Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Case PresentationDocumento27 pagineCase PresentationAjayNessuna valutazione finora
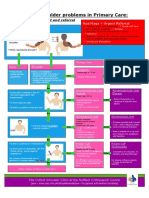
- NHS UK Diagnosis of Shoulder ProblemsDocumento1 paginaNHS UK Diagnosis of Shoulder ProblemsmertNessuna valutazione finora
- NCP Rheumatoid ArthritisDocumento2 pagineNCP Rheumatoid ArthritisMark Zedrix MediarioNessuna valutazione finora
- Escala de Diagnóstico (SI5) de Disfunción de La Articulación Sacroiliaca Estudio PilotoDocumento8 pagineEscala de Diagnóstico (SI5) de Disfunción de La Articulación Sacroiliaca Estudio PilotoLuis HerreraNessuna valutazione finora
- Jurnal Gerontik No IssnDocumento15 pagineJurnal Gerontik No IssnFiradilla ZaskiaNessuna valutazione finora
- A Field Guide To Joint Disease in Archaelogy - Rogers e Waldron PDFDocumento66 pagineA Field Guide To Joint Disease in Archaelogy - Rogers e Waldron PDFD BarbosaNessuna valutazione finora
- Ophtha Quiz - Glaucoma & UveitisDocumento3 pagineOphtha Quiz - Glaucoma & UveitisadiNessuna valutazione finora
- OsteoarthritisDocumento10 pagineOsteoarthritisRehanNessuna valutazione finora
- Best Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihDocumento7 pagineBest Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihARS University BandungNessuna valutazione finora
- Interpreting The Orthopaedic X-Rays - NewDocumento29 pagineInterpreting The Orthopaedic X-Rays - NewSanju427Nessuna valutazione finora
- Effects of Osteoarthritis and Fatigue On Proprioception of The Knee JointDocumento5 pagineEffects of Osteoarthritis and Fatigue On Proprioception of The Knee JointRosaneLacerdaNessuna valutazione finora
- Biomechanics of The Spine1 (Chapter5.t)Documento24 pagineBiomechanics of The Spine1 (Chapter5.t)Z .TNessuna valutazione finora
- 7 Uleiuri Esentiale Pentru ReumatismDocumento3 pagine7 Uleiuri Esentiale Pentru ReumatismDorel ManNessuna valutazione finora
- Function: What Is The Skeletal System?Documento6 pagineFunction: What Is The Skeletal System?Mr. Christian ParabuacNessuna valutazione finora
- Case On Acute Rheumatoid ArthritisDocumento15 pagineCase On Acute Rheumatoid ArthritisdeepakNessuna valutazione finora
- Outline Cast and TractionDocumento9 pagineOutline Cast and Tractionjulieyauder624Nessuna valutazione finora
- Care Plan For Septic ArthritisDocumento5 pagineCare Plan For Septic ArthritisSundaraBharathi57% (7)
- Sports Medicine Exam2020 QQ - 1Documento22 pagineSports Medicine Exam2020 QQ - 1Volc100% (1)
- Homework 6 - JointsDocumento5 pagineHomework 6 - JointsAdwoa OkohNessuna valutazione finora
- Arthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.Documento12 pagineArthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.C Martin TraumatoNessuna valutazione finora
- Drug-Study KetorolacDocumento1 paginaDrug-Study KetorolacMonique CandidoNessuna valutazione finora
- Dequervain MWMDocumento12 pagineDequervain MWMirongrafNessuna valutazione finora
- Complex Elbow InstabilityDocumento9 pagineComplex Elbow InstabilityAristoteles Plato SocratesNessuna valutazione finora
- Juvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16Documento15 pagineJuvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16KathirNessuna valutazione finora
- Normative Values For Isometric Muscle Force by Handheld DynamometerDocumento14 pagineNormative Values For Isometric Muscle Force by Handheld DynamometerWasemBhatNessuna valutazione finora
- Knee Special TestDocumento89 pagineKnee Special TestNURUL AFIQAH NORKHAMISZANNessuna valutazione finora
- DR Yuliasih PIN PABDI FinalDocumento26 pagineDR Yuliasih PIN PABDI FinalAri SimbaraNessuna valutazione finora
- Resource Unit Rheumatoid Arthritis MustaphaDocumento7 pagineResource Unit Rheumatoid Arthritis MustaphaAlyssa Ashley A. ImamNessuna valutazione finora
- Cronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementDocumento4 pagineCronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementAnandhu GNessuna valutazione finora
- Rachel Scott - Anatomy of Bone Joints Jan 2019Documento7 pagineRachel Scott - Anatomy of Bone Joints Jan 2019idyogaNessuna valutazione finora