Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Symmetrir and Order. Reasons To Live According The LodgeDocumento6 pagineSymmetrir and Order. Reasons To Live According The LodgeAnonymous zfNrN9NdNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- TDS-11SH Top Drive D392004689-MKT-001 Rev. 01Documento2 pagineTDS-11SH Top Drive D392004689-MKT-001 Rev. 01Israel Medina100% (2)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Meanings of Goddess PT IIIDocumento14 pagineThe Meanings of Goddess PT IIILevonce68Nessuna valutazione finora
- Workshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Documento33 pagineWorkshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Ilie Viorel75% (4)
- Property Case Digest DonationDocumento13 pagineProperty Case Digest DonationJesselle Maminta100% (1)
- P4 Science Topical Questions Term 1Documento36 pagineP4 Science Topical Questions Term 1Sean Liam0% (1)
- LANY Lyrics: "Thru These Tears" LyricsDocumento2 pagineLANY Lyrics: "Thru These Tears" LyricsAnneNessuna valutazione finora
- GDCR - Second RevisedDocumento290 pagineGDCR - Second RevisedbhaveshbhoiNessuna valutazione finora
- ReflectionDocumento3 pagineReflectionapi-174391216Nessuna valutazione finora
- Synopsis SsDocumento14 pagineSynopsis SsJYOTI KATIYAR SVUNessuna valutazione finora
- MARKETING STUDY EditedDocumento48 pagineMARKETING STUDY EditedRichard Rhamil Carganillo Garcia Jr.Nessuna valutazione finora
- Btech CertificatesDocumento6 pagineBtech CertificatesSuresh VadlamudiNessuna valutazione finora
- Maharashtra State Board of Technical Education. Academic Monitoring Department ProfileDocumento14 pagineMaharashtra State Board of Technical Education. Academic Monitoring Department Profilevspd2010Nessuna valutazione finora
- Centric WhitepaperDocumento25 pagineCentric WhitepaperFadhil ArsadNessuna valutazione finora
- Pelatihan Dan Workshop Peningkatan Kompetensi GuruDocumento6 paginePelatihan Dan Workshop Peningkatan Kompetensi Guruhenry jakatariNessuna valutