Potrebbero piacerti anche
- ABHA Coil ProportionsDocumento5 pagineABHA Coil ProportionsOctav OctavianNessuna valutazione finora
- XXX. MCQ Cardiovascular System Book 315-336Documento19 pagineXXX. MCQ Cardiovascular System Book 315-336Maria OnofreiNessuna valutazione finora
- Coronary Atery Disease-Htn-Thrombo QuestionsDocumento38 pagineCoronary Atery Disease-Htn-Thrombo Questionssrivari sriniNessuna valutazione finora
- Cardiac Physiology MCQsDocumento13 pagineCardiac Physiology MCQsالعراقي الصامد100% (2)
- Final Questions 2021Documento8 pagineFinal Questions 2021PatrycjaSkierkaNessuna valutazione finora
- The Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersDocumento609 pagineThe Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersShakir Daddy-Phatstacks Cannon100% (1)
- Blood MCQDocumento24 pagineBlood MCQBijay Kumar MahatoNessuna valutazione finora
- MCQ CardioDocumento12 pagineMCQ CardioAhmed MahanaNessuna valutazione finora
- Vq40de Service ManualDocumento257 pagineVq40de Service Manualjaumegus100% (4)
- All Past Rounds Cardio MCQs AlexandriaDocumento37 pagineAll Past Rounds Cardio MCQs AlexandriaMahmoud Abouelsoud100% (1)
- Cvs MCQ Exam 2008Documento14 pagineCvs MCQ Exam 2008ZH. omg sarNessuna valutazione finora
- CVS MCQ 2010 PDFDocumento23 pagineCVS MCQ 2010 PDFjuniorebinda60% (5)
- CVS MCQsDocumento21 pagineCVS MCQsMohammed Boyka100% (1)
- Heart McqsDocumento33 pagineHeart McqsNaghman Zuberi75% (16)
- MCQ Cardio 2Documento54 pagineMCQ Cardio 2Dian Paramita100% (1)
- Respiratory MCQDocumento3 pagineRespiratory MCQMarjina Khatoon NipuNessuna valutazione finora
- CPSP Demo Questions With Key - PDF Version 1Documento23 pagineCPSP Demo Questions With Key - PDF Version 1Arshad AliNessuna valutazione finora
- Paper C 2019 With Key andDocumento28 paginePaper C 2019 With Key andaizaz100% (1)
- بنك الأسئلةDocumento775 pagineبنك الأسئلةسماح صلاح100% (1)
- Cardiology Mcq's Part - 1Documento31 pagineCardiology Mcq's Part - 1aymenNessuna valutazione finora
- The DIRKS Methodology: A User GuideDocumento285 pagineThe DIRKS Methodology: A User GuideJesus Frontera100% (2)
- 012 CardiacDocumento41 pagine012 CardiacAhmed Zaghw100% (1)
- CVS MCQDocumento14 pagineCVS MCQNur Hamizah Md FuziNessuna valutazione finora
- Renal MCQ 4Documento10 pagineRenal MCQ 4AzizNessuna valutazione finora
- Quiz Cardiovascular Part 3 of 3Documento60 pagineQuiz Cardiovascular Part 3 of 3MedShare100% (7)
- Ganong Physiology Mcqs & SeqsDocumento193 pagineGanong Physiology Mcqs & SeqsRichardNessuna valutazione finora
- MCQ CVS PDFDocumento22 pagineMCQ CVS PDFGovindaraju Subramani100% (1)
- Neurology Multiple Choice Questions With Explanations: Volume IIIDa EverandNeurology Multiple Choice Questions With Explanations: Volume IIIValutazione: 4.5 su 5 stelle4.5/5 (6)
- Respiratory Failure MCQ and QuestionsDocumento5 pagineRespiratory Failure MCQ and QuestionsChikezie Onwukwe67% (3)
- Exam 2018 PDFDocumento62 pagineExam 2018 PDFWondimu Koy100% (1)
- Physiology McqsDocumento5 paginePhysiology McqsFaisal AwanNessuna valutazione finora
- Cardiovascular MCQs LJDocumento11 pagineCardiovascular MCQs LJYanis Yan100% (1)
- Investment Analysis and Portfolio Management: Frank K. Reilly & Keith C. BrownDocumento113 pagineInvestment Analysis and Portfolio Management: Frank K. Reilly & Keith C. BrownWhy you want to knowNessuna valutazione finora
