Potrebbero piacerti anche
- Selected Topics in the History of Biochemistry. Personal Recollections. Part IIIDa EverandSelected Topics in the History of Biochemistry. Personal Recollections. Part IIIValutazione: 1 su 5 stelle1/5 (1)
- Haem Lecture 2.2016 PDFDocumento12 pagineHaem Lecture 2.2016 PDFdorsa koraeiNessuna valutazione finora
- Introduction To HematologyDocumento95 pagineIntroduction To HematologyAhmad Farhan Hassan0% (1)
- The Hallmarks of CancerDocumento6 pagineThe Hallmarks of CancerSaffronMaeNessuna valutazione finora
- Introduction To HematologyDocumento23 pagineIntroduction To HematologyReba PhiliposeNessuna valutazione finora
- Pathological AnatomyDocumento25 paginePathological AnatomyafrahNessuna valutazione finora
- WHO Manual - The Treatment of DiarrhoeaDocumento47 pagineWHO Manual - The Treatment of DiarrhoeaRamona BunescuNessuna valutazione finora
- Endocrine Disorders 1234399857677955 1Documento130 pagineEndocrine Disorders 1234399857677955 1api-19824701Nessuna valutazione finora
- BLOOD PHYSIOLOGY Study Notes For Medical StudentsDocumento3 pagineBLOOD PHYSIOLOGY Study Notes For Medical StudentsBijay Kumar MahatoNessuna valutazione finora
- Lab ResultsDocumento2 pagineLab Resultsaldrin31Nessuna valutazione finora
- Ist Year MbbsDocumento3 pagineIst Year MbbsJaved Gaba0% (1)
- anatomy 8 scalp تعلم بذكاءDocumento8 pagineanatomy 8 scalp تعلم بذكاءmahmoud ezzeldeenNessuna valutazione finora
- 1 Red Blood Cells Anemia and PolycythemiaDocumento43 pagine1 Red Blood Cells Anemia and PolycythemiaGeevee Naganag VentulaNessuna valutazione finora
- Renal PhysiologyDocumento87 pagineRenal PhysiologyQusaiBadrNessuna valutazione finora
- Calcium & Phosphate MetabolismDocumento36 pagineCalcium & Phosphate MetabolismMustafa KhandgawiNessuna valutazione finora
- Fed Fast CycleDocumento7 pagineFed Fast CycleZahra AlaradiNessuna valutazione finora
- Dr. Niranjan Murthy H.L Assistant Professor Dept of Physiology SSMCDocumento22 pagineDr. Niranjan Murthy H.L Assistant Professor Dept of Physiology SSMCnirilibNessuna valutazione finora
- Osmolarity&tonicitypracticeproblemsfrominternetDocumento14 pagineOsmolarity&tonicitypracticeproblemsfrominternetbsktblbabe88Nessuna valutazione finora
- Metabolism of HemeDocumento138 pagineMetabolism of HemeZafir MonNessuna valutazione finora
- Hallmarks of Cancer IDocumento12 pagineHallmarks of Cancer IMatthew GunnaxNessuna valutazione finora
- Stereochemistry QuestionsDocumento7 pagineStereochemistry Questionsalyson_lNessuna valutazione finora
- Acid - Base Basics: Dr. Fawzeya Aboul Fetouh Prof of Anesthesia Cairo UnversityDocumento54 pagineAcid - Base Basics: Dr. Fawzeya Aboul Fetouh Prof of Anesthesia Cairo UnversityPaolo Uccello100% (1)
- Embryology MnemonicsDocumento5 pagineEmbryology MnemonicsAnnapurna DangetiNessuna valutazione finora
- Acid-Base Disorders NotesDocumento10 pagineAcid-Base Disorders NotesLovely100% (1)
- How To Remember The Brachial PlexusDocumento4 pagineHow To Remember The Brachial PlexusAmanda PachecoNessuna valutazione finora
- FC Derm (SA) Part II Past Papers - 2011 Mar 25-3-2014Documento4 pagineFC Derm (SA) Part II Past Papers - 2011 Mar 25-3-2014matentenNessuna valutazione finora
- Color Atlas of Haematology 2000Documento20 pagineColor Atlas of Haematology 2000Zahraa Al-Sayed100% (1)
- BRS BiochemistryDocumento345 pagineBRS Biochemistrysxymd321100% (1)
- Complete Blood CountDocumento10 pagineComplete Blood CountGenevang Seaweeds100% (1)
- Physiology of DiabetesDocumento52 paginePhysiology of DiabetesPhysiology by Dr RaghuveerNessuna valutazione finora
- Serum Protein ElectrophoresisDocumento7 pagineSerum Protein ElectrophoresisShahrulnizam SaudiNessuna valutazione finora
- E. S. C. Koay Noel Walmsley-A Primer of Chemical PathologyDocumento408 pagineE. S. C. Koay Noel Walmsley-A Primer of Chemical PathologyUdara Senarathne100% (1)
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Documento4 pagineInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauNessuna valutazione finora
- Gastrointestinal HormonesDocumento46 pagineGastrointestinal HormonesTaufiq Singgih BaskoroNessuna valutazione finora
- Basic Science Notes MRCP AssDocumento9 pagineBasic Science Notes MRCP AssUm HamoOdNessuna valutazione finora
- Multiple Choice Questions-Cancers: AdvertisementDocumento5 pagineMultiple Choice Questions-Cancers: AdvertisementSp PpvNessuna valutazione finora
- Endocrinology - Dr. R. SilverDocumento44 pagineEndocrinology - Dr. R. SilverOmoloye AyooluwaNessuna valutazione finora
- Endocrinology NotesDocumento12 pagineEndocrinology Notesrandiey john abelleraNessuna valutazione finora
- Interpret Liver TestsDocumento4 pagineInterpret Liver TestsKaram Ali ShahNessuna valutazione finora
- Acid Base ImbalanceDocumento50 pagineAcid Base ImbalanceDian Pratiwi BurnamaNessuna valutazione finora
- Sir Salahudin Kamal's Pearls All in OneeDocumento156 pagineSir Salahudin Kamal's Pearls All in OneeSHAKEEL1991Nessuna valutazione finora
- General Pathology: Workflow and Safety in The Histopathology LaboratoryDocumento7 pagineGeneral Pathology: Workflow and Safety in The Histopathology LaboratoryJaiy HingcoNessuna valutazione finora
- Urine Dipstick Testing + Common Renal Problem 2012Documento52 pagineUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNessuna valutazione finora
- Biology of C Reactive Protein in Health and Disease PDFDocumento324 pagineBiology of C Reactive Protein in Health and Disease PDFdanielleeNessuna valutazione finora
- 1 Body FluidsDocumento9 pagine1 Body FluidsSenthereng MoaisiNessuna valutazione finora
- Antigen-Antibody Reactions In Vivo: Methods in Immunology and Immunochemistry, Vol. 5Da EverandAntigen-Antibody Reactions In Vivo: Methods in Immunology and Immunochemistry, Vol. 5Nessuna valutazione finora
- RENALMCQDocumento5 pagineRENALMCQkrishnadoctor1Nessuna valutazione finora
- Metabolic OR Endocrine Disorders: Amanda Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistDocumento124 pagineMetabolic OR Endocrine Disorders: Amanda Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistLyn LynNessuna valutazione finora
- Differential Diagnosis of Malaria ParasiteDocumento101 pagineDifferential Diagnosis of Malaria ParasiteSohaib Omer Salih100% (1)
- 03 Cell InjuryDocumento72 pagine03 Cell InjuryLunaLure100% (1)
- EndocrinologyDocumento3 pagineEndocrinologyRumana AliNessuna valutazione finora
- Bleeding Disorders: LCDR Art GeorgeDocumento54 pagineBleeding Disorders: LCDR Art Georgesatya_mdsNessuna valutazione finora
- COMPILED SCTL Adrenal Disorders PDFDocumento14 pagineCOMPILED SCTL Adrenal Disorders PDFeeelie35Nessuna valutazione finora
- Histology of Lymphoid Organ PDFDocumento82 pagineHistology of Lymphoid Organ PDFRionaldy TaminNessuna valutazione finora
- Hormon GDSDocumento23 pagineHormon GDSBRI KUNessuna valutazione finora
- Acid Base Handout RevisedDocumento3 pagineAcid Base Handout RevisedKaren HutchinsonNessuna valutazione finora
- 1.genetic Disorders & Inborn Errors of MetabolismDocumento17 pagine1.genetic Disorders & Inborn Errors of MetabolismAhmed Ali Mohammed AlbashirNessuna valutazione finora
- Clinical Biochemistry: Contemporary Theories and TechniquesDa EverandClinical Biochemistry: Contemporary Theories and TechniquesHerbert SpiegelNessuna valutazione finora
- Commonrashes in Neonates201205suDocumento6 pagineCommonrashes in Neonates201205suDanielcc LeeNessuna valutazione finora
