Potrebbero piacerti anche
- 6th Central Pay Commission Salary CalculatorDocumento15 pagine6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Department of Labor: Generalprovision 6 28 07Documento6 pagineDepartment of Labor: Generalprovision 6 28 07USA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Aces CPDocumento36 pagineDepartment of Labor: Aces CPUSA_DepartmentOfLabor100% (2)
- 6th Central Pay Commission Salary CalculatorDocumento15 pagine6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Department of Labor: YouthworkerDocumento1 paginaDepartment of Labor: YouthworkerUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Yr English GuideDocumento1 paginaDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: YouthRulesBrochureDocumento12 pagineDepartment of Labor: YouthRulesBrochureUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: 20040422 YouthrulesDocumento1 paginaDepartment of Labor: 20040422 YouthrulesUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Niosh Recs To Dol 050302Documento198 pagineDepartment of Labor: Niosh Recs To Dol 050302USA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: ln61003Documento2 pagineDepartment of Labor: ln61003USA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Niosh Letter FinalDocumento3 pagineDepartment of Labor: Niosh Letter FinalUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: JYMP 11x17 3Documento1 paginaDepartment of Labor: JYMP 11x17 3USA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Final ReportDocumento37 pagineDepartment of Labor: Final ReportUSA_DepartmentOfLaborNessuna valutazione finora
- Department of Labor: Yr English GuideDocumento1 paginaDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Saili English TranslationDocumento2 pagineSaili English TranslationKaucha WorkNessuna valutazione finora
- Ethics CaseDocumento3 pagineEthics CaseButch MaatNessuna valutazione finora
- KUSOW Abdi M. & ENO Mohamed A. - Racial and Caste Prejudice in SomaliaDocumento30 pagineKUSOW Abdi M. & ENO Mohamed A. - Racial and Caste Prejudice in SomaliazahramineNessuna valutazione finora
- Indeed Malawian Songs Aimed at Demeaning Females in SocietyDocumento2 pagineIndeed Malawian Songs Aimed at Demeaning Females in Societyfrances chisiNessuna valutazione finora
- The Great Game in AsiaDocumento16 pagineThe Great Game in AsiadvxyzNessuna valutazione finora
- Defendant's MemorandumDocumento17 pagineDefendant's MemorandumAntonio de VeraNessuna valutazione finora
- Kenya's Physical and Land Use Planning Act 2019Documento67 pagineKenya's Physical and Land Use Planning Act 2019Sahil KhadkaNessuna valutazione finora
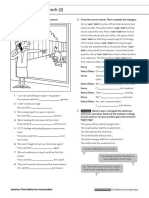
- 8D Reported Speech 2 1-1Documento1 pagina8D Reported Speech 2 1-1oputina rmNessuna valutazione finora
- G.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALDocumento20 pagineG.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALLucy HeartfiliaNessuna valutazione finora
- 218816-2018-Asia Pacific Resources InternationalDocumento11 pagine218816-2018-Asia Pacific Resources Internationalf919Nessuna valutazione finora
- JDCI Removed PortionsDocumento8 pagineJDCI Removed PortionscriminologyallianceNessuna valutazione finora
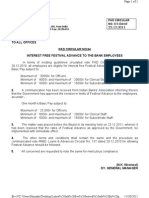
- Latest Circular For Payment of Interest Free Festival Advance To StaffDocumento1 paginaLatest Circular For Payment of Interest Free Festival Advance To Staffhimadri_bhattacharjeNessuna valutazione finora
- TRF LTD Vs Energo Engineering Projects LTD 0307201SC20171807171045272COM952734Documento20 pagineTRF LTD Vs Energo Engineering Projects LTD 0307201SC20171807171045272COM952734Aman BajajNessuna valutazione finora
- Donya Pierce Lawsuit Against Velda CityDocumento40 pagineDonya Pierce Lawsuit Against Velda CityRyan J. ReillyNessuna valutazione finora
- Mea Member BenefitsDocumento14 pagineMea Member Benefitsapi-84334367Nessuna valutazione finora
- I-864W, Intending Immigrant's Affidavit of Support Exemption InstructionsDocumento2 pagineI-864W, Intending Immigrant's Affidavit of Support Exemption InstructionsVladimir AliendreNessuna valutazione finora
- 03 3 PDFDocumento82 pagine03 3 PDFHông HoaNessuna valutazione finora
- SST General Male List PDFDocumento320 pagineSST General Male List PDFNoman ShahNessuna valutazione finora
- Period 2 Modules 2-3, 2-4, 2-5 Cornell NotesDocumento6 paginePeriod 2 Modules 2-3, 2-4, 2-5 Cornell NotesRayan ChoudharyNessuna valutazione finora
- N. Chomsky-Controlled-Asset-Of-The-New-World-OrderDocumento16 pagineN. Chomsky-Controlled-Asset-Of-The-New-World-Orderolim owletNessuna valutazione finora
- Law and Poverty ProjectDocumento35 pagineLaw and Poverty ProjectSWETCHCHA MISKANessuna valutazione finora
- Alanis III v. Court of Appeals G.R. No. 216425, November 11, 2020 FactsDocumento2 pagineAlanis III v. Court of Appeals G.R. No. 216425, November 11, 2020 FactsTraining Office100% (2)
- The Child Act 2001Documento20 pagineThe Child Act 2001SaidatulnajwaNessuna valutazione finora
- Rule 111Documento27 pagineRule 111janbryle.cardenas.21Nessuna valutazione finora
- Chapter Ix - Test Techniques With Some Samples of Set of QuestionsDocumento7 pagineChapter Ix - Test Techniques With Some Samples of Set of QuestionsErica Marie Bagon100% (2)
- NAACP Lawsuit Against Wilmington PoliceDocumento27 pagineNAACP Lawsuit Against Wilmington PoliceCris BarrishNessuna valutazione finora
- Saklar NeroDocumento9 pagineSaklar NeroIsmi Ambar SariNessuna valutazione finora
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Documento1 paginaTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)sahil sachdevaNessuna valutazione finora
- 199 Wajeeha 2k18 LLBDocumento6 pagine199 Wajeeha 2k18 LLBWajeeha LakhoNessuna valutazione finora
- UCD81 Mark McGradyDocumento4 pagineUCD81 Mark McGradymark mcgradyNessuna valutazione finora