Potrebbero piacerti anche
- CRM in HospitalsDocumento5 pagineCRM in HospitalsSubramanya DgNessuna valutazione finora
- Gap Model WordDocumento3 pagineGap Model WordPARAM CLOTHINGNessuna valutazione finora
- Customer SatisfactionDocumento44 pagineCustomer SatisfactionEbrahim Khan100% (3)
- Customer Satisfaction in OPDDocumento44 pagineCustomer Satisfaction in OPDMudasir GulzarNessuna valutazione finora
- PATIENT CARE ISSUES AND MANAGEMENT ISSUESDocumento8 paginePATIENT CARE ISSUES AND MANAGEMENT ISSUESAnitha KarthikNessuna valutazione finora
- CBMEC - Operations Management - PreMidDocumento4 pagineCBMEC - Operations Management - PreMidjojie dadorNessuna valutazione finora
- Key Characteristics of Hospital ServicesDocumento4 pagineKey Characteristics of Hospital ServicesKrithiga MahendravarmanNessuna valutazione finora
- Lynne Maher Original Transcript FinalDocumento5 pagineLynne Maher Original Transcript Finalvinh vũNessuna valutazione finora
- Gibbs Reflective Journal SampleDocumento4 pagineGibbs Reflective Journal SampleCres Padua Quinzon100% (1)
- Final Paper Satisfaction 2015Documento18 pagineFinal Paper Satisfaction 2015Ananga ChakrabortyNessuna valutazione finora
- Nature and Characteristics of Services in HospitalsDocumento7 pagineNature and Characteristics of Services in HospitalsOun MuhammadNessuna valutazione finora
- Patient SatisfactionDocumento13 paginePatient Satisfactionchristyattumalil100% (2)
- Importance of Support ServicesDocumento5 pagineImportance of Support ServicesRockson Ohene AsanteNessuna valutazione finora
- Methods of Public RelationsDocumento3 pagineMethods of Public RelationsAnusha Verghese100% (2)
- Chetana's Self Financing Courses: Submitted To: ProfDocumento13 pagineChetana's Self Financing Courses: Submitted To: ProfAniket MoreNessuna valutazione finora
- Challenges in NursingDocumento4 pagineChallenges in NursingAnju PandeyNessuna valutazione finora
- SWOT AssignmentDocumento14 pagineSWOT AssignmentNur Farzana100% (1)
- Patient Satisfaction Key to Quality HealthcareDocumento8 paginePatient Satisfaction Key to Quality HealthcareAjlan AliNessuna valutazione finora
- PSIP 7 Test SubmissionsDocumento7 paginePSIP 7 Test SubmissionsNCPQSWNessuna valutazione finora
- Improving Quality Health Care in The Hospitals NetDocumento2 pagineImproving Quality Health Care in The Hospitals Nettummalapalli venkateswara raoNessuna valutazione finora
- Dealing With Professional MisconductDocumento12 pagineDealing With Professional MisconductArlene MarasiganNessuna valutazione finora
- Patient Experience: What Does This Mean? - Beyond Philosophy ConsultancyDocumento15 paginePatient Experience: What Does This Mean? - Beyond Philosophy ConsultancyBeyond PhilosophyNessuna valutazione finora
- Chapter 1Documento7 pagineChapter 1Sharon BactatNessuna valutazione finora
- A Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraDocumento9 pagineA Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraVital TejaNessuna valutazione finora
- NCM 107Documento7 pagineNCM 107Jose Jumamoy100% (1)
- Medical Assitant ProjectDocumento18 pagineMedical Assitant Projectapi-378167354100% (1)
- Improving Quality of Care at Sunlight HospitalDocumento7 pagineImproving Quality of Care at Sunlight HospitalTooba SiddiquiNessuna valutazione finora
- Chapter 1,2 Impact of Hospital Services On Outpatient SatisfactionDocumento31 pagineChapter 1,2 Impact of Hospital Services On Outpatient SatisfactionHaseeb AhmedNessuna valutazione finora
- Patient Care Technician Cover LetterDocumento7 paginePatient Care Technician Cover Lettere76qy0tk100% (1)
- The Role of the Charge NurseDocumento25 pagineThe Role of the Charge NurseAlan George BevanNessuna valutazione finora
- Quality and HospitalDocumento6 pagineQuality and HospitalKuldeep BajajNessuna valutazione finora