- DNA Genetic Testing, Mar04, Prof Ron TrentDocumento7 pagineDNA Genetic Testing, Mar04, Prof Ron TrentDanielcc LeeNessuna valutazione finora
- Birthmarks Identificationandmx201205ryanDocumento4 pagineBirthmarks Identificationandmx201205ryanDanielcc LeeNessuna valutazione finora
- 14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Documento9 pagine14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Danielcc Lee100% (1)
- Lab TSTNG Acute Diarrhoea Sept03Documento8 pagineLab TSTNG Acute Diarrhoea Sept03Danielcc LeeNessuna valutazione finora
- Interpretation of The eGFR Jul 07Documento8 pagineInterpretation of The eGFR Jul 07Danielcc LeeNessuna valutazione finora
- 14 Essentials To MxMT2013!09!029-BRODATY - 0Documento11 pagine14 Essentials To MxMT2013!09!029-BRODATY - 0Danielcc LeeNessuna valutazione finora
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Documento8 pagineDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNessuna valutazione finora
- Avoiding Unnecessary Laboratory Tests May 2008Documento8 pagineAvoiding Unnecessary Laboratory Tests May 2008Danielcc LeeNessuna valutazione finora
- Biochemical Measurements in OsteoporosisDocumento7 pagineBiochemical Measurements in OsteoporosisDanielcc LeeNessuna valutazione finora
- Bleeding Disorders March 2008Documento8 pagineBleeding Disorders March 2008Danielcc LeeNessuna valutazione finora
- Diabetes Diagnosis and Monitoring, April 2002 Author Peter ColmanDocumento13 pagineDiabetes Diagnosis and Monitoring, April 2002 Author Peter ColmanDanielcc LeeNessuna valutazione finora
- Assessing Renal Function Aug04Documento9 pagineAssessing Renal Function Aug04Danielcc LeeNessuna valutazione finora
- Autoimmune Diseases Mar 2003Documento12 pagineAutoimmune Diseases Mar 2003Danielcc LeeNessuna valutazione finora
- Diagnosis and Management of Chronic Heart Failure 2006: Quick Reference GuideDocumento10 pagineDiagnosis and Management of Chronic Heart Failure 2006: Quick Reference GuideasharobeamNessuna valutazione finora
- Nonalcoholic Fatty Liver DiseaseDocumento4 pagineNonalcoholic Fatty Liver DiseaseDanielcc LeeNessuna valutazione finora
- Evaluation of Sleepy PatientsDocumento4 pagineEvaluation of Sleepy PatientsDanielcc LeeNessuna valutazione finora
- Arthritis - Which Tests To Choose, and Which To Avoid Nov08Documento9 pagineArthritis - Which Tests To Choose, and Which To Avoid Nov08Danielcc LeeNessuna valutazione finora
- Antenatal Screening For Down Syndrome - Nov 2007Documento8 pagineAntenatal Screening For Down Syndrome - Nov 2007Danielcc LeeNessuna valutazione finora
- Spider Bites200911Documento6 pagineSpider Bites200911Danielcc LeeNessuna valutazione finora
- Box Jellyfish - Australian Venom Research UnitDocumento2 pagineBox Jellyfish - Australian Venom Research UnitDanielcc LeeNessuna valutazione finora
- Mammalian Bites200911dendleDocumento6 pagineMammalian Bites200911dendleDanielcc LeeNessuna valutazione finora
- Blood Transfusion ProcedureDocumento0 pagineBlood Transfusion ProcedureDanielcc LeeNessuna valutazione finora
- Mosquito InfoDocumento4 pagineMosquito InfoJessica FornoNessuna valutazione finora
- Coughing Child-Could It Be AsthmaDocumento4 pagineCoughing Child-Could It Be AsthmaDanielcc LeeNessuna valutazione finora
- Diarrhoea in TravellersDocumento5 pagineDiarrhoea in TravellersMazo KhanNessuna valutazione finora
- Work Related Asthma201001Documento4 pagineWork Related Asthma201001Danielcc LeeNessuna valutazione finora
- Bed Bugs: What The GP Needs To KnowDocumento5 pagineBed Bugs: What The GP Needs To KnowDanielcc LeeNessuna valutazione finora
- Deteting Familial Hyperholesterolaemia in General PratieDocumento4 pagineDeteting Familial Hyperholesterolaemia in General PratieDanielcc LeeNessuna valutazione finora
