Potrebbero piacerti anche
- PostpartumDocumento32 paginePostpartumClaire Moraleta100% (1)
- Preeclampsia FinalDocumento112 paginePreeclampsia FinalEarl John DayanghirangNessuna valutazione finora
- 1.female Reproductive System PDFDocumento21 pagine1.female Reproductive System PDFTrang KhúcNessuna valutazione finora
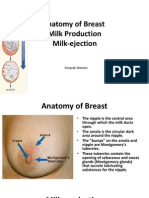
- Anatomy of Breast, Milk Production, and Milk-EjectionDocumento23 pagineAnatomy of Breast, Milk Production, and Milk-EjectionDeepak Ghimire100% (2)
- Abnormal Uterine BleedingDocumento4 pagineAbnormal Uterine BleedingAmellyn Reyes0% (1)
- Case Presentation: Placenta Previa: Crissa Marie D. PinedaDocumento42 pagineCase Presentation: Placenta Previa: Crissa Marie D. PinedaCrissa PinedaNessuna valutazione finora
- Case Study (Aub)Documento16 pagineCase Study (Aub)Lucila Lugo0% (2)
- PNLE Maternal and Child Health Nursing Exam - Reviewer PDFDocumento29 paginePNLE Maternal and Child Health Nursing Exam - Reviewer PDFSheng DekitNessuna valutazione finora
- Case Study - NSVD ScribdDocumento20 pagineCase Study - NSVD ScribdShar EnriquezNessuna valutazione finora
- GDM Case PresentationDocumento20 pagineGDM Case PresentationATEHAN BORDS100% (1)
- PediatricDocumento55 paginePediatricJade Q Osit100% (6)
- Anatomy and Physiology of The BreastDocumento4 pagineAnatomy and Physiology of The BreastRahmanNessuna valutazione finora
- Growth and Development Case Study grp1Documento7 pagineGrowth and Development Case Study grp1sleep whatNessuna valutazione finora
- Case Study-Ectopic PNDocumento55 pagineCase Study-Ectopic PNArbie Jacinto100% (2)
- AVENT Breastfeeding Online Guidebook2018Documento60 pagineAVENT Breastfeeding Online Guidebook2018indikapereraNessuna valutazione finora
- Gestational HypertensionDocumento71 pagineGestational HypertensionDevikha PeremelNessuna valutazione finora
- Gest. HTN C. StudyDocumento51 pagineGest. HTN C. StudyshangheartsyewNessuna valutazione finora
- Undescended TestisDocumento25 pagineUndescended TestisAmir ShafiqNessuna valutazione finora
- Case Study - PostpartumDocumento3 pagineCase Study - PostpartumLouel VicitacionNessuna valutazione finora
- Problem Solution Unwanted Pregnancy - Student ExampleDocumento4 pagineProblem Solution Unwanted Pregnancy - Student ExampleFlávia FermonNessuna valutazione finora
- Case Study Ob WardDocumento41 pagineCase Study Ob WardIan Mizzel A. Dulfina0% (2)
- Nursing Care of A Family During Labor and BirthDocumento19 pagineNursing Care of A Family During Labor and BirthPbNessuna valutazione finora
- Severe PreeclampsiaDocumento84 pagineSevere PreeclampsiaJm Bernardo50% (2)
- Case Study NSVDDocumento25 pagineCase Study NSVDLanju FerminNessuna valutazione finora
- Postpartum Hemorrhage: A.Personal DataDocumento55 paginePostpartum Hemorrhage: A.Personal DataEmmanuel Recodo100% (1)
- Normal Puerperium PDFDocumento22 pagineNormal Puerperium PDFwawa3385100% (1)
- The Royal Pentagon Review Specialist Inc. Pediatric NursingDocumento55 pagineThe Royal Pentagon Review Specialist Inc. Pediatric NursingDavid PunzalanNessuna valutazione finora
- Puerperium and Its Management 1Documento35 paginePuerperium and Its Management 1Elvis100% (2)
- A Case Study of Patient With Com Minuted Fracture Distal Third FemurDocumento70 pagineA Case Study of Patient With Com Minuted Fracture Distal Third FemurJellou Mac50% (8)
- Case Study Pre-EclampsiaDocumento51 pagineCase Study Pre-EclampsiaRomelle Jane M. VelascoNessuna valutazione finora
- Uterine ProlapseDocumento21 pagineUterine ProlapseFau Fau DheoboNessuna valutazione finora
- NSG 700 - Organ TranspantDocumento30 pagineNSG 700 - Organ TranspantJellou MacNessuna valutazione finora
- Case Study BMC-Surgical WardDocumento55 pagineCase Study BMC-Surgical WardVirgilio Reyes ManuelNessuna valutazione finora
