Potrebbero piacerti anche
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Da EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Valutazione: 5 su 5 stelle5/5 (2)
- Goljan High Yield PharmaDocumento9 pagineGoljan High Yield Pharmahabdulhye100% (1)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessDa EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNessuna valutazione finora
- Micro Rapid ReviewDocumento6 pagineMicro Rapid ReviewEvan Miller100% (3)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionDa EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNessuna valutazione finora
- USMLE Step 1 EquationsDocumento1 paginaUSMLE Step 1 EquationsDina Nadeem100% (2)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Da EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Valutazione: 5 su 5 stelle5/5 (1)
- Usmle CluesDocumento86 pagineUsmle CluesAlejandro Bocanegra Osuna100% (8)
- Basic Science Quick Facts Step1Documento31 pagineBasic Science Quick Facts Step1Hannah Jackson100% (20)
- USMLE PathognomicsDocumento9 pagineUSMLE PathognomicsMatt McGlothlin94% (18)
- Pathoma Notes CH 1-3Documento11 paginePathoma Notes CH 1-3imdaking12392% (25)
- Usmle Smasher: A Smart Guide to Smash Usmle Clinical SkillsDa EverandUsmle Smasher: A Smart Guide to Smash Usmle Clinical SkillsNessuna valutazione finora
- USMLE Step 1 Radiology Buzzwords - USMLE ForumsDocumento5 pagineUSMLE Step 1 Radiology Buzzwords - USMLE Forumsfrabzi100% (2)
- Penicillins Pen&G Pen&V: T.%pallidum% (Syphilis)Documento1 paginaPenicillins Pen&G Pen&V: T.%pallidum% (Syphilis)gregoryvo100% (5)
- Dr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsDa EverandDr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsValutazione: 5 su 5 stelle5/5 (1)
- Step 1 HintsDocumento4 pagineStep 1 HintsKelvin Aquino GallozaNessuna valutazione finora
- U.S. MEDICAL LICENSING EXAM (USMLE) STEP I – Basic Medical Sciences: Passbooks Study GuideDa EverandU.S. MEDICAL LICENSING EXAM (USMLE) STEP I – Basic Medical Sciences: Passbooks Study GuideNessuna valutazione finora
- Essential Medical Concepts and TerminologyDocumento3 pagineEssential Medical Concepts and TerminologyMedStudent7650% (4)
- Goljan Path Review: Cell Injury, Inflammation, and Immune SystemDocumento57 pagineGoljan Path Review: Cell Injury, Inflammation, and Immune Systemnewmexicoomfs100% (5)
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionDa EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNessuna valutazione finora
- Pharmacology Usmle Step 1Documento5 paginePharmacology Usmle Step 1raj_1041100% (15)
- SURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.Da EverandSURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.Valutazione: 5 su 5 stelle5/5 (1)
- Super Recall EAQDocumento63 pagineSuper Recall EAQlourdeslulylou100% (27)
- 500 High Yield Nuggets Step 1Documento25 pagine500 High Yield Nuggets Step 1AmrAliTaha91% (22)
- USMLE Step 1: Integrated Vignettes: Must-know, high-yield reviewDa EverandUSMLE Step 1: Integrated Vignettes: Must-know, high-yield reviewValutazione: 4.5 su 5 stelle4.5/5 (7)
- USMLE Step 1 Board Exam High Yield Anatomy For MedicineDocumento7 pagineUSMLE Step 1 Board Exam High Yield Anatomy For Medicinesirp328100% (2)
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyDa EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyValutazione: 5 su 5 stelle5/5 (2)
- Pathoma Notes CH 1 3 PDFDocumento11 paginePathoma Notes CH 1 3 PDFAmanda Teaca67% (3)
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsDa EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsValutazione: 5 su 5 stelle5/5 (9)
- Step 1 USMLE NotesDocumento15 pagineStep 1 USMLE Notes13un391543100% (1)
- U.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideDa EverandU.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideNessuna valutazione finora
- DIT High Yield QuestionsDocumento13 pagineDIT High Yield Questionsdrcharleston100% (12)
- UWORLD Notes by Subject (Main Division) (Usmle Grassroots)Documento80 pagineUWORLD Notes by Subject (Main Division) (Usmle Grassroots)Mital Bhakta83% (18)
- Step 1 UworldDocumento25 pagineStep 1 UworldKarl Abiaad100% (23)
- USMLE Questions SummarizedDocumento85 pagineUSMLE Questions SummarizedJamesIwu89% (19)
- Microbiology Step 1 Weird Exceptions and DetailDocumento10 pagineMicrobiology Step 1 Weird Exceptions and DetailLucykesh100% (2)
- Pathoma NotesDocumento28 paginePathoma NotesHarun Rashid100% (4)
- Immunology High Yield For STEP 1Documento13 pagineImmunology High Yield For STEP 1Lucykesh100% (6)
- High Yield Step 1 FactsDocumento3 pagineHigh Yield Step 1 Factsadmitone01Nessuna valutazione finora
- Khan USMLE Pearls MicroDocumento8 pagineKhan USMLE Pearls Microlourdesfercab75% (4)
- USMLE STEP ! RAPID REVIEW NotesDocumento232 pagineUSMLE STEP ! RAPID REVIEW NotesSSGFL194% (18)
- Usmle Hy Images: By: MeduploaderDocumento62 pagineUsmle Hy Images: By: Meduploaderdamodarpatil100% (18)
- List of Forgettables - What You Need To Review Few Days Before The Exam - USMLE ForumsDocumento1 paginaList of Forgettables - What You Need To Review Few Days Before The Exam - USMLE ForumsJahanzeb AhmedNessuna valutazione finora
- High Yield Image Plates Gross - Patholog PDFDocumento151 pagineHigh Yield Image Plates Gross - Patholog PDFld100% (2)
- Nephritic Table USMLE Step 1Documento2 pagineNephritic Table USMLE Step 1Davin PersaudNessuna valutazione finora
- Goljan - Audio TranscriptsDocumento296 pagineGoljan - Audio TranscriptsGurbir Singh Gill90% (30)
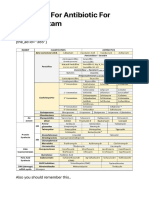
- Summary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study DataDocumento5 pagineSummary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study Dataomy yadavNessuna valutazione finora
- DirtyUSMLE RocksDocumento412 pagineDirtyUSMLE RocksDavid S. Chou90% (30)
- Behavioural Science Notes UsmleDocumento19 pagineBehavioural Science Notes UsmleLucykesh100% (3)
- UW Path NoteDocumento218 pagineUW Path NoteSophia Yin100% (4)
- Insulinoma and Hyperinsulinism GuideDocumento13 pagineInsulinoma and Hyperinsulinism Guideaileen agustinNessuna valutazione finora
- I. Answer The Following QuestionsDocumento9 pagineI. Answer The Following QuestionsFaheem MusthafaNessuna valutazione finora
- Trimbow-Fostair Combined Pi 78785Documento1 paginaTrimbow-Fostair Combined Pi 78785Shauna DunnNessuna valutazione finora
- Drugs Trade Mechanism Indications Kinetics Ci/Ae Hypothalamic-Anterior Pituitary AxisDocumento7 pagineDrugs Trade Mechanism Indications Kinetics Ci/Ae Hypothalamic-Anterior Pituitary Axisrmiller8456161Nessuna valutazione finora
- Ochem Assignment ChemistryDocumento6 pagineOchem Assignment Chemistrysplinter594Nessuna valutazione finora
- WBC Usmle QuestionsDocumento17 pagineWBC Usmle Questionssplinter594100% (1)
- Usmle ICM ReviewDocumento6 pagineUsmle ICM Reviewsplinter594Nessuna valutazione finora
- WBC Usmle QuestionsDocumento17 pagineWBC Usmle Questionssplinter594100% (1)
- UTP3-SW04-TP60 Datasheet VER2.0Documento2 pagineUTP3-SW04-TP60 Datasheet VER2.0Ricardo TitoNessuna valutazione finora
- NewspaperDocumento11 pagineNewspaperКристина ОрёлNessuna valutazione finora
- Guiding Childrens Social Development and Learning 8th Edition Kostelnik Test BankDocumento16 pagineGuiding Childrens Social Development and Learning 8th Edition Kostelnik Test Bankoglepogy5kobgk100% (27)
- Insider Threat ManagementDocumento48 pagineInsider Threat ManagementPatricia LehmanNessuna valutazione finora
- Polytechnic University Management Services ExamDocumento16 paginePolytechnic University Management Services ExamBeverlene BatiNessuna valutazione finora
- The Berkeley Review: MCAT Chemistry Atomic Theory PracticeDocumento37 pagineThe Berkeley Review: MCAT Chemistry Atomic Theory Practicerenjade1516Nessuna valutazione finora
- Panel Data Econometrics: Manuel ArellanoDocumento5 paginePanel Data Econometrics: Manuel Arellanoeliasem2014Nessuna valutazione finora
- BIBLIO Eric SwyngedowDocumento34 pagineBIBLIO Eric Swyngedowadriank1975291Nessuna valutazione finora
- 3ccc PDFDocumento20 pagine3ccc PDFKaka KunNessuna valutazione finora