- Patient Friendly Standards For AHPIDocumento26 paginePatient Friendly Standards For AHPIdrruchiNessuna valutazione finora
- SBARDocumento4 pagineSBARAhmad Safi'i Bin SamirinNessuna valutazione finora
- 7 Ps of Marketing For HospitalsDocumento3 pagine7 Ps of Marketing For HospitalsAnil Kumar Singh0% (1)
- Case Study - Patient ExperienceDocumento4 pagineCase Study - Patient ExperienceSusi RahmawatiNessuna valutazione finora
- Caring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Documento7 pagineCaring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Ryrey Abraham PacamanaNessuna valutazione finora
- ResponsibiltyDocumento12 pagineResponsibiltyhnasdbsywnyNessuna valutazione finora
- Case StudyDocumento2 pagineCase StudyKelvin NziokiNessuna valutazione finora
- Joshua Ofori EssiamDocumento9 pagineJoshua Ofori EssiamOfori EssiamNessuna valutazione finora
- Quality and Synthesis PaperDocumento6 pagineQuality and Synthesis Paperapi-253093073Nessuna valutazione finora
- Patient Satisfaction Survey ResultsDocumento57 paginePatient Satisfaction Survey ResultsrhinesafitriNessuna valutazione finora
- 260-Elder AbuseDocumento6 pagine260-Elder Abuseapi-283974740Nessuna valutazione finora
- Marketing Hospital IIPMDocumento108 pagineMarketing Hospital IIPMAnil Kumar SinghNessuna valutazione finora
- Ethics With Respect T The Helathcare WebsiteDocumento6 pagineEthics With Respect T The Helathcare Websiteih1989Nessuna valutazione finora
- Complaint HandlingDocumento15 pagineComplaint HandlingjarodzeeNessuna valutazione finora
- Research Paper Delegation in NursingDocumento6 pagineResearch Paper Delegation in Nursingafeavbrpd100% (1)
- Hospital Marketing MixDocumento6 pagineHospital Marketing MixJigar ShahNessuna valutazione finora
- Bioethics Article AnalysisssssDocumento5 pagineBioethics Article AnalysisssssKyle AndrewNessuna valutazione finora
- Give 2 Examples of Old Standards in Nursing Which Are Also Related To Customer Service?Documento2 pagineGive 2 Examples of Old Standards in Nursing Which Are Also Related To Customer Service?Bien EstrellaNessuna valutazione finora
- Running Head: Professional Development Assignment 1Documento12 pagineRunning Head: Professional Development Assignment 1api-396212664Nessuna valutazione finora
- Patient Relationship Management As ConsequenceDocumento8 paginePatient Relationship Management As ConsequenceAnil GowdaNessuna valutazione finora
- Servuction Model Explained in 40 CharactersDocumento4 pagineServuction Model Explained in 40 Charactersrajendrakumar33% (3)
- Effect of Customer Experience in Relation To Organizational PerformanceDocumento20 pagineEffect of Customer Experience in Relation To Organizational Performancereuben kipchumbaNessuna valutazione finora
- Customer Perception Towards Private HospitalsDocumento29 pagineCustomer Perception Towards Private HospitalsBilal Ah Parray90% (10)
- Hospital RelationshipDocumento14 pagineHospital RelationshipprofjthiruNessuna valutazione finora
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayDa EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNessuna valutazione finora
- Textbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosDa EverandTextbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosNessuna valutazione finora
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareDa EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNessuna valutazione finora
- Hidden Hospital Hazards: Saving Lives and Improving MarginsDa EverandHidden Hospital Hazards: Saving Lives and Improving MarginsNessuna valutazione finora
- PTE Writing Mock Test 2Documento24 paginePTE Writing Mock Test 2Abhishek Puri100% (1)
- PTE Speaking Mock Test 1 PDFDocumento49 paginePTE Speaking Mock Test 1 PDFAbhishek PuriNessuna valutazione finora
