Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Brachial PlexusDocumento62 pagineBrachial PlexusTutankhamoun Akhenatoun100% (2)
- Understanding Stroke-Brain Anatomy and Cerebral CirculationDocumento47 pagineUnderstanding Stroke-Brain Anatomy and Cerebral CirculationNaveen Eldose100% (4)
- Infantile, Childhood, and Adolescent Epilepsies.9Documento34 pagineInfantile, Childhood, and Adolescent Epilepsies.9Silviana IlieNessuna valutazione finora
- Checklist For All Loan TypesDocumento2 pagineChecklist For All Loan TypesSedaka DonaldsonNessuna valutazione finora
- Neurophysiology of PainDocumento32 pagineNeurophysiology of PainShivan A.C.Nessuna valutazione finora
- Bed Sore 48Documento45 pagineBed Sore 48Sedaka DonaldsonNessuna valutazione finora
- Wound Closure ManualDocumento127 pagineWound Closure ManualDougyStoffell100% (5)
- Ihbas ReportDocumento11 pagineIhbas ReportSeema YadavNessuna valutazione finora
- MCCQE 1 Scope of Questions - CDMDocumento11 pagineMCCQE 1 Scope of Questions - CDMmiadelfior100% (2)
- Stroke 1Documento35 pagineStroke 1Aisyah IcahNessuna valutazione finora
- Creutzfeldt-Jakob Disease 1Documento16 pagineCreutzfeldt-Jakob Disease 1anu1643Nessuna valutazione finora
- Barry E. Kosofsky, MD, PHD Adapted From Wayne Blount, MDDocumento34 pagineBarry E. Kosofsky, MD, PHD Adapted From Wayne Blount, MDSedaka DonaldsonNessuna valutazione finora
- International Observership HandbookDocumento51 pagineInternational Observership HandbookSedaka DonaldsonNessuna valutazione finora
- Fluids - Electrolytes ICU PDFDocumento91 pagineFluids - Electrolytes ICU PDFAhmed Shihab AhmedNessuna valutazione finora
- Gen Medicine - Finalized Scheme of ExaminationDocumento30 pagineGen Medicine - Finalized Scheme of Examinationsp_rao2000Nessuna valutazione finora
- Laryngeal Dystonia (Spasmodic Dysphonia) : SymptomsDocumento3 pagineLaryngeal Dystonia (Spasmodic Dysphonia) : SymptomschalixchassreenNessuna valutazione finora
- Imagenes Psicologia FisiologicaDocumento18 pagineImagenes Psicologia FisiologicaMayra VillegasNessuna valutazione finora
- Mithyantha2017 PDFDocumento7 pagineMithyantha2017 PDFRifki Sanjaya PratamaNessuna valutazione finora
- Different Types of Diseases/disorders of The Nervous System.Documento23 pagineDifferent Types of Diseases/disorders of The Nervous System.Saba Parvin Haque100% (4)
- 1 s2.0 S1474442222004318 MainDocumento15 pagine1 s2.0 S1474442222004318 MainItamar MeirelesNessuna valutazione finora
- Multiple Choice Questions For Part IVDocumento18 pagineMultiple Choice Questions For Part IVTarek MohsenNessuna valutazione finora
- Differential Diagnosis of Neurological Diseases ofDocumento25 pagineDifferential Diagnosis of Neurological Diseases ofRajesh kumarNessuna valutazione finora
- Epilepsy Syndromes in Children - UpToDateDocumento26 pagineEpilepsy Syndromes in Children - UpToDatecapt_zoeNessuna valutazione finora
- Journal of Neurology and NeurocienceDocumento49 pagineJournal of Neurology and NeurocienceInternational Medical PublisherNessuna valutazione finora
- TalkDocumento18 pagineTalkapi-338453738Nessuna valutazione finora
- Neuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityDocumento46 pagineNeuroradiology: Sony Sutrisno Department of Radiology Krida Wacana Christian UniversityPaulus AnungNessuna valutazione finora
- Clinical Examination and Management of Impairments in VariousDocumento34 pagineClinical Examination and Management of Impairments in Variousmukesh pokharelNessuna valutazione finora
- Case Study For AphasiaDocumento4 pagineCase Study For AphasiaYell Yint MyatNessuna valutazione finora
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocumento5 pagineChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaNessuna valutazione finora
- Simulation Questions Cooper MadisonDocumento2 pagineSimulation Questions Cooper MadisonJohn MixerNessuna valutazione finora
- Management of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHSDocumento8 pagineManagement of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHS彭金辉 KIVINessuna valutazione finora
- Management of Unconscious PatientDocumento51 pagineManagement of Unconscious PatientHylman Mahendra100% (1)
- Brain AbscessDocumento25 pagineBrain AbscessprembarnabasNessuna valutazione finora
- What Is A Brain Aneurysm?Documento2 pagineWhat Is A Brain Aneurysm?shinNessuna valutazione finora
- Bigler 2013 PDFDocumento41 pagineBigler 2013 PDFCarolina SalazarNessuna valutazione finora
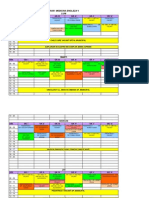
- Orar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViDocumento3 pagineOrar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViCornel MihaiNessuna valutazione finora