- Health Services in WADocumento10 pagineHealth Services in WAlaureeateNessuna valutazione finora
- LidocaineDocumento11 pagineLidocaineStanford AnesthesiaNessuna valutazione finora
- OITE Review 2013Documento263 pagineOITE Review 2013addison wood100% (2)
- Basic Health ServicesDocumento2 pagineBasic Health ServicesSam Raven AndresNessuna valutazione finora
- Post-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesDocumento10 paginePost-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesJared CossioNessuna valutazione finora
- A Regenerative Interventional Approach To The Management of Degenerative Low Back PainDocumento16 pagineA Regenerative Interventional Approach To The Management of Degenerative Low Back PainAthenaeum Scientific PublishersNessuna valutazione finora
- Principle of Laser Application in Medicine & LASER SAFETY5Documento62 paginePrinciple of Laser Application in Medicine & LASER SAFETY5melisandrianaNessuna valutazione finora
- Lesson Plan For Anatomy and PhysiologyDocumento7 pagineLesson Plan For Anatomy and PhysiologyJamie Bagundol100% (1)
- Leaflet Glycophos 1 (Spesifikasi Produk)Documento2 pagineLeaflet Glycophos 1 (Spesifikasi Produk)Irhamna FauziahNessuna valutazione finora
- Brockton Police Log Updated 10/01/2013Documento19 pagineBrockton Police Log Updated 10/01/2013BB0% (1)
- Drug StudyDocumento4 pagineDrug StudyYasminGianneDeOcampoBarizoNessuna valutazione finora
- DDFGGDocumento2 pagineDDFGGstrafforNessuna valutazione finora
- Typhoid Fever at A GlanceDocumento2 pagineTyphoid Fever at A GlanceLIZNessuna valutazione finora
- Social Stratification in The PhilippinesDocumento11 pagineSocial Stratification in The PhilippinesMichael VillavertNessuna valutazione finora
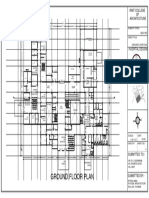
- Ground Floor Plan Sheet 2Documento1 paginaGround Floor Plan Sheet 2riteshNessuna valutazione finora
- Gattefossé Nov 2015 Efficient Skin Delivery No Compromise With TranscutolDocumento16 pagineGattefossé Nov 2015 Efficient Skin Delivery No Compromise With TranscutolJoaozinhoMéndezNessuna valutazione finora
- Interpretation of Histograms and Its Correlation WDocumento5 pagineInterpretation of Histograms and Its Correlation WrezqiNessuna valutazione finora
- No Kode SAP Lokasi Rak Nama ProdukDocumento117 pagineNo Kode SAP Lokasi Rak Nama ProdukKimia ByPass TabananNessuna valutazione finora
- Khalil High Yeild Step 2 Cs Mnemonic 2nd EdDocumento24 pagineKhalil High Yeild Step 2 Cs Mnemonic 2nd EdCarolina Lopez100% (1)
- Emqs ObsDocumento33 pagineEmqs Obsbakkiaha100% (1)
- Rectal ProlapseDocumento9 pagineRectal ProlapseAnjani Putri RetnaninggalihNessuna valutazione finora
- Tetracycline, Doxycycline, minocycline-Tetracyclines-InfenctionsDocumento1 paginaTetracycline, Doxycycline, minocycline-Tetracyclines-InfenctionsNatalia SpencerNessuna valutazione finora
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDocumento84 pagineDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)
- Case of Bataliny v. RussiaDocumento29 pagineCase of Bataliny v. RussiamrbtdfNessuna valutazione finora
- Blood TransfusionDocumento5 pagineBlood TransfusionMoustafa Hazzaa100% (1)
- Opportunity, Challenge and Scope of Natural Products in Medicinal ChemistryDocumento434 pagineOpportunity, Challenge and Scope of Natural Products in Medicinal ChemistryCamilla Karen Fernandes Carneiro100% (1)
- 5 Meo DMTDocumento18 pagine5 Meo DMTJimmy Contreras Rey100% (1)
- Farmasi Manajemen Puskesmas KaliorangDocumento5 pagineFarmasi Manajemen Puskesmas KaliorangDEA REGGIANANessuna valutazione finora
- Massage TherapyDocumento79 pagineMassage TherapyMukesh Duryodhan Hirekhan100% (1)
- 04-09-12 EditionDocumento28 pagine04-09-12 EditionSan Mateo Daily JournalNessuna valutazione finora