- Data Sheet: Experiment 5: Factors Affecting Reaction RateDocumento4 pagineData Sheet: Experiment 5: Factors Affecting Reaction Ratesmuyet lêNessuna valutazione finora
- Portfolio Artifact Entry Form - Ostp Standard 3Documento1 paginaPortfolio Artifact Entry Form - Ostp Standard 3api-253007574Nessuna valutazione finora
- Multiple Choice: CH142 Sample Exam 2 QuestionsDocumento12 pagineMultiple Choice: CH142 Sample Exam 2 QuestionsRiky GunawanNessuna valutazione finora
- Onan Service Manual MDJA MDJB MDJC MDJE MDJF Marine Diesel Genset Engines 974-0750Documento92 pagineOnan Service Manual MDJA MDJB MDJC MDJE MDJF Marine Diesel Genset Engines 974-0750GreenMountainGenerators80% (10)
- تاااتتاااDocumento14 pagineتاااتتاااMegdam Sameeh TarawnehNessuna valutazione finora
- PRODUCTDocumento82 paginePRODUCTSrishti AggarwalNessuna valutazione finora
- "Behind The Times: A Look at America's Favorite Crossword," by Helene HovanecDocumento5 pagine"Behind The Times: A Look at America's Favorite Crossword," by Helene HovanecpspuzzlesNessuna valutazione finora
- MBO, Management by Objectives, Pooja Godiyal, Assistant ProfessorDocumento20 pagineMBO, Management by Objectives, Pooja Godiyal, Assistant ProfessorPooja GodiyalNessuna valutazione finora
- The Impact of School Facilities On The Learning EnvironmentDocumento174 pagineThe Impact of School Facilities On The Learning EnvironmentEnrry Sebastian71% (31)
- The European Journal of Applied Economics - Vol. 16 #2Documento180 pagineThe European Journal of Applied Economics - Vol. 16 #2Aleksandar MihajlovićNessuna valutazione finora
- Innovation Through Passion: Waterjet Cutting SystemsDocumento7 pagineInnovation Through Passion: Waterjet Cutting SystemsRomly MechNessuna valutazione finora
- India: Kerala Sustainable Urban Development Project (KSUDP)Documento28 pagineIndia: Kerala Sustainable Urban Development Project (KSUDP)ADBGADNessuna valutazione finora
- Current Diagnosis and Therapy For Head and Neck MalignanciesDocumento249 pagineCurrent Diagnosis and Therapy For Head and Neck MalignanciesMara TomaNessuna valutazione finora
- DELcraFT Works CleanEra ProjectDocumento31 pagineDELcraFT Works CleanEra Projectenrico_britaiNessuna valutazione finora
- Table of Specification for Pig Farming SkillsDocumento7 pagineTable of Specification for Pig Farming SkillsYeng YengNessuna valutazione finora
- Exercises2 SolutionsDocumento7 pagineExercises2 Solutionspedroagv08Nessuna valutazione finora
- PointerDocumento26 paginePointerpravin2mNessuna valutazione finora
- Polyol polyether+NCO Isupur PDFDocumento27 paginePolyol polyether+NCO Isupur PDFswapon kumar shillNessuna valutazione finora
- Maverick Brochure SMLDocumento16 pagineMaverick Brochure SMLmalaoui44Nessuna valutazione finora
- Family Service and Progress Record: Daughter SeptemberDocumento29 pagineFamily Service and Progress Record: Daughter SeptemberKathleen Kae Carmona TanNessuna valutazione finora
- FranklinDocumento4 pagineFranklinapi-291282463Nessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesDa EverandThe Ultimate Guide To Memory Improvement TechniquesValutazione: 5 su 5 stelle5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementDa EverandTechniques Exercises And Tricks For Memory ImprovementValutazione: 4.5 su 5 stelle4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNessuna valutazione finora
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 3.5 su 5 stelle3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 5 su 5 stelle5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDa EverandThe Happiness Trap: How to Stop Struggling and Start LivingValutazione: 4 su 5 stelle4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 5 su 5 stelle5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 3.5 su 5 stelle3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossDa EverandThe Tennis Partner: A Doctor's Story of Friendship and LossValutazione: 4.5 su 5 stelle4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDa EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisValutazione: 5 su 5 stelle5/5 (3)