Potrebbero piacerti anche
- New and Emerging Entities in Dermatology and DermatopathologyDa EverandNew and Emerging Entities in Dermatology and DermatopathologyNessuna valutazione finora
- Diagnosing Leprosy: A Guide to the Cardinal SignsDocumento23 pagineDiagnosing Leprosy: A Guide to the Cardinal SignsbayoesunaryoNessuna valutazione finora
- TP LeprosyDocumento4 pagineTP LeprosyZarina RobledoNessuna valutazione finora
- Neurometabolic Hereditary Diseases of AdultsDa EverandNeurometabolic Hereditary Diseases of AdultsAlessandro P. BurlinaNessuna valutazione finora
- Thesis Jessica KattanDocumento45 pagineThesis Jessica Kattanaztigan100% (2)
- Tugas Ujian RioDocumento9 pagineTugas Ujian RioMaxend Arselino SilooyNessuna valutazione finora
- Leprosy JEADVDocumento9 pagineLeprosy JEADVAna BeatrizNessuna valutazione finora
- Diagnosis of Leprosy: Salvatore Noto and Pieter A M SchreuderDocumento10 pagineDiagnosis of Leprosy: Salvatore Noto and Pieter A M SchreuderMichelle HutahurukNessuna valutazione finora
- Leprosy Diagnosis and TreatmentDocumento7 pagineLeprosy Diagnosis and TreatmentEzra Manalansan-Beltran BaulNessuna valutazione finora
- Differential Diagnosis of LeprosyDocumento25 pagineDifferential Diagnosis of Leprosyma hNessuna valutazione finora
- What causes leprosy and its symptomsDocumento7 pagineWhat causes leprosy and its symptomsArron Buenavista AblogNessuna valutazione finora
- Refmh 9Documento10 pagineRefmh 9Anonymous S0MyRHNessuna valutazione finora
- Case Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisDocumento5 pagineCase Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisadibahtiarNessuna valutazione finora
- Lepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeDocumento2 pagineLepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeAstri MelistriNessuna valutazione finora
- Neurological Manifestations and Brain Disorders of Leprosy: Nazli Gamze BulbulDocumento3 pagineNeurological Manifestations and Brain Disorders of Leprosy: Nazli Gamze BulbulMia Shofianne LibertyNessuna valutazione finora
- Approach To Patients EULARDocumento35 pagineApproach To Patients EULARstuckinbedNessuna valutazione finora
- Jurnal KUSTADocumento10 pagineJurnal KUSTAzizee61Nessuna valutazione finora
- Dental Sealant ToxicityDocumento14 pagineDental Sealant ToxicityGuru SvamiNessuna valutazione finora
- Lupus Term PaperDocumento10 pagineLupus Term Paperc5qdk8jn100% (1)
- How To Evaluate A Case of LeprosyDocumento35 pagineHow To Evaluate A Case of LeprosyBarath Kumar SinghNessuna valutazione finora
- Lupus White BookDocumento60 pagineLupus White BookLisbeth MartínezNessuna valutazione finora
- The Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDDocumento9 pagineThe Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDmahmoud korieshNessuna valutazione finora
- 1793-Article Text-19545-2-10-20190508 PDFDocumento5 pagine1793-Article Text-19545-2-10-20190508 PDFRezkyRamadhaniSyarifNessuna valutazione finora
- LeprosyDocumento6 pagineLeprosyMaricel Y. LizadaNessuna valutazione finora
- Leprosy and Leprosy ProgramDocumento26 pagineLeprosy and Leprosy ProgramAnne LeeNessuna valutazione finora
- Scabies Clinical Manifestations and Diagnosis 2015 Polish Annals of MedicinDocumento4 pagineScabies Clinical Manifestations and Diagnosis 2015 Polish Annals of MedicinAbrahamisnanNessuna valutazione finora