- Pulm 2005 Exam QuestionsDocumento32 paginePulm 2005 Exam QuestionsItharshan IndreswaranNessuna valutazione finora
- CVS Trial ExamDocumento29 pagineCVS Trial ExamAssale Maen100% (1)
- Cardiology 2015-mcqsDocumento78 pagineCardiology 2015-mcqsAsif Newaz100% (1)
- MCQs PulmonologyDocumento2 pagineMCQs PulmonologySadia Batool86% (7)
- RenalDocumento8 pagineRenalVallesh ShettyNessuna valutazione finora
- MCQ IM DepDocumento183 pagineMCQ IM DepHesham A100% (3)
- Renal Disease McqsDocumento20 pagineRenal Disease McqsShankar Deshmukh100% (1)
- Self-Assessment: BOFs for MRCP(UK) and MRCP(I) Part IDa EverandSelf-Assessment: BOFs for MRCP(UK) and MRCP(I) Part INessuna valutazione finora
- Neurology Multiple Choice Questions With Explanations: Volume IDa EverandNeurology Multiple Choice Questions With Explanations: Volume IValutazione: 4 su 5 stelle4/5 (7)
- Medicine-I Important BCQSDocumento10 pagineMedicine-I Important BCQSShairy SohoNessuna valutazione finora
- Medicine I Past BCQsDocumento25 pagineMedicine I Past BCQsShairy SohoNessuna valutazione finora
- Heart, Nerve and Mucsle, Membrane Transport Mcqs With KeyDocumento8 pagineHeart, Nerve and Mucsle, Membrane Transport Mcqs With KeyMudassar Roomi100% (7)
- Cardio SLE Mcqs With AnswersDocumento37 pagineCardio SLE Mcqs With AnswersAsif Newaz100% (4)
- 47 MCQs On GI and Nutrition PhysiologyDocumento14 pagine47 MCQs On GI and Nutrition Physiologyrazsubedi100% (1)
- Ecg Mcqs 1700 DR - AfsanaDocumento5 pagineEcg Mcqs 1700 DR - AfsanaSamah Khan100% (2)
- 003 Pathology MCQ ACEM Primary CardiovascularDocumento5 pagine003 Pathology MCQ ACEM Primary Cardiovascularbmhsh100% (2)
- 15 Miscellaneous Bacteria PDFDocumento2 pagine15 Miscellaneous Bacteria PDFAnne MorenoNessuna valutazione finora
- Gi Physiology Mcqs 24 Aug 04Documento7 pagineGi Physiology Mcqs 24 Aug 04Ran AccNessuna valutazione finora
- Cardiology MCQDocumento7 pagineCardiology MCQNesma Adel100% (1)
- Lung MCQDocumento7 pagineLung MCQArvinth Guna Segaran100% (2)
- Landscape ArchitectureDocumento9 pagineLandscape Architecturelisan2053Nessuna valutazione finora
- 1 Medicine MCQs - CNSDocumento10 pagine1 Medicine MCQs - CNSDiwakesh C B80% (5)
- Neurology: Self-Assessment for MRCP(UK) Neurology SCEDa EverandNeurology: Self-Assessment for MRCP(UK) Neurology SCEValutazione: 5 su 5 stelle5/5 (1)
- Investigation Data FormDocumento1 paginaInvestigation Data Formnildin danaNessuna valutazione finora
- GIT MCQs DR - Ahmed MowafyDocumento15 pagineGIT MCQs DR - Ahmed Mowafya7wfNessuna valutazione finora
- Advanced Oil Gas Accounting International Petroleum Accounting International Petroleum Operations MSC Postgraduate Diploma Intensive Full TimeDocumento70 pagineAdvanced Oil Gas Accounting International Petroleum Accounting International Petroleum Operations MSC Postgraduate Diploma Intensive Full TimeMoheieldeen SamehNessuna valutazione finora
- CVS MCQsDocumento1 paginaCVS MCQsManisha JindalNessuna valutazione finora
- MCQs and Cases 5th YearDocumento118 pagineMCQs and Cases 5th Yearyoune6Nessuna valutazione finora
- Git & Nutrition McqsDocumento24 pagineGit & Nutrition McqsShahabuddin Shaikh100% (1)
- MCQ CardiologyDocumento2 pagineMCQ Cardiologyvishaljairam100% (1)
