Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Atx Power Supply PFC Schematic PDFDocumento1 paginaAtx Power Supply PFC Schematic PDFzequinhawinsNessuna valutazione finora
- MOS MemoryDocumento53 pagineMOS Memoryskh_1987100% (1)
- The Electric Motor IIDocumento6 pagineThe Electric Motor IIGray Fox GarcíaNessuna valutazione finora
- Sensory QuestionnaireDocumento11 pagineSensory QuestionnaireElisa DellaNessuna valutazione finora
- ET End Sem18Documento3 pagineET End Sem18venkatarao HanumanthuNessuna valutazione finora
- Klemsan Catalogue 2013Documento226 pagineKlemsan Catalogue 2013Tapelea Cristian0% (1)
- Fx5u Pid Control Function PDFDocumento38 pagineFx5u Pid Control Function PDFNutchaiSaengsurathamNessuna valutazione finora
- Dokumen - Tips Ready Admit Card Cooch Behar Without Admit Card Will Not Be Allowed For WrittenDocumento410 pagineDokumen - Tips Ready Admit Card Cooch Behar Without Admit Card Will Not Be Allowed For WrittenCavya DealsNessuna valutazione finora
- Monitoring-Times Magazine Aug 1996Documento116 pagineMonitoring-Times Magazine Aug 1996Benjamin DoverNessuna valutazione finora
- 5 Asahan Street, Pematangsiantar, North Sumatera - 21132: Age Erliando AnggataraDocumento4 pagine5 Asahan Street, Pematangsiantar, North Sumatera - 21132: Age Erliando AnggataraagerliandoNessuna valutazione finora
- P Special Cables GBDocumento16 pagineP Special Cables GBVlado PetkovskiNessuna valutazione finora
- Syed Ahsan: Electrical EngineerDocumento3 pagineSyed Ahsan: Electrical Engineerاحسن سيدNessuna valutazione finora
- Tripple Beam Antenna 6W22ME-01 PDFDocumento3 pagineTripple Beam Antenna 6W22ME-01 PDFTú Hà Văn100% (2)
- Echnical News: Power Factor, What Is It?Documento6 pagineEchnical News: Power Factor, What Is It?Fuji Electric SMBENessuna valutazione finora
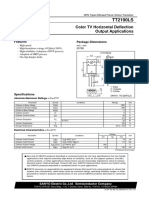
- TT2190LS: Color TV Horizontal Deflection Output ApplicationsDocumento4 pagineTT2190LS: Color TV Horizontal Deflection Output ApplicationsFreddyNessuna valutazione finora
- M SCD enDocumento204 pagineM SCD enMosargt ArgNessuna valutazione finora
- Square Wave GeneratorDocumento6 pagineSquare Wave GeneratorRahul KunduNessuna valutazione finora
- EXLIM Q-D - Section of Surge Arrester Buyers Guide - Edition 11 2014-05 - English - 1HSM 9543 12-00enDocumento8 pagineEXLIM Q-D - Section of Surge Arrester Buyers Guide - Edition 11 2014-05 - English - 1HSM 9543 12-00enmissmoonNessuna valutazione finora
- Astro - Manual - 149 Wedge WelderDocumento12 pagineAstro - Manual - 149 Wedge WelderElnegro NegroNessuna valutazione finora
- Zener DRDocumento4 pagineZener DRArchana SadanandanNessuna valutazione finora
- Declaration of ConformityDocumento1 paginaDeclaration of ConformityhamadaeidNessuna valutazione finora
- Lec10 PDFDocumento29 pagineLec10 PDFNaresh BirudalaNessuna valutazione finora
- Gro-12v-35 - 3 601 JC5 001Documento2 pagineGro-12v-35 - 3 601 JC5 001achmade zakryNessuna valutazione finora
- User Guide: Technique@Documento41 pagineUser Guide: Technique@Apra PashterNessuna valutazione finora
- Screen-Printed, Flexible, Parasitic Beam-Switching Millimeter-Wave Antenna Array For Wearable ApplicationsDocumento9 pagineScreen-Printed, Flexible, Parasitic Beam-Switching Millimeter-Wave Antenna Array For Wearable Applicationsantonio ScacchiNessuna valutazione finora
- Chapter 3. Single-Transistor Primitives An Intuitive Approach (Analog IC Design An Intuitive Approach)Documento26 pagineChapter 3. Single-Transistor Primitives An Intuitive Approach (Analog IC Design An Intuitive Approach)Minh Hai RungNessuna valutazione finora
- Saab 9-5 1998-2000 Model Year ManualDocumento256 pagineSaab 9-5 1998-2000 Model Year ManualSaabDude01Nessuna valutazione finora
- Level 2 Repair: 7-1. Components On The Rear CaseDocumento8 pagineLevel 2 Repair: 7-1. Components On The Rear CaseNguyễn Duy LinhNessuna valutazione finora
- NTE123AP Silicon NPN Transistor Audio Amplifier, Switch (Compl To NTE159)Documento3 pagineNTE123AP Silicon NPN Transistor Audio Amplifier, Switch (Compl To NTE159)Didier DoradoNessuna valutazione finora
- Unit-3 PsocDocumento23 pagineUnit-3 PsocDESI BRAHMNNessuna valutazione finora