Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Robin Goh: This Is To Certify ThatDocumento1 paginaRobin Goh: This Is To Certify ThatYhr YhNessuna valutazione finora
- NetBank - TransactionsDocumento1 paginaNetBank - TransactionsYhr YhNessuna valutazione finora
- Pathophysiology On ArrhythmiaDocumento34 paginePathophysiology On ArrhythmiaYhr Yh100% (1)
- Hyperlipidaemias (MRCP+ Step 1)Documento2 pagineHyperlipidaemias (MRCP+ Step 1)Yhr YhNessuna valutazione finora
- The Pale Yellow in The Aorta Are The Earliest Lesion of AtherosclerosisDocumento1 paginaThe Pale Yellow in The Aorta Are The Earliest Lesion of AtherosclerosisYhr YhNessuna valutazione finora
- Pathophysiology of Myocardial InfarctionDocumento4 paginePathophysiology of Myocardial InfarctionYhr YhNessuna valutazione finora
- Bets - DunningrDocumento5 pagineBets - DunningrYhr YhNessuna valutazione finora
- CP 111Documento246 pagineCP 111Yhr YhNessuna valutazione finora
- JVPDocumento5 pagineJVPYhr YhNessuna valutazione finora
- CCCCDocumento1 paginaCCCCYhr YhNessuna valutazione finora
- Orientation - Booklet DeclarationDocumento1 paginaOrientation - Booklet DeclarationYhr YhNessuna valutazione finora
- Reviewer's Report Title: Cutaneous Squamous Cell Carcinoma Metastatic To Parotid - Analysis ofDocumento2 pagineReviewer's Report Title: Cutaneous Squamous Cell Carcinoma Metastatic To Parotid - Analysis ofYhr YhNessuna valutazione finora
- Feasibidlity For AustraliaDocumento13 pagineFeasibidlity For AustraliaYhr YhNessuna valutazione finora
- Fair Work Information Statement Acknowledgement FormDocumento1 paginaFair Work Information Statement Acknowledgement FormYhr YhNessuna valutazione finora
- Microsoft Word - Choice of Superannuation Fund Form - HESTADocumento2 pagineMicrosoft Word - Choice of Superannuation Fund Form - HESTAYhr YhNessuna valutazione finora
- HESTA Product Disclosure Statement September 2012Documento28 pagineHESTA Product Disclosure Statement September 2012Yhr YhNessuna valutazione finora
- LBU F VL MR9 VehicleTransferDocumento6 pagineLBU F VL MR9 VehicleTransferYhr YhNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- UROLOGYDocumento3 pagineUROLOGYNoneNessuna valutazione finora
- Osteogenic Sarcoma (Osteosarcoma)Documento12 pagineOsteogenic Sarcoma (Osteosarcoma)Carmella CaritosNessuna valutazione finora
- FCM3-3.02 Philippine Cancer Control ProgramDocumento11 pagineFCM3-3.02 Philippine Cancer Control ProgramJoher MendezNessuna valutazione finora
- CNS Tumors NeurologyDocumento45 pagineCNS Tumors NeurologyChristinaNessuna valutazione finora
- Gambaran Pengetahuan Pencegahan Kanker ServiksDocumento10 pagineGambaran Pengetahuan Pencegahan Kanker ServiksSabrina Nadjib Mohamad -Nessuna valutazione finora
- Stabt 2Documento62 pagineStabt 2Kate Camille SoteloNessuna valutazione finora
- ChemotherapyDocumento16 pagineChemotherapyCandida NickensNessuna valutazione finora
- NEUROPATHOLOGYDocumento28 pagineNEUROPATHOLOGYPratama SutardiNessuna valutazione finora
- Policitemia VeraDocumento14 paginePolicitemia VeraVicky MolinaNessuna valutazione finora
- Ayurveda Herbal Liver Cancer CureDocumento7 pagineAyurveda Herbal Liver Cancer CureChirag Patel100% (1)
- Bladder 4.1.0.0.rel CapcpDocumento19 pagineBladder 4.1.0.0.rel CapcpkarimahihdaNessuna valutazione finora
- Bone Tumors - Clues and CuesDocumento97 pagineBone Tumors - Clues and CuesRhyRhye Sawitri AriantiNessuna valutazione finora
- 3 - NCM112Documento6 pagine3 - NCM112Edthel IniegoNessuna valutazione finora
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDocumento8 pagineCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianNessuna valutazione finora
- WHO Classifications of Lung TumorDocumento26 pagineWHO Classifications of Lung Tumorayeshanabilla8808100% (1)
- American Cancer SocietyDocumento56 pagineAmerican Cancer SocietyranaNessuna valutazione finora
- Stase Gastro - Multiple Nodul HeparDocumento13 pagineStase Gastro - Multiple Nodul HeparRozen RyuhaNessuna valutazione finora
- Test Bank For The Biology of Cancer Second EditionDocumento7 pagineTest Bank For The Biology of Cancer Second EditionDale Passe100% (26)
- Ebook Clinical Gynecologic Oncology PDF Full Chapter PDFDocumento67 pagineEbook Clinical Gynecologic Oncology PDF Full Chapter PDFalton.kanahele202100% (26)
- BJR 17982822Documento6 pagineBJR 17982822Ther RayNessuna valutazione finora
- Lord'S Angels Montessori School, Inc. M - /20 A - /20 H - /20Documento4 pagineLord'S Angels Montessori School, Inc. M - /20 A - /20 H - /20Rose Ann VillanuevaNessuna valutazione finora
- Toledo, John Carlo - Colon CancerDocumento13 pagineToledo, John Carlo - Colon CancerKristine YoungNessuna valutazione finora
- WIL - English Does Work 7 Cronica WRITINGDocumento2 pagineWIL - English Does Work 7 Cronica WRITINGwilbert edill rodriguez martinez50% (2)
- Nrg-Gi002 Protocol PresentationDocumento16 pagineNrg-Gi002 Protocol Presentationapi-508897697Nessuna valutazione finora
- RT For General PublicDocumento24 pagineRT For General Publicraheel252100% (1)
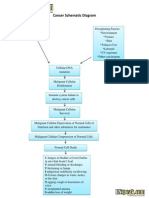
- Cancer Schematic DiagramDocumento1 paginaCancer Schematic DiagramCyrus De Asis100% (4)
- Tema e Diplomes Kanceri GastrikDocumento35 pagineTema e Diplomes Kanceri GastrikDorisa BahjaNessuna valutazione finora
- Pancreatic Cancer - Clinical Management-Intech (2012)Documento324 paginePancreatic Cancer - Clinical Management-Intech (2012)María Reynel TarazonaNessuna valutazione finora
- Gynecologic OncologyDocumento16 pagineGynecologic OncologyBioleagues EventsNessuna valutazione finora
- Angka Tahan Hidup Penderita Kanker Paru Bukan KarsinomaDocumento8 pagineAngka Tahan Hidup Penderita Kanker Paru Bukan KarsinomaFebrinaHutasosweetNessuna valutazione finora