Potrebbero piacerti anche
- ListDocumento1 paginaListSatyendra KumarNessuna valutazione finora
- Rappelli Coccia RondoniDocumento6 pagineRappelli Coccia RondoniMohamed VandettaNessuna valutazione finora
- Whitepaper en E5303 E5306 E5353 Xperia c4Documento23 pagineWhitepaper en E5303 E5306 E5353 Xperia c4Satyendra KumarNessuna valutazione finora
- 37580145Documento8 pagine37580145Satyendra KumarNessuna valutazione finora
- Flabby RidgeDocumento4 pagineFlabby RidgeBrijesh MaskeyNessuna valutazione finora
- BDocumento15 pagineBSatyendra KumarNessuna valutazione finora
- A Review of Pros Tho Don Tic Management of Fibrous RidgesDocumento5 pagineA Review of Pros Tho Don Tic Management of Fibrous RidgesMohsin HabibNessuna valutazione finora
- ListDocumento1 paginaListSatyendra KumarNessuna valutazione finora
- Resor PtionDocumento13 pagineResor PtionSatyendra KumarNessuna valutazione finora
- FPD DesignDocumento9 pagineFPD DesignMohamed AliNessuna valutazione finora
- Review Small Diameter ImplantsDocumento11 pagineReview Small Diameter ImplantsSatyendra KumarNessuna valutazione finora
- Teeth in a Day: The Branemark Novum SystemDocumento4 pagineTeeth in a Day: The Branemark Novum SystemSatyendra KumarNessuna valutazione finora
- 084 03Documento6 pagine084 03Satyendra KumarNessuna valutazione finora
- 11999539Documento11 pagine11999539Satyendra KumarNessuna valutazione finora
- 11999539Documento11 pagine11999539Satyendra KumarNessuna valutazione finora
- Scientific Review - Narrow Implants (79179)Documento2 pagineScientific Review - Narrow Implants (79179)Satyendra KumarNessuna valutazione finora
- 37580145Documento8 pagine37580145Satyendra KumarNessuna valutazione finora
- Abstracts - Kurze, Schmale Implantate 1Documento53 pagineAbstracts - Kurze, Schmale Implantate 1Satyendra KumarNessuna valutazione finora
- 64690685Documento7 pagine64690685Satyendra KumarNessuna valutazione finora
- 11999539Documento11 pagine11999539Satyendra KumarNessuna valutazione finora
- 1 s2.0 S2210815712000339 MainDocumento4 pagine1 s2.0 S2210815712000339 MainSatyendra KumarNessuna valutazione finora
- Scientific Review - Narrow Implants (79179)Documento2 pagineScientific Review - Narrow Implants (79179)Satyendra KumarNessuna valutazione finora
- Participants From GITAM Dental College For Cultural in Vijayawada ConferenceDocumento1 paginaParticipants From GITAM Dental College For Cultural in Vijayawada ConferenceSatyendra KumarNessuna valutazione finora
- 084 03Documento6 pagine084 03Satyendra KumarNessuna valutazione finora
- Direct Relining of Dentures With Soft Materials: Mutluay & RuyterDocumento2 pagineDirect Relining of Dentures With Soft Materials: Mutluay & RuyterSatyendra KumarNessuna valutazione finora
- Titanium and Its AlloysDocumento63 pagineTitanium and Its AlloysSatyendra KumarNessuna valutazione finora
- 1 s2.0 S0109564106003149 MainDocumento9 pagine1 s2.0 S0109564106003149 MainSatyendra KumarNessuna valutazione finora
- Study On Ti SheetDocumento11 pagineStudy On Ti SheetSatyendra KumarNessuna valutazione finora
- Dental Materials ScienceDocumento89 pagineDental Materials ScienceWilan Dita NesyiaNessuna valutazione finora
- Sports ScheduleDocumento3 pagineSports ScheduleSatyendra KumarNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Big Four by Rolf GordonDocumento40 pagineThe Big Four by Rolf GordonArcanistNessuna valutazione finora
- Chicken Pox SOAPDocumento8 pagineChicken Pox SOAPKevin NyasogoNessuna valutazione finora
- PARASITOLOGY (Quizlet)Documento9 paginePARASITOLOGY (Quizlet)Allyssa AniNessuna valutazione finora
- Briefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Documento16 pagineBriefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Sheila Tirta AyumurtiNessuna valutazione finora