- Foundation For Maternal and Child Health NursingDocumento18 pagineFoundation For Maternal and Child Health NursingChari RivoNessuna valutazione finora
- PUERPERIUMDocumento58 paginePUERPERIUMPencenk Azznew100% (4)
- Engorgement Post Partum: Merry C.ODocumento12 pagineEngorgement Post Partum: Merry C.OmerycoNessuna valutazione finora
- Background and Rationale of The StudyDocumento27 pagineBackground and Rationale of The StudyJellou MacNessuna valutazione finora
- New Case of Pre-EclampsiaDocumento13 pagineNew Case of Pre-EclampsiaKristine AlejandroNessuna valutazione finora
- PBLDocumento8 paginePBLJellou MacNessuna valutazione finora
- Gestational HTNDocumento6 pagineGestational HTNSim DimalantaNessuna valutazione finora
- Introduction To Reproductive HealthDocumento28 pagineIntroduction To Reproductive HealthpriyaNessuna valutazione finora
- My Case StudyDocumento17 pagineMy Case StudymaramNessuna valutazione finora
- The Nurse-Midwife and Crisis in A Home DeliveryDocumento2 pagineThe Nurse-Midwife and Crisis in A Home DeliverychoobiNessuna valutazione finora
- Partograph ExercisesDocumento2 paginePartograph ExercisesrlinaoNessuna valutazione finora
- Case Study in ObwardDocumento6 pagineCase Study in Obwardcharles_florendo25100% (3)
- Final Case Study SLDocumento17 pagineFinal Case Study SLCharmie Mei Paredes-RoqueNessuna valutazione finora
- Group 2. Ectopic PregnancyDocumento61 pagineGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
- Normal Spontaneous DeliveryDocumento1 paginaNormal Spontaneous DeliveryGi GiNessuna valutazione finora
- VacuumDocumento22 pagineVacuumRed WilliamsNessuna valutazione finora
- Case Study MiscariageDocumento14 pagineCase Study MiscariagesexiiimammaNessuna valutazione finora
- CHN Case Analysis Case ScenarioDocumento7 pagineCHN Case Analysis Case ScenarioNathalie kate petallarNessuna valutazione finora
- Case Study LTCSDocumento5 pagineCase Study LTCSKimNessuna valutazione finora
- MCN Case Study-2pDocumento76 pagineMCN Case Study-2pAngeline ShackletonNessuna valutazione finora
- Health Teaching PlanDocumento17 pagineHealth Teaching Planvictoria joy patauegNessuna valutazione finora
- Fetal DistressDocumento33 pagineFetal DistressYara H QaisiNessuna valutazione finora
- Nursing Care Plan (Post CS)Documento5 pagineNursing Care Plan (Post CS)Tony ReyesNessuna valutazione finora
- Evidence-Based Practice in Maternal & Child HealthDocumento15 pagineEvidence-Based Practice in Maternal & Child HealthJan Oliver YaresNessuna valutazione finora
- A Case of Cervical CancerDocumento24 pagineA Case of Cervical CancerDebbie beeNessuna valutazione finora
- Premature Rupture of MembraneDocumento66 paginePremature Rupture of MembranePriscilla Marie Macasaddug100% (1)
- Premature RuptureDocumento30 paginePremature RuptureSanthosh.S.U100% (1)
- Roxipan (Oxytocin) - Drug StudyDocumento4 pagineRoxipan (Oxytocin) - Drug StudyIzza DeloriaNessuna valutazione finora
- NSDDocumento44 pagineNSDabyssodeep100% (1)
- Vaginal Bleeding in Pregnancy - Teaching Care PlanDocumento3 pagineVaginal Bleeding in Pregnancy - Teaching Care PlannajmulNessuna valutazione finora
- PREECLAMPSIA Case ScenarioDocumento2 paginePREECLAMPSIA Case Scenariosabao kizuiteNessuna valutazione finora
- Case Study 2Documento19 pagineCase Study 2Sumit Singh100% (1)
- Drug Study For PreeclampsiaDocumento6 pagineDrug Study For PreeclampsiaLarah Mae AndogNessuna valutazione finora
- Prelim Examination MaternalDocumento23 paginePrelim Examination MaternalAaron ConstantinoNessuna valutazione finora
- Gestational Diabetes MellitusDocumento25 pagineGestational Diabetes MellitusMazlina MaidinNessuna valutazione finora
- SIM - Anemias of PregnancyDocumento17 pagineSIM - Anemias of PregnancyGabrielle EvangelistaNessuna valutazione finora
- Myoma Final Power PointDocumento45 pagineMyoma Final Power Pointicesexy100% (1)