- Medical Science MCQs Practice Test 1 PDFDocumento3 pagineMedical Science MCQs Practice Test 1 PDFHazim Rhman AliNessuna valutazione finora
- Lange - Endocrine - Physiology Self-Assessment Study QuestionsDocumento19 pagineLange - Endocrine - Physiology Self-Assessment Study QuestionsDimsy Flora KpaiNessuna valutazione finora
- General Medicine - Surgery IV YearDocumento40 pagineGeneral Medicine - Surgery IV YearCynthia GNessuna valutazione finora
- Hech MCQDocumento9 pagineHech MCQamol dahiphaleNessuna valutazione finora
- Endocrine Pathology Mcqs Set 1Documento1 paginaEndocrine Pathology Mcqs Set 1Ho Yong Wai100% (2)
- EPMS System Guide For Subcontractor - V1 2Documento13 pagineEPMS System Guide For Subcontractor - V1 2AdouaneNassim100% (2)
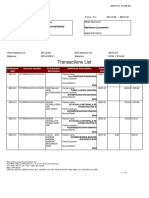
- Transactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinDocumento12 pagineTransactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinConstantin MarilenaNessuna valutazione finora
- Vendor Registration FormDocumento4 pagineVendor Registration FormhiringNessuna valutazione finora
- Bagian AwalDocumento17 pagineBagian AwalCitra Monalisa LaoliNessuna valutazione finora
- FINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Documento45 pagineFINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Edmar Cielo SarmientoNessuna valutazione finora
- CV Ashish PDFDocumento3 pagineCV Ashish PDFRoshan KejariwalNessuna valutazione finora
- Less Homework More TroubleDocumento7 pagineLess Homework More Troubleg697a0mw100% (1)
- Subeeka Akbar Advance NutritionDocumento11 pagineSubeeka Akbar Advance NutritionSubeeka AkbarNessuna valutazione finora
- Stratum CorneumDocumento4 pagineStratum CorneumMuh Firdaus Ar-RappanyNessuna valutazione finora
- Energy Production From Speed BreakerDocumento44 pagineEnergy Production From Speed BreakerMuhammad Bilal67% (3)
- Formato MultimodalDocumento1 paginaFormato MultimodalcelsoNessuna valutazione finora
- Oil List: Audi Front Axle DriveDocumento35 pagineOil List: Audi Front Axle DriveAska QianNessuna valutazione finora
- Ferobide Applications Brochure English v1 22Documento8 pagineFerobide Applications Brochure English v1 22Thiago FurtadoNessuna valutazione finora
- Catalogo PukangDocumento41 pagineCatalogo PukangClarita Muller LeigueNessuna valutazione finora
- Chapter 4: Thermal ComfortDocumento16 pagineChapter 4: Thermal ComfortWengelNessuna valutazione finora
- P01 - PT in Building & Its AdvantagesDocumento11 pagineP01 - PT in Building & Its AdvantagesPartha Pratim RoyNessuna valutazione finora
- Flight Data Recorder Rule ChangeDocumento7 pagineFlight Data Recorder Rule ChangeIgnacio ZupaNessuna valutazione finora
- Concise Selina Solutions Class 9 Maths Chapter 15 Construction of PolygonsDocumento31 pagineConcise Selina Solutions Class 9 Maths Chapter 15 Construction of Polygonsbhaskar51178Nessuna valutazione finora
- Pediatric Fever of Unknown Origin: Educational GapDocumento14 paginePediatric Fever of Unknown Origin: Educational GapPiegl-Gulácsy VeraNessuna valutazione finora
- Ty Baf TaxationDocumento4 pagineTy Baf TaxationAkki GalaNessuna valutazione finora
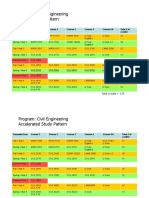
- HKUST 4Y Curriculum Diagram CIVLDocumento4 pagineHKUST 4Y Curriculum Diagram CIVLfrevNessuna valutazione finora