Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Medical BillingDocumento229 pagineMedical BillingMohammad Apzar100% (6)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- 2023 - MHA-MABHS State Agency Involved Pediatric Patients - FinalDocumento11 pagine2023 - MHA-MABHS State Agency Involved Pediatric Patients - FinalBoston 25 DeskNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- White Paper: On Joint ReplacementDocumento144 pagineWhite Paper: On Joint ReplacementCosme MejiaNessuna valutazione finora
- Implementation of Kayakalp in HospitalsDocumento212 pagineImplementation of Kayakalp in HospitalsAbdus Subhan A Takildar100% (1)
- Lactation Management Training SampleDocumento12 pagineLactation Management Training SampleCart Sunrise100% (1)
- Diarrhoea Guidelines PDFDocumento58 pagineDiarrhoea Guidelines PDFmustikaarumNessuna valutazione finora
- TP Leads - GurgaonDocumento32 pagineTP Leads - GurgaonDeepika Aggarwal0% (1)
- Outcome Studies On The Efficacy of Art TherapyDocumento11 pagineOutcome Studies On The Efficacy of Art TherapyYashpal MalikNessuna valutazione finora
- Drug Silver Sulfadiazine FlamazineDocumento2 pagineDrug Silver Sulfadiazine Flamazinenj_pink081794100% (1)
- Gastric Volvulus: Bang Chau, Susan DufelDocumento2 pagineGastric Volvulus: Bang Chau, Susan DufelmustikaarumNessuna valutazione finora
- Nutrition and Stroke: Review ArticleDocumento9 pagineNutrition and Stroke: Review Articlerichie_ciandraNessuna valutazione finora
- 24 4 385Documento6 pagine24 4 385mustikaarumNessuna valutazione finora
- Dietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiaDocumento7 pagineDietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiamustikaarumNessuna valutazione finora
- Bushra, 2010Documento7 pagineBushra, 2010Citta ArastiNessuna valutazione finora
- Cooking RequirementsDocumento1 paginaCooking RequirementsvectorNessuna valutazione finora
- Logistics Execution Suite Manages Warehouse OperationsDocumento9 pagineLogistics Execution Suite Manages Warehouse OperationsmustikaarumNessuna valutazione finora
- ViaClinica RICA EnglishDocumento127 pagineViaClinica RICA EnglishmustikaarumNessuna valutazione finora
- Vitamind - TB PDFDocumento7 pagineVitamind - TB PDFmustikaarumNessuna valutazione finora
- Parenteral Nutrition in Critical CareDocumento5 pagineParenteral Nutrition in Critical CaremustikaarumNessuna valutazione finora
- Tingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarDocumento4 pagineTingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarmustikaarumNessuna valutazione finora
- Selected Health IndicatorsDocumento93 pagineSelected Health IndicatorsmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
- Laporan Week 9 BDocumento36 pagineLaporan Week 9 BmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
- Nutrition Management - Sirosis PDFDocumento10 pagineNutrition Management - Sirosis PDFmustikaarumNessuna valutazione finora
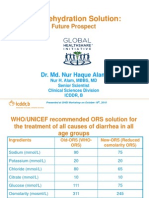
- Oral Rehydration Solution:: Future ProspectDocumento48 pagineOral Rehydration Solution:: Future ProspectmustikaarumNessuna valutazione finora
- BCAADocumento8 pagineBCAAmustikaarumNessuna valutazione finora
- Reliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodDocumento5 pagineReliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodmustikaarumNessuna valutazione finora
- Posterior Sagittal Anorectoplasty in Anorectal MalformationsDocumento5 paginePosterior Sagittal Anorectoplasty in Anorectal MalformationsmustikaarumNessuna valutazione finora
- Ioi 160069Documento9 pagineIoi 160069mustikaarumNessuna valutazione finora
- Hungx BuiDocumento92 pagineHungx BuimustikaarumNessuna valutazione finora
- Nousea and Vomiting Mediciation 130509Documento3 pagineNousea and Vomiting Mediciation 130509mustikaarumNessuna valutazione finora
- Micronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93Documento9 pagineMicronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93mustikaarumNessuna valutazione finora
- 18 Total Quality ApstractDocumento5 pagine18 Total Quality ApstractPooja GuptaNessuna valutazione finora
- Mustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsDocumento18 pagineMustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsmustikaarumNessuna valutazione finora
- Metronidazole Baxter in FDocumento14 pagineMetronidazole Baxter in FmustikaarumNessuna valutazione finora
- Consumer Medicine Information Arrow - Ranitidine: What Is in This LeafletDocumento8 pagineConsumer Medicine Information Arrow - Ranitidine: What Is in This LeafletmustikaarumNessuna valutazione finora
- Metronidazole: Common Drug Name Common Brand NamesDocumento1 paginaMetronidazole: Common Drug Name Common Brand NamesmustikaarumNessuna valutazione finora
- The Role of A Physical Therapist in Spinal Cord Injury RehabilitationDocumento2 pagineThe Role of A Physical Therapist in Spinal Cord Injury Rehabilitationrihamsol2Nessuna valutazione finora
- Chief Nursing Officer VP Nursing in New Orleans LA Resume Mary GenoveseDocumento5 pagineChief Nursing Officer VP Nursing in New Orleans LA Resume Mary GenoveseMary GenoveseNessuna valutazione finora
- Cancer RegistryDocumento36 pagineCancer RegistryJoebe VincyNessuna valutazione finora
- Cna Liscense NumberDocumento2 pagineCna Liscense Numberapi-548066065Nessuna valutazione finora
- TesisDocumento9 pagineTesisRachel SepulvedaNessuna valutazione finora
- Medical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) CategoryDocumento3 pagineMedical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) Categoryscope 3901Nessuna valutazione finora
- Admed Claimant'S Statement: A. Personal DetailsDocumento2 pagineAdmed Claimant'S Statement: A. Personal Detailsshemina armorerNessuna valutazione finora
- Factors influencing nurse absenteeism in South African hospitalsDocumento9 pagineFactors influencing nurse absenteeism in South African hospitalsChandra Hidayat RcrNessuna valutazione finora
- Basics of OncologyDocumento64 pagineBasics of OncologyCiubotaru Diana -MariaNessuna valutazione finora
- Family Planning Health TeachingDocumento1 paginaFamily Planning Health TeachingLoverMind CabaronNessuna valutazione finora
- 2013 NTP Manual Procedures for TB PreventionDocumento32 pagine2013 NTP Manual Procedures for TB PreventionaringkinkingNessuna valutazione finora
- Clinic Duties and Responsibilities UpdatedDocumento5 pagineClinic Duties and Responsibilities UpdatedYssa ManilaNessuna valutazione finora
- Healthcare GeneralDocumento2 pagineHealthcare GeneralkrisluidhardtNessuna valutazione finora
- Literature Review - Jacob HaireDocumento8 pagineLiterature Review - Jacob Haireapi-609397927Nessuna valutazione finora
- Etikolegal Gadar Prof - NursalamDocumento77 pagineEtikolegal Gadar Prof - NursalamIrmaNessuna valutazione finora
- Main Notice of Injury or Occupational Disease Incident Report NevadaDocumento2 pagineMain Notice of Injury or Occupational Disease Incident Report NevadaSamier MohamedNessuna valutazione finora
- Chapter 4Documento19 pagineChapter 4EmmaNessuna valutazione finora
- Scenario Assignment Scenario3Documento4 pagineScenario Assignment Scenario3MonizaBorgesNessuna valutazione finora
- Xlri GMP ProfileDocumento64 pagineXlri GMP ProfileManish VermaNessuna valutazione finora
- Facts and Figures: Geographical and Demographic ProfileDocumento4 pagineFacts and Figures: Geographical and Demographic ProfileJulius MarcelinoNessuna valutazione finora
- Focus Pdca WorksheetDocumento2 pagineFocus Pdca Worksheetapi-256214553Nessuna valutazione finora
- Chapter 16 Psychtx BasicDocumento28 pagineChapter 16 Psychtx Basicosrah_gNessuna valutazione finora