Feb2014Documento3 pagineDPA Fact Sheet Portugal Decriminalization Feb2014webmaster@drugpolicy.orgNessuna valutazione finora
- Decup 2014Documento8 pagineDecup 2014Elija BrockNessuna valutazione finora
- Behavior Therapy Research PaperDocumento8 pagineBehavior Therapy Research PaperAmoni AzziNessuna valutazione finora
- South West Regional Bulletin: A Message From The Director All Change at The CentreDocumento19 pagineSouth West Regional Bulletin: A Message From The Director All Change at The Centre433188Nessuna valutazione finora
- Lecture (2) - Pharmaceutical CareDocumento38 pagineLecture (2) - Pharmaceutical CareRaju NiraulaNessuna valutazione finora
- The Use of Attar (Essential Oils) : Chamomile (Dry & Hot)Documento6 pagineThe Use of Attar (Essential Oils) : Chamomile (Dry & Hot)Ashraf DockratNessuna valutazione finora
- PsychSim 4 Activities Psychopathology and TherapyDocumento6 paginePsychSim 4 Activities Psychopathology and TherapyCarolineNessuna valutazione finora
- Jurnal SkoliosisDocumento9 pagineJurnal SkoliosisLidya SiahaanNessuna valutazione finora
- Stroke StatisticsDocumento13 pagineStroke StatisticsAldo EmeraldNessuna valutazione finora
- Santrock Section 7 Early AdulthoodDocumento12 pagineSantrock Section 7 Early AdulthoodAssumpta Minette Burgos100% (1)
- DR Mahdavi - Mechanical VentilationDocumento28 pagineDR Mahdavi - Mechanical VentilationHimanshu ShrimaliNessuna valutazione finora
- Social Pragmatic Deficits Checklist Sample For Preschool ChildrenDocumento5 pagineSocial Pragmatic Deficits Checklist Sample For Preschool ChildrenBianca GonzalesNessuna valutazione finora
- The Magic of Ilizarov PDFDocumento310 pagineThe Magic of Ilizarov PDFOrto Mesp83% (6)
- Abscess Incision and Drainage NEJMDocumento4 pagineAbscess Incision and Drainage NEJMMarcela CharryNessuna valutazione finora
- Guidelines For Management of Endometrial CarcinomaDocumento41 pagineGuidelines For Management of Endometrial CarcinomaVeenaNessuna valutazione finora
- Foods That Can Purify Blood Naturally - PositiveMedffDocumento7 pagineFoods That Can Purify Blood Naturally - PositiveMedfftmk1989Nessuna valutazione finora
- Greening The Roadmap of The Philippine Pulp and Paper IndustryDocumento14 pagineGreening The Roadmap of The Philippine Pulp and Paper IndustryJade LimbagoNessuna valutazione finora