Potrebbero piacerti anche
- The Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesDa EverandThe Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesValutazione: 1.5 su 5 stelle1.5/5 (3)
- Mrcog Part 1 Recalls 2005-2009Documento227 pagineMrcog Part 1 Recalls 2005-2009sanabinfaizNessuna valutazione finora
- Dewhurst's Textbook of Obstetrics & GynaecologyDa EverandDewhurst's Textbook of Obstetrics & GynaecologyChristoph LeesValutazione: 2 su 5 stelle2/5 (1)
- Septeper 2015 Recall 200 Sba Mrcog Part 1Documento49 pagineSepteper 2015 Recall 200 Sba Mrcog Part 1VINOD GUPTA100% (2)
- MCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookDocumento118 pagineMCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookAhmed Abdelmonsef Albashatly86% (14)
- PROLOG: Obstetrics, Eighth Edition (Assessment & Critique)Da EverandPROLOG: Obstetrics, Eighth Edition (Assessment & Critique)Valutazione: 5 su 5 stelle5/5 (2)
- Mrcog Part1Documento7 pagineMrcog Part1Yogeshwari Pardeshi100% (3)
- Instruction Manual in Obstetrics: Volume OneDa EverandInstruction Manual in Obstetrics: Volume OneNessuna valutazione finora
- Solved Mrcog Past Papers 2005 To 2001Documento220 pagineSolved Mrcog Past Papers 2005 To 2001Betrayin Innocence79% (19)
- Comprehensive Handbook Obstetrics & Gynecology 3rd EdDa EverandComprehensive Handbook Obstetrics & Gynecology 3rd EdValutazione: 5 su 5 stelle5/5 (1)
- Part 1 MrcogDocumento17 paginePart 1 Mrcogaartil88100% (2)
- FRCPath Part 1: Examination Preparation Guide: eBookDa EverandFRCPath Part 1: Examination Preparation Guide: eBookNessuna valutazione finora
- SBA Part 1 MRCOGDocumento247 pagineSBA Part 1 MRCOGHendra Pamukti100% (6)
- PROLOG: Patient Management in the Office, Eighth EditionDa EverandPROLOG: Patient Management in the Office, Eighth EditionNessuna valutazione finora
- @pharmacy7 MRCOG Part 1 One 2ndDocumento1.077 pagine@pharmacy7 MRCOG Part 1 One 2ndAditya Prabawa100% (2)
- MrcogDocumento26 pagineMrcogShafiqueMuhammad100% (1)
- Single-Port Robotic Surgery in Urology: The New Beginning After the Advent of Dedicated PlatformsDa EverandSingle-Port Robotic Surgery in Urology: The New Beginning After the Advent of Dedicated PlatformsRiccardo BertoloNessuna valutazione finora
- EmbryologyDocumento11 pagineEmbryologyWhy YouNessuna valutazione finora
- Top Causes of Recalls September 2016Documento49 pagineTop Causes of Recalls September 2016kyahuaNessuna valutazione finora
- Medical School Companion Obstetrics and Gynecology Practice Question BookDa EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNessuna valutazione finora
- SBAs and EMQs For MRCOG II Addressing The New Exam Format2Documento460 pagineSBAs and EMQs For MRCOG II Addressing The New Exam Format2Hasan Dahamsheh91% (11)
- Mrcog Part 1Documento26 pagineMrcog Part 1JenkRisk100% (2)
- Adel Elkady Sba PDFDocumento290 pagineAdel Elkady Sba PDFAsh Ame100% (2)
- Mrcog 1 Solved Past Papers1997 To 2001Documento219 pagineMrcog 1 Solved Past Papers1997 To 2001Betrayin Innocence93% (15)
- Vagina Anatomy QuestionsDocumento10 pagineVagina Anatomy QuestionsDjabhi SpinzzNessuna valutazione finora
- RCOG Green Top Notes 1Documento48 pagineRCOG Green Top Notes 1Anonymous LnLvsb100% (1)
- Gynecology & Obstetrics 2001-2005 MCQ False)Documento44 pagineGynecology & Obstetrics 2001-2005 MCQ False)Lakshmi Chaitanya100% (4)
- Paper 1 (Gyn) Jan 2018 RecallsDocumento19 paginePaper 1 (Gyn) Jan 2018 Recallshumma100% (1)