- Diagnostic Strategy in RheumatologyDocumento25 pagineDiagnostic Strategy in Rheumatologyaa031987Nessuna valutazione finora
- International Workshop On Neuropathology in Leprosy - Consensus ReportDocumento18 pagineInternational Workshop On Neuropathology in Leprosy - Consensus ReportiisisiisNessuna valutazione finora
- Primary Neural Leprosy: Systematic Review: Hanseníase Neural Primária: Revisão SistemáticaDocumento8 paginePrimary Neural Leprosy: Systematic Review: Hanseníase Neural Primária: Revisão SistemáticaAjie WitamaNessuna valutazione finora
- MorgellonsDocumento3 pagineMorgellonsUul Parello OllaolloNessuna valutazione finora
- Lupus:: An Autoimmune DiseaseDocumento19 pagineLupus:: An Autoimmune DiseaseDan DanNessuna valutazione finora
- Jurnal Kulit 3Documento4 pagineJurnal Kulit 3yayan latuconsinaNessuna valutazione finora
- Case Leprosy-NewDocumento16 pagineCase Leprosy-NewChinta Nur SilmiNessuna valutazione finora
- Lupus Research Paper ThesisDocumento7 pagineLupus Research Paper Thesisgz8reqdc100% (1)
- European Guideline On Chronic PruritusDocumento20 pagineEuropean Guideline On Chronic PruritusBernardo Nascentes Bruno100% (1)
- Systemic Lupus Erythematosus SLEDocumento7 pagineSystemic Lupus Erythematosus SLEDjdjjd SiisusNessuna valutazione finora
- Morgellons Disease The Mystery Unfolds Virginia R Savely and Raphael B StrickerDocumento12 pagineMorgellons Disease The Mystery Unfolds Virginia R Savely and Raphael B Strickersisterrosetta100% (1)
- Psoriasis - Systemic DiseaseDocumento225 paginePsoriasis - Systemic DiseaseShengping LUONessuna valutazione finora
- Leprosy: M Leprae Is An Obligate Intracellular Acid-Fast Bacillus With A Unique Ability ToDocumento4 pagineLeprosy: M Leprae Is An Obligate Intracellular Acid-Fast Bacillus With A Unique Ability ToShine Reyes MackieNessuna valutazione finora
- Syphilis Recognition Description and DiagnosisDocumento138 pagineSyphilis Recognition Description and DiagnosisCelta Gómez TrejoNessuna valutazione finora
- Psoriasis Research PaperDocumento4 paginePsoriasis Research Papervvjrpsbnd100% (1)
- 1887 - 3147021-Pathophysiology and Management of Sensitive Skin - Position Paper From The Special Interest Group On Sensitive Skin of The International Forum For The Study of Itch (IFSI)Documento8 pagine1887 - 3147021-Pathophysiology and Management of Sensitive Skin - Position Paper From The Special Interest Group On Sensitive Skin of The International Forum For The Study of Itch (IFSI)chen peng feiNessuna valutazione finora
- Diagnosis Dan Penatalaksanaan Psoriasis Pada Orang Dewasa: Novella Ruana Fista Hamady 102014197 / C5Documento19 pagineDiagnosis Dan Penatalaksanaan Psoriasis Pada Orang Dewasa: Novella Ruana Fista Hamady 102014197 / C5vellahamadyNessuna valutazione finora
- tmpCE57 TMPDocumento1 paginatmpCE57 TMPFrontiersNessuna valutazione finora
- Acad Dermatol Venereol - 2020 - Misery - A Position Paper On The Management of Itch and Pain in Atopic Dermatitis From TheDocumento10 pagineAcad Dermatol Venereol - 2020 - Misery - A Position Paper On The Management of Itch and Pain in Atopic Dermatitis From Themaituuyen1997Nessuna valutazione finora
- Leprosy 22Documento49 pagineLeprosy 22Phc ChathannoorNessuna valutazione finora
- Thesis PsoriasisDocumento4 pagineThesis PsoriasisDereck Downing100% (2)
- Leprosy Written ReportDocumento7 pagineLeprosy Written Reportnicah05Nessuna valutazione finora