- G.R. No. 196102 November 26, 2014 Government Service Insurance System, Petitioner, AURELIA Y. CALUMPIANO, RespondentDocumento4 pagineG.R. No. 196102 November 26, 2014 Government Service Insurance System, Petitioner, AURELIA Y. CALUMPIANO, RespondentMarra RicaldeNessuna valutazione finora
- AEF2e TB4 VP 2Documento2 pagineAEF2e TB4 VP 2Minji LeeNessuna valutazione finora
- CHN-Week 1Documento4 pagineCHN-Week 1rich_dela_china100% (3)
- Medical AbbreviationDocumento13 pagineMedical AbbreviationRaf Luis100% (1)
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDocumento287 pagineThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALINessuna valutazione finora
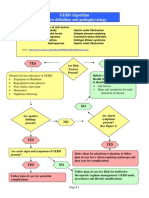
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocumento3 pagineGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNessuna valutazione finora
- Non-Plaque Induced GingivitisDocumento30 pagineNon-Plaque Induced GingivitisDentist AymanNessuna valutazione finora
- Occupational Diseases 302-04280 enDocumento19 pagineOccupational Diseases 302-04280 enJithesh S VNessuna valutazione finora
- Metabolic Acidosis: Irish Grace A. Dayao Dra. RamosDocumento14 pagineMetabolic Acidosis: Irish Grace A. Dayao Dra. RamosBing DayaoNessuna valutazione finora
- Friedreich's Ataxia: Anatomical Structures AffectedDocumento26 pagineFriedreich's Ataxia: Anatomical Structures AffectedAparna RawatNessuna valutazione finora
- Preeclampsia and EclampsiaDocumento24 paginePreeclampsia and EclampsiaFawzia Haznah Nurul ImaniNessuna valutazione finora
- Nonparametric Test: DR - Dr. Siswanto, MSCDocumento44 pagineNonparametric Test: DR - Dr. Siswanto, MSCFikhyRizkyHapsariNessuna valutazione finora
- Thyroid Disease Anesthetic ConsiderationsDocumento30 pagineThyroid Disease Anesthetic Considerationssachin10dulkarNessuna valutazione finora
- Ludwig AnginaDocumento5 pagineLudwig AnginaSiti Aprilia wahyuniNessuna valutazione finora
- Test Bank Chapter 6: Older Adults: Lewis: Medical-Surgical Nursing, 7 EditionDocumento11 pagineTest Bank Chapter 6: Older Adults: Lewis: Medical-Surgical Nursing, 7 EditionBriseidaSolisNessuna valutazione finora
- Ilovepdf MergedDocumento351 pagineIlovepdf MergedSwara SawantNessuna valutazione finora
- Semi-Detailed LP-Linear and Non - Linear TextDocumento6 pagineSemi-Detailed LP-Linear and Non - Linear TextFlordelis Blanco LisaoNessuna valutazione finora
- Gabriel Ogun StateDocumento15 pagineGabriel Ogun Statedavid ojNessuna valutazione finora
- 2010 STEPS Report BangladeshDocumento176 pagine2010 STEPS Report Bangladeshfatehatun noorNessuna valutazione finora
- Airline Ground Safety Panel: Toolbox TalkDocumento3 pagineAirline Ground Safety Panel: Toolbox TalkRohit SinghNessuna valutazione finora
- Heart PathologyDocumento8 pagineHeart PathologyJose SirittNessuna valutazione finora
- Health FairDocumento11 pagineHealth FairThe Lima NewsNessuna valutazione finora
- Lymphoma of The StomachDocumento21 pagineLymphoma of The Stomachapi-19641337Nessuna valutazione finora
- Cocaine and Other Sympathomimetics PDFDocumento11 pagineCocaine and Other Sympathomimetics PDFLizeth GirónNessuna valutazione finora
- (Pittsburgh Pocket Psychiatry Series) Michael J Marcsisin, Jason B Rosenstock, Jessica M Gannon-Schizophrenia and Related Disorders-Oxford University Press (2017) PDFDocumento313 pagine(Pittsburgh Pocket Psychiatry Series) Michael J Marcsisin, Jason B Rosenstock, Jessica M Gannon-Schizophrenia and Related Disorders-Oxford University Press (2017) PDFToader AndreiNessuna valutazione finora
- Elstrott 2019Documento9 pagineElstrott 2019Aurha Akmal GinarisNessuna valutazione finora