Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Stretching To Stay Young - Simple Workouts To Keep You Flexible, Energized, and Pain FreeDocumento248 pagineStretching To Stay Young - Simple Workouts To Keep You Flexible, Energized, and Pain Freeeliseo_pamandanan75% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Phase 1 & 2 Bodybuilding Workout and Diet PlanDocumento7 paginePhase 1 & 2 Bodybuilding Workout and Diet PlanBrandon Foley83% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Training System For Enhancing Athletic Performance Al VermeilDocumento165 pagineTraining System For Enhancing Athletic Performance Al Vermeilxaviermay100% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Quiz Osteopathic Part 1 of 4Documento51 pagineQuiz Osteopathic Part 1 of 4MedShare100% (3)
- 12 Top Exercises For Higher Kicks TKDCoach - AcademyDocumento16 pagine12 Top Exercises For Higher Kicks TKDCoach - AcademytestNessuna valutazione finora
- Skeleton-Worksheet KEY ANSWERDocumento4 pagineSkeleton-Worksheet KEY ANSWERjustine alina50% (2)
- Week 1-6 FRC Mobility and Stabilization ExercisesDocumento12 pagineWeek 1-6 FRC Mobility and Stabilization ExercisesRob Banach100% (1)
- Muscles Covered in The Trigger Point ChartsDocumento19 pagineMuscles Covered in The Trigger Point ChartsSaninan Mat100% (5)
- Igcse Flash CardsDocumento13 pagineIgcse Flash Cardsapi-588487311Nessuna valutazione finora
- Scapula LandmarksDocumento9 pagineScapula LandmarksxoNessuna valutazione finora
- Coaptation Slab ImmobilizationDocumento10 pagineCoaptation Slab ImmobilizationabdmaliknasNessuna valutazione finora
- Myology ComposDocumento117 pagineMyology ComposjehanNessuna valutazione finora
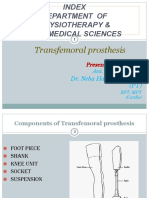
- TRANSFEMORAL - PPT 1Documento64 pagineTRANSFEMORAL - PPT 1Farheen KhanNessuna valutazione finora
- Meniscus Repair ProtocolDocumento2 pagineMeniscus Repair ProtocolFlorentinaDinNessuna valutazione finora
- Arbour2013 HypoplasiaDocumento5 pagineArbour2013 HypoplasiaCarolina GomezNessuna valutazione finora
- Concept Map TemplateDocumento4 pagineConcept Map TemplateaamenaNessuna valutazione finora
- Politeus Msl.Documento6 paginePoliteus Msl.Ajay Pal NattNessuna valutazione finora
- Anatomy Bones and SkeletonDocumento4 pagineAnatomy Bones and Skeletonタナトス ThanatosNessuna valutazione finora
- MnemonicsDocumento4 pagineMnemonicsramonlimNessuna valutazione finora
- Myelomeningocele classificationDocumento5 pagineMyelomeningocele classificationLema Ulloa ZoraidaNessuna valutazione finora
- Subacromial BursitisDocumento28 pagineSubacromial BursitisRonak PatelNessuna valutazione finora
- Kettlebell Swing AlternativesDocumento4 pagineKettlebell Swing AlternativesCeline Kyla MalloNessuna valutazione finora
- Arthroscopic Acromioplasty ProtocolDocumento2 pagineArthroscopic Acromioplasty ProtocolporongporongNessuna valutazione finora
- Anatomski Atlas Sobotta Na Njemacki PDFDocumento68 pagineAnatomski Atlas Sobotta Na Njemacki PDFEmir JašarevićNessuna valutazione finora
- Skeletal System ExamDocumento9 pagineSkeletal System ExamBijay Kumar Mahato100% (1)
- Rad 331 - Upper Limb (Humerus) : Muhammad Njiti, Msc. Medical Radiography Dept. College of Medical Sciences, UnimaidDocumento34 pagineRad 331 - Upper Limb (Humerus) : Muhammad Njiti, Msc. Medical Radiography Dept. College of Medical Sciences, UnimaidJameeluh TijjanyNessuna valutazione finora
- Human Anatomy and Fiology: by Firdaus. M.PDDocumento15 pagineHuman Anatomy and Fiology: by Firdaus. M.PDPrinces 1234Nessuna valutazione finora
- Anatomy of The Lower LimbDocumento3 pagineAnatomy of The Lower LimbRayNessuna valutazione finora
- Nonsurgical Shoulder Impingement Rehabilitation Protocol: Ramin R. Tabaddor, MD Arlene D. Kavanagh, PA-CDocumento4 pagineNonsurgical Shoulder Impingement Rehabilitation Protocol: Ramin R. Tabaddor, MD Arlene D. Kavanagh, PA-CRiaz KhanNessuna valutazione finora
- Muscular System GuideDocumento3 pagineMuscular System GuidebuenaNessuna valutazione finora