- Mycobacterial Diseases: Physical Disabilities in Leprosy: Some Contemporary Basic AspectsDocumento4 pagineMycobacterial Diseases: Physical Disabilities in Leprosy: Some Contemporary Basic AspectsAjie WitamaNessuna valutazione finora
- Color Atlas of Small Animal NecropsyDocumento76 pagineColor Atlas of Small Animal Necropsykritvet100% (3)
- Acad Dermatol Venereol - 2016 - Misery - Sensitive SkinDocumento7 pagineAcad Dermatol Venereol - 2016 - Misery - Sensitive SkinmochisrtNessuna valutazione finora
- A Case Study Presentation On Systemic Lupus Erythematosus - Group 1Documento34 pagineA Case Study Presentation On Systemic Lupus Erythematosus - Group 1KeepItSecret100% (2)
- Childhood Leprosy: Facts, Myths and Mysteries: Jayamini SeneviratneDocumento7 pagineChildhood Leprosy: Facts, Myths and Mysteries: Jayamini SeneviratneDhanasree VijayanNessuna valutazione finora
- Infectious Diseases: Leprosy Case Series in The Emergency Room: A Warning Sign For A Challenging DiagnosisDocumento5 pagineInfectious Diseases: Leprosy Case Series in The Emergency Room: A Warning Sign For A Challenging DiagnosisDaffa Muhamad Hadyan ZainNessuna valutazione finora
- EULEP Group Documents on Late Effects of RadiationDocumento50 pagineEULEP Group Documents on Late Effects of RadiationDiana Buzatu100% (1)
- Research Paper On LupusDocumento4 pagineResearch Paper On Lupusfyrj7h9z100% (1)
- Tmbhan Referat FiztrikDocumento4 pagineTmbhan Referat FiztrikAde Irwan SuryadiNessuna valutazione finora
- 5 - LeprosyDocumento15 pagine5 - LeprosyCaila LimNessuna valutazione finora
- Sarcoidosis (Heerfordt Syndrome) : A Case Report: Tiia Tamme, Edvitar Leibur, Andres KullaDocumento4 pagineSarcoidosis (Heerfordt Syndrome) : A Case Report: Tiia Tamme, Edvitar Leibur, Andres KullajaquelineartNessuna valutazione finora
- Distal Radius and UlnaDocumento40 pagineDistal Radius and UlnaDia CembranoNessuna valutazione finora
- RadPos Summary 2Documento9 pagineRadPos Summary 2Jocel LongosNessuna valutazione finora
- 5001: Focus On Upper and Lower Limbs and Chest:: ST ST THDocumento3 pagine5001: Focus On Upper and Lower Limbs and Chest:: ST ST TH'Emily MillsNessuna valutazione finora
- Bones WorksheetDocumento3 pagineBones WorksheetSulthan Ramiz0% (1)
- Elbow ComplexDocumento17 pagineElbow ComplexLeslie RognstadNessuna valutazione finora
- Paid Orthobullet MCQs - AnatomyDocumento22 paginePaid Orthobullet MCQs - AnatomyMohamad Ramadan33% (3)
- Anatomy and Physiology ReviewerDocumento49 pagineAnatomy and Physiology ReviewerCourtney Dela FierraNessuna valutazione finora
- GALEAZZI AND MONTEGGIA FRACTURE CAREDocumento31 pagineGALEAZZI AND MONTEGGIA FRACTURE CAREnihthaNessuna valutazione finora
- Muscle AnatomyDocumento3 pagineMuscle AnatomyJosue CastilloNessuna valutazione finora
- Madelung's Deformity of The Wrist-CurrentDocumento4 pagineMadelung's Deformity of The Wrist-CurrentAnonymous bUBXIFfNessuna valutazione finora
- Cross Sections of Upper LimbDocumento12 pagineCross Sections of Upper LimbBigBoostingNessuna valutazione finora
- Muscle IdentificationDocumento7 pagineMuscle Identificationhakdog hakdogNessuna valutazione finora
- Both Bone # of ForearmDocumento40 pagineBoth Bone # of ForearmSashmi Sareen ManandharNessuna valutazione finora
- Access To Surgery 500 SBA AnatomyDocumento51 pagineAccess To Surgery 500 SBA Anatomytoichongw50% (8)