- Obs and Gynae Data Interpretation Past PaperDocumento21 pagineObs and Gynae Data Interpretation Past PaperShaheera Shamsudin100% (2)
- MrcogDocumento286 pagineMrcoglina100% (5)
- MRCOG-1 Exam Guide: Syllabus, Format, TopicsDocumento2 pagineMRCOG-1 Exam Guide: Syllabus, Format, TopicsVirithaReddyNessuna valutazione finora
- All RecallsDocumento301 pagineAll RecallsFA Khan100% (2)
- 2017 sepRECALLDocumento58 pagine2017 sepRECALLkyahuaNessuna valutazione finora
- Your Answer: A Correct Answer: BDocumento107 pagineYour Answer: A Correct Answer: Btariq100% (3)
- Paper 2 (OBS) Jan 2018 RecallsDocumento19 paginePaper 2 (OBS) Jan 2018 RecallshummaNessuna valutazione finora
- EMQs For The MRCOG Part 2-The Essential GuideDocumento152 pagineEMQs For The MRCOG Part 2-The Essential GuideJuanda Raynaldi100% (1)
- PASS - MRCOG Physiology 2017Documento46 paginePASS - MRCOG Physiology 2017reffyNessuna valutazione finora
- Multiple page document scanned with CamScannerDocumento39 pagineMultiple page document scanned with CamScannerHuma Khan100% (14)
- Books For Mrcog Part1Documento2 pagineBooks For Mrcog Part1srini100% (3)
- 1 - Anatomy - Pass - Mrcog 2017Documento92 pagine1 - Anatomy - Pass - Mrcog 2017omernouman100% (2)
- MRCOG Part 1 HijauDocumento367 pagineMRCOG Part 1 HijaurifkiNessuna valutazione finora
- Recommended Books For MRCOG Part 2 ExaminationsDocumento9 pagineRecommended Books For MRCOG Part 2 Examinationssaqii67% (6)
- 550 Sbas and MCQS: Mrcog Part 1Documento10 pagine550 Sbas and MCQS: Mrcog Part 1Rizka Adi0% (2)
- Obstetric SBAs MCQDocumento5 pagineObstetric SBAs MCQCofeelovesIronman Javier100% (1)
- Genetics For MrcogDocumento4 pagineGenetics For MrcogsriniNessuna valutazione finora
- Andrew Sizer, Bidyut Kumar, Guy Calcott - Part 2 MRCOG 500 EMQs and SBAs-Cambridge University Press (2019)Documento294 pagineAndrew Sizer, Bidyut Kumar, Guy Calcott - Part 2 MRCOG 500 EMQs and SBAs-Cambridge University Press (2019)rifki100% (2)
- Antenatal management and statisticsDocumento64 pagineAntenatal management and statisticsHasan Dahamsheh100% (4)
- MRCOG Part 2 September 2017 Recalls FinalDocumento13 pagineMRCOG Part 2 September 2017 Recalls FinalSaeed HasanNessuna valutazione finora
- YDS Preposition Soru Tipi PDFDocumento4 pagineYDS Preposition Soru Tipi PDFMuhammed DemirNessuna valutazione finora
- Choose The Most Appropriate Options To Complete The Short Reading ArticlesDocumento20 pagineChoose The Most Appropriate Options To Complete The Short Reading ArticlesEllia45Nessuna valutazione finora
- Mi̇q İngi̇li̇s Di̇li̇ Sinaq İmtahani - Ipg - Az Saytindan YuklenilibDocumento10 pagineMi̇q İngi̇li̇s Di̇li̇ Sinaq İmtahani - Ipg - Az Saytindan YuklenilibCinare100% (1)
- 838 - Advanced Level Grammar Exercise MCQ Test 15Documento4 pagine838 - Advanced Level Grammar Exercise MCQ Test 15BEASTNessuna valutazione finora
- CanDocumento4 pagineCan7erikyano7Nessuna valutazione finora
- PharmaDocumento114 paginePharmaSiva RamanNessuna valutazione finora
- Ogy Ogy: 3 Semester Examination - 2021 3 Semester Examination - 2021Documento2 pagineOgy Ogy: 3 Semester Examination - 2021 3 Semester Examination - 2021gopal trustNessuna valutazione finora
- 1976 Feb 6 Appetites Unchecked by KnowledgeDocumento2 pagine1976 Feb 6 Appetites Unchecked by KnowledgeVvadaHottaNessuna valutazione finora