- Nicu ReportDocumento18 pagineNicu ReportKabita KarakNessuna valutazione finora
- UTERINE PROLAPSE - Case ReportDocumento3 pagineUTERINE PROLAPSE - Case ReportIOSRjournalNessuna valutazione finora
- Final SDL 1Documento21 pagineFinal SDL 1Cy PilapilNessuna valutazione finora
- GORDONSDocumento4 pagineGORDONSInah Krizia LagueNessuna valutazione finora
- GH Case StudyDocumento14 pagineGH Case StudyHafza MacabatoNessuna valutazione finora
- ReferencesDocumento5 pagineReferencesJellou MacNessuna valutazione finora
- University of Immaculate Conception (CRF)Documento2 pagineUniversity of Immaculate Conception (CRF)Jellou MacNessuna valutazione finora
- Chapter VDocumento15 pagineChapter VJellou MacNessuna valutazione finora
- Table of Specifications: Subject: NAME OF TEACHER: - Degree Program: Academic Level: Sy SemesterDocumento2 pagineTable of Specifications: Subject: NAME OF TEACHER: - Degree Program: Academic Level: Sy SemesterJellou MacNessuna valutazione finora
- Major or Scrub, Circu PRC - VSMMC, CCMC, MaternityDocumento6 pagineMajor or Scrub, Circu PRC - VSMMC, CCMC, MaternityJellou MacNessuna valutazione finora
- Jera GDocumento4 pagineJera GJellou MacNessuna valutazione finora
- Intraoperative SOAPIEDocumento5 pagineIntraoperative SOAPIEJellou MacNessuna valutazione finora
- HysterectomyDocumento2 pagineHysterectomyJellou MacNessuna valutazione finora
- Puerperium and AnalgesiaDocumento12 paginePuerperium and AnalgesiaKim RamosNessuna valutazione finora
- Health and Nutritional Status of Certain Lactating Mothers of Bahawalpur, PakistanDocumento7 pagineHealth and Nutritional Status of Certain Lactating Mothers of Bahawalpur, PakistanDr Sharique AliNessuna valutazione finora
- HND 403 - Nutrition During LactationDocumento23 pagineHND 403 - Nutrition During LactationDanish KhanNessuna valutazione finora
- 2021 Promoting Human Milk and Breastfeeding For The Very Low Birth Weight InfantDocumento15 pagine2021 Promoting Human Milk and Breastfeeding For The Very Low Birth Weight InfantIlda IldaNessuna valutazione finora
- Factors Responsible For Lactation Failure Among MothersDocumento5 pagineFactors Responsible For Lactation Failure Among MothersVinay Kumar NandimallaNessuna valutazione finora
- NDT Midterms TransesDocumento30 pagineNDT Midterms TransesAleah JayaganNessuna valutazione finora
- Breast Feeding & Weaning: Supervisor DR: Hamsa Reda. Prepared By: GroupDocumento19 pagineBreast Feeding & Weaning: Supervisor DR: Hamsa Reda. Prepared By: GroupAhmed SanadNessuna valutazione finora
- SynopsisDocumento6 pagineSynopsisIsha NisarNessuna valutazione finora
- ANHP 00221 Dairy Technology Full NotesDocumento57 pagineANHP 00221 Dairy Technology Full NotesMachira MuturiNessuna valutazione finora
- 2nd Periodic TestDocumento2 pagine2nd Periodic TestJaymarNessuna valutazione finora
- Penerapan Hypnobreastfeeding Pada Ibu MenyusuiDocumento6 paginePenerapan Hypnobreastfeeding Pada Ibu MenyusuiKhotim SholehaNessuna valutazione finora
- MCN FinalsDocumento57 pagineMCN FinalsJudy BaguiwenNessuna valutazione finora
- LactationDocumento12 pagineLactationShafaqet KamalNessuna valutazione finora
- Nutrition Through The Life Cycle 6th Edition Brown Solutions ManualDocumento11 pagineNutrition Through The Life Cycle 6th Edition Brown Solutions Manualrobertadelatkmu100% (28)
- Presentation On BreastfeedindDocumento58 paginePresentation On Breastfeedindcharanjit kaurNessuna valutazione finora
- Physiology of Lactation and PurpuriumDocumento37 paginePhysiology of Lactation and Purpuriumvarshasharma05Nessuna valutazione finora
- Metoclopramide - Drugs and Lactation Database (LactMed®) - NCBI BookshelfDocumento1 paginaMetoclopramide - Drugs and Lactation Database (LactMed®) - NCBI BookshelfT. SaritaNessuna valutazione finora
- Moringa Breastfeeding Study PDFDocumento4 pagineMoringa Breastfeeding Study PDFCisco Silva100% (1)