Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 7 Lesson 7 DIET IN FEVERSDocumento14 pagine7 Lesson 7 DIET IN FEVERSBorolElemNessuna valutazione finora
- CA 2 - CHN Review 50 Items PretestDocumento10 pagineCA 2 - CHN Review 50 Items PretestAlibasher Macalnas100% (1)
- Treatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsDocumento65 pagineTreatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsLloyd Daniel BarrantesNessuna valutazione finora
- Contoh Penggunaan Intervensi Dalam Keperawatan KeluargaDocumento8 pagineContoh Penggunaan Intervensi Dalam Keperawatan KeluargaHimatul AliyahNessuna valutazione finora
- DafpusDocumento21 pagineDafpusDella Ayu PutriNessuna valutazione finora
- The Effect of Ramadan Fasting On Tuberculin Skin Test and Leukocyte Count Dalam Bhasa InggrisDocumento4 pagineThe Effect of Ramadan Fasting On Tuberculin Skin Test and Leukocyte Count Dalam Bhasa InggrisファラハンNessuna valutazione finora
- Okuda-Time Series Analysis of Under-Five MortalityDocumento61 pagineOkuda-Time Series Analysis of Under-Five MortalityBoniface Okuda100% (4)
- Baringo County SMART Survey Report - July 2019Documento61 pagineBaringo County SMART Survey Report - July 2019Artful Eyes ProductionsNessuna valutazione finora
- TuberkulozaDocumento2 pagineTuberkulozaDen HelfyNessuna valutazione finora
- Global Consultation of National Leprosy Programme Managers, Partners and Affected Persons On Global Leprosy Strategy 2021-2030Documento72 pagineGlobal Consultation of National Leprosy Programme Managers, Partners and Affected Persons On Global Leprosy Strategy 2021-2030سلوى بوشبيرقةNessuna valutazione finora
- Kristia Carpio Pulmonary TuberculosisDocumento31 pagineKristia Carpio Pulmonary TuberculosiskisNessuna valutazione finora
- Saida, Syamsiar : Volume 7 Nomor 1 Bulan Oktober 2019 EISSN: 2443-0218Documento9 pagineSaida, Syamsiar : Volume 7 Nomor 1 Bulan Oktober 2019 EISSN: 2443-0218neno fitriyani hasbieNessuna valutazione finora
- Adominal TBDocumento50 pagineAdominal TBTamjid KhanNessuna valutazione finora
- 3rd Reading ExamDocumento4 pagine3rd Reading Examjerielseguido-1Nessuna valutazione finora
- ICD-10 CM All Diagnosis and Trigger Codes - Revised 9-17-2015Documento6.507 pagineICD-10 CM All Diagnosis and Trigger Codes - Revised 9-17-2015Puskesmas MakaleNessuna valutazione finora
- Meningitis TBDocumento6 pagineMeningitis TBGarrett SimpsonNessuna valutazione finora
- PASSMEDICINE MCQs-RESPIRATORY MEDICINEDocumento111 paginePASSMEDICINE MCQs-RESPIRATORY MEDICINEHashim Ahmad75% (4)
- Marrow UpdatesDocumento9 pagineMarrow UpdatesVirat KohliNessuna valutazione finora
- The Challenge of Tuberculosis and Diabetes Mellitus ComorbidityDocumento23 pagineThe Challenge of Tuberculosis and Diabetes Mellitus ComorbidityHendra AryawinataNessuna valutazione finora
- Feed Ig MCCIDocumento5 pagineFeed Ig MCCIayuhati siregarNessuna valutazione finora
- Second Edition, 2017: Untold Stories of CourageDocumento32 pagineSecond Edition, 2017: Untold Stories of CouragenandumallidiNessuna valutazione finora
- Silo - Tips - Boardworks Gcse Science Biology Infections and ImmunityDocumento41 pagineSilo - Tips - Boardworks Gcse Science Biology Infections and ImmunityqrqrNessuna valutazione finora
- Salient Features of National Health Policy 2017Documento7 pagineSalient Features of National Health Policy 2017rajsandhu25Nessuna valutazione finora
- Att Reintroduction Nhs FlowchartDocumento6 pagineAtt Reintroduction Nhs FlowchartNitesh Gupta100% (1)
- Chrysalis Crack BookletDocumento9 pagineChrysalis Crack BookletHhhNessuna valutazione finora
- New Employee Medical QuestionnaireDocumento2 pagineNew Employee Medical QuestionnaireRichard R M ThodéNessuna valutazione finora
- Journal of Nutrition College,: Online Di: Http://ejournal3.undip - Ac.id/index - PHP/JNCDocumento11 pagineJournal of Nutrition College,: Online Di: Http://ejournal3.undip - Ac.id/index - PHP/JNCannisa dian zizianiNessuna valutazione finora
- RNTCP Guidelines Presentation, Gujarat, IndiaDocumento22 pagineRNTCP Guidelines Presentation, Gujarat, IndiaDhaval BhawaniNessuna valutazione finora
- TUBERCULOSISDocumento16 pagineTUBERCULOSISTonia Noor NajmNessuna valutazione finora
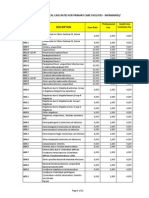
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocumento22 paginePhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNessuna valutazione finora