- International Meat Crisis PDFDocumento174 pagineInternational Meat Crisis PDFTanisha JacksonNessuna valutazione finora
- 4.3 13, YT, DET Sample TestDocumento145 pagine4.3 13, YT, DET Sample TestHamed FroghNessuna valutazione finora
- Soal Bahasa Inggris Kelas 11 IpaDocumento6 pagineSoal Bahasa Inggris Kelas 11 IpaDavid SyaifudinNessuna valutazione finora
- Present Tense VerbDocumento15 paginePresent Tense VerbMai Mai BallanoNessuna valutazione finora
- CH 12 Word ListDocumento3 pagineCH 12 Word ListtigertiaNessuna valutazione finora
- Inihaw Na Liempo: IngredientsDocumento1 paginaInihaw Na Liempo: Ingredientsnmmng2011Nessuna valutazione finora
- The Eats in ShanghaiDocumento52 pagineThe Eats in ShanghaiLee Lay PhengNessuna valutazione finora
- GanapathyDocumento5 pagineGanapathybravindranath5768Nessuna valutazione finora
- Neutral Zone Approach For Rehabilitation of Severely Atrophic RidgeDocumento5 pagineNeutral Zone Approach For Rehabilitation of Severely Atrophic RidgeLynda M. NaranjoNessuna valutazione finora
- NEET UG Biology Evolution PDFDocumento22 pagineNEET UG Biology Evolution PDFamsaeangovanNessuna valutazione finora
- Module 3 Developmental Stages in Middle and Late AdolescenceDocumento21 pagineModule 3 Developmental Stages in Middle and Late Adolescencejulietpamintuan100% (5)
- Digital Booklet - CalifornicationDocumento11 pagineDigital Booklet - CalifornicationChristian Campos0% (1)
- Argumentative EssayDocumento4 pagineArgumentative Essayapi-527619279Nessuna valutazione finora
- Phonetic Animals ListDocumento6 paginePhonetic Animals ListJOHN. J MESANessuna valutazione finora
- ProverbDocumento38 pagineProverbAnkita GoelNessuna valutazione finora
- 2nd QRTR Anet ReteachDocumento13 pagine2nd QRTR Anet Reteachapi-310709379Nessuna valutazione finora
- Antiremed Kelas 08 Bahasa Inggris: Chapter 4 - Latihan SoalDocumento3 pagineAntiremed Kelas 08 Bahasa Inggris: Chapter 4 - Latihan SoalNonna ShellyNessuna valutazione finora
- Types of ClaimsDocumento14 pagineTypes of ClaimsCatherine Joy ManaloNessuna valutazione finora
- Demidov - A Shooting Trip To Kamchatka 1904Documento360 pagineDemidov - A Shooting Trip To Kamchatka 1904Tibor Bánfalvi100% (1)
- Mubashir's Reading TaskDocumento15 pagineMubashir's Reading TaskMuhammad AliNessuna valutazione finora
- The Cat Burglar's RetirementDocumento3 pagineThe Cat Burglar's RetirementrachaelNessuna valutazione finora
- Vector Borne DiseasesDocumento23 pagineVector Borne DiseasesKanishk BhatiaNessuna valutazione finora
- Racy Telenovelas Drive Social ChangeDocumento19 pagineRacy Telenovelas Drive Social Changebhavith akulaNessuna valutazione finora
- Ujian Masuk Program Pascasarjana: Jangan Dibuka Dulu. Tunggu PetunjukDocumento21 pagineUjian Masuk Program Pascasarjana: Jangan Dibuka Dulu. Tunggu PetunjukLalu SuhaimiNessuna valutazione finora
- Recommended Cards: Effect MonstersDocumento35 pagineRecommended Cards: Effect MonstersBela YusdiantikaNessuna valutazione finora
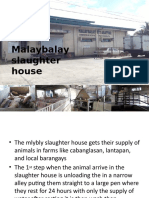
- Ansci 30 Slaughter HouseDocumento34 pagineAnsci 30 Slaughter HouseDieanne MaeNessuna valutazione finora
- Microbiological Monitoring - RODACDocumento2 pagineMicrobiological Monitoring - RODACdeden.drj19Nessuna valutazione finora
- Grammar Exercises - Simple Past TenseDocumento6 pagineGrammar Exercises - Simple Past TensePatty JonasNessuna valutazione finora
- THE STAG - Class NotesDocumento3 pagineTHE STAG - Class Notesmishka100% (1)