- Anatomy ListDocumento9 pagineAnatomy ListMartin ClydeNessuna valutazione finora
- Veterinary Anatomy Coloring BookDocumento53 pagineVeterinary Anatomy Coloring BookJuliana Escudero100% (4)
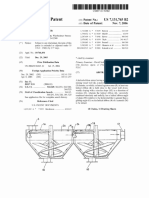
- Helical-Ribbon Mixer with Improved Mixing Performance and Self-Emptying PropertiesDocumento16 pagineHelical-Ribbon Mixer with Improved Mixing Performance and Self-Emptying PropertiesEduardo Fernandez DazaNessuna valutazione finora
- Anatomy QuestionDocumento22 pagineAnatomy Questionشاجوان عباس محمد احمدNessuna valutazione finora
- Modified Kapandji Wiring TechniqueDocumento4 pagineModified Kapandji Wiring TechniquemonkeyzergNessuna valutazione finora
- EVOS Wrist Surgical Technique Smith and NephewDocumento32 pagineEVOS Wrist Surgical Technique Smith and NephewWillem SmitNessuna valutazione finora
- 1-Bones of The Upper Limb Final-2Documento18 pagine1-Bones of The Upper Limb Final-2DrVasu Mudiraj100% (1)
- تجميع المذكرات الاورثوDocumento59 pagineتجميع المذكرات الاورثوMarah AbdulrahimNessuna valutazione finora
- Muscles of the Shoulder and ArmDocumento14 pagineMuscles of the Shoulder and ArmFanserbia100% (1)
- Anatomy Summary From MooreDocumento131 pagineAnatomy Summary From MooreNishma Malde100% (2)
- The Basic Principles of External Fixation Using The Ilizarov DeviceDocumento30 pagineThe Basic Principles of External Fixation Using The Ilizarov DevicedendroaspisblackNessuna valutazione finora
- LOG BOOK: ORTHOPEDIC AND TRAUMATOLOGY MAGANGDocumento32 pagineLOG BOOK: ORTHOPEDIC AND TRAUMATOLOGY MAGANGrandy rakhmatNessuna valutazione finora
- Hygienic Physiology: With Special Reference To The Use of Alcoholic Drinks and Narcotics by Steele, Joel DormanDocumento235 pagineHygienic Physiology: With Special Reference To The Use of Alcoholic Drinks and Narcotics by Steele, Joel DormanGutenberg.orgNessuna valutazione finora
- Clinical Anatomy of the Hand: A Guide for SurgeonsDocumento54 pagineClinical Anatomy of the Hand: A Guide for Surgeonsmarikos82Nessuna valutazione finora
- Arterial Puncture: Claire Babcock O'ConnellDocumento10 pagineArterial Puncture: Claire Babcock O'ConnellGerson Tocno LopezNessuna valutazione finora
- The Endoskeleton of Birds.Documento29 pagineThe Endoskeleton of Birds.Ian LasarianoNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 3.5 su 5 stelle3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNessuna valutazione finora
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementDa EverandTechniques Exercises And Tricks For Memory ImprovementValutazione: 4.5 su 5 stelle4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 5 su 5 stelle5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesDa EverandThe Ultimate Guide To Memory Improvement TechniquesValutazione: 5 su 5 stelle5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 5 su 5 stelle5/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 3.5 su 5 stelle3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDa EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisValutazione: 5 su 5 stelle5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDa EverandThe Happiness Trap: How to Stop Struggling and Start LivingValutazione: 4 su 5 stelle4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- The Tennis Partner: A Doctor's Story of Friendship and LossDa EverandThe Tennis Partner: A Doctor's Story of Friendship and LossValutazione: 4.5 su 5 stelle4.5/5 (4)