- PTE Speaking Mock Test 2 PDFDocumento49 paginePTE Speaking Mock Test 2 PDFAbhishek PuriNessuna valutazione finora
- Linkers 1Documento3 pagineLinkers 1Antonio M. ScielzoNessuna valutazione finora
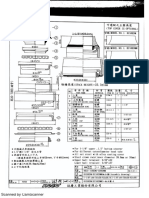
- 159EDM-159EDMM 組合圖Documento1 pagina159EDM-159EDMM 組合圖Abhishek PuriNessuna valutazione finora
- PTE Speaking Mock Test 2 PDFDocumento49 paginePTE Speaking Mock Test 2 PDFAbhishek PuriNessuna valutazione finora
- PTE Writing Mock Test 1Documento10 paginePTE Writing Mock Test 1Abhishek PuriNessuna valutazione finora
- Speaking Describe Image: Telegram Link: Mobile App LinkDocumento5 pagineSpeaking Describe Image: Telegram Link: Mobile App LinkyouvsyouNessuna valutazione finora
- PTE Writing Mock Test 2 PDFDocumento10 paginePTE Writing Mock Test 2 PDFAbhishek PuriNessuna valutazione finora
- PTE Writing Mock Test 2 PDFDocumento10 paginePTE Writing Mock Test 2 PDFAbhishek PuriNessuna valutazione finora
- Official Guide PTEA Teacher NotesDocumento249 pagineOfficial Guide PTEA Teacher NotesIqbal singh95% (20)
- Retell TemplateDocumento1 paginaRetell TemplateAbhishek PuriNessuna valutazione finora
- Production or Plant Engineer JobsDocumento4 pagineProduction or Plant Engineer JobsLoga NathanNessuna valutazione finora
- INCO Terms 2016 - Skyways Management Services LTDDocumento9 pagineINCO Terms 2016 - Skyways Management Services LTDAbhishek PuriNessuna valutazione finora
- China "EPA" Crackdown Shuts Down Tens of Thousands of Factories With No End in SightDocumento9 pagineChina "EPA" Crackdown Shuts Down Tens of Thousands of Factories With No End in SightAbhishek PuriNessuna valutazione finora
- 2013 Valuation OlympiadDocumento4 pagine2013 Valuation OlympiadAbhishek Puri0% (1)
- Radio Frequency IdentificationDocumento18 pagineRadio Frequency IdentificationAbhishek PuriNessuna valutazione finora
- Beginners Guide To ImportingDocumento3 pagineBeginners Guide To ImportingAbhishek PuriNessuna valutazione finora
- Assessing Changes in The Monetary Transmission Mechanism: A VAR ApproachDocumento15 pagineAssessing Changes in The Monetary Transmission Mechanism: A VAR ApproachAbhishek PuriNessuna valutazione finora
- Beginners Guide To ImportingDocumento27 pagineBeginners Guide To ImportingFarhanNessuna valutazione finora
- Production or Plant Engineer JobsDocumento4 pagineProduction or Plant Engineer JobsLoga NathanNessuna valutazione finora
- Beginners Guide To ImportingDocumento3 pagineBeginners Guide To ImportingAbhishek PuriNessuna valutazione finora
- Ontario Express Entry Guide 2018Documento64 pagineOntario Express Entry Guide 2018Anil rajputNessuna valutazione finora
- 7 Eleven 140613174951 Phpapp02Documento21 pagine7 Eleven 140613174951 Phpapp02Abhishek PuriNessuna valutazione finora
- Member RegistrationDocumento2 pagineMember Registrationasknishan0% (1)
- Logistic Regression (With R) : 1 TheoryDocumento15 pagineLogistic Regression (With R) : 1 TheoryrattonxNessuna valutazione finora
- Moving With The Technology: Time and Cost Savings, IncludingDocumento2 pagineMoving With The Technology: Time and Cost Savings, IncludingAbhishek PuriNessuna valutazione finora
- 2013 11 10 Repurchase Market TimingDocumento37 pagine2013 11 10 Repurchase Market TimingAbhishek PuriNessuna valutazione finora
- Making Credit Safer: The Case For RegulationDocumento5 pagineMaking Credit Safer: The Case For RegulationAbhishek PuriNessuna valutazione finora
- A Study On Ti CkhyclesDocumento25 pagineA Study On Ti CkhyclesAbhishek PuriNessuna valutazione finora
- Hospital Information SystemsDocumento32 pagineHospital Information SystemsabhiramghadaiNessuna valutazione finora
- ACER Report On The Implementation of The Balancing Network CodeDocumento144 pagineACER Report On The Implementation of The Balancing Network CodePasquale CutriNessuna valutazione finora
- Ipcrf EpsDocumento50 pagineIpcrf Epsrahimson100% (1)
- Thesis Template (Numbered)Documento29 pagineThesis Template (Numbered)michaelurielNessuna valutazione finora
- Policy Paper GuidelineDocumento3 paginePolicy Paper GuidelineLynn ThetNessuna valutazione finora
- Construction Management (CE754) : Ramesh Banstola 1Documento41 pagineConstruction Management (CE754) : Ramesh Banstola 1Naresh JirelNessuna valutazione finora
- Guidance Notes - 05 - Member CEngDocumento14 pagineGuidance Notes - 05 - Member CEngDavide BoreanezeNessuna valutazione finora
- CIVL 1101 Problem Solving ChapterDocumento9 pagineCIVL 1101 Problem Solving ChapterZenPhiNessuna valutazione finora
- NSTP 456Documento19 pagineNSTP 456Sarahjane TerradoNessuna valutazione finora
- Gmac RCDocumento16 pagineGmac RCDebasish SarangiNessuna valutazione finora
- A Guide To Producing Coursework: Oxford University Continuing EducationDocumento12 pagineA Guide To Producing Coursework: Oxford University Continuing EducationbogarguzNessuna valutazione finora
- EMGT101 PinoyBixDocumento12 pagineEMGT101 PinoyBixAllen Dela CruzNessuna valutazione finora
- MTP Micro Turn Proudtcs Apqp Timing Plan: S.No Description Resp. Status W1 W2Documento9 pagineMTP Micro Turn Proudtcs Apqp Timing Plan: S.No Description Resp. Status W1 W2Sahil WadhwaNessuna valutazione finora
- Evaluating Assistive DevicesDocumento16 pagineEvaluating Assistive DevicesMilton R. GutierrezNessuna valutazione finora
- APQP4Wind E-Manual Version 1.2 - Partial PreviewDocumento12 pagineAPQP4Wind E-Manual Version 1.2 - Partial PreviewGüner Güvenç0% (1)
- Coaching Softball Technical - Tactical Skills PDFDocumento272 pagineCoaching Softball Technical - Tactical Skills PDFenergetiko15Nessuna valutazione finora
- Uganda Gender PolicyDocumento42 pagineUganda Gender PolicyTrent EdgarsNessuna valutazione finora
- Audit and Assurance Case Study Questions - ACCA Qualification - Students - ACCA GlobalDocumento4 pagineAudit and Assurance Case Study Questions - ACCA Qualification - Students - ACCA GlobalKelly Tan Xue LingNessuna valutazione finora
- Principles of Health AdminDocumento42 paginePrinciples of Health AdminAnne BattulayanNessuna valutazione finora
- Training Evaluation1Documento13 pagineTraining Evaluation1sirajuddin islamNessuna valutazione finora
- Guide To Pre Qualification DocumentsDocumento65 pagineGuide To Pre Qualification DocumentsAllen CochranNessuna valutazione finora
- Self-Evaluation Guide for Professional DevelopmentDocumento24 pagineSelf-Evaluation Guide for Professional DevelopmentJun CrisostomoNessuna valutazione finora
- Ul CalibrationrequirementsDocumento7 pagineUl CalibrationrequirementsAlexandre HesslerNessuna valutazione finora
- Competency MappingDocumento12 pagineCompetency Mappingarchana2089100% (1)
- Rijvan Hasan S Books CollectionDocumento1 paginaRijvan Hasan S Books CollectionSîronamHin MonirNessuna valutazione finora
- Comprehensive Analysis of Knowledge Management CyclesDocumento9 pagineComprehensive Analysis of Knowledge Management CyclesJoão Ricardo PeixotoNessuna valutazione finora
- Worcester Superintendent of Schools Melinda Boone's End-of-Cycle Summative EvaluationDocumento19 pagineWorcester Superintendent of Schools Melinda Boone's End-of-Cycle Summative EvaluationMegan BardNessuna valutazione finora
- Change Control in Pharma Supply ChainsDocumento12 pagineChange Control in Pharma Supply ChainsAhmed MagdyNessuna valutazione finora
- 10.1.1.72.7494Documento12 pagine10.1.1.72.7494Ivan Philip PerezNessuna valutazione finora
- Project Procurement and Contract Admin-1Documento16 pagineProject Procurement and Contract Admin-1Dereje LuleNessuna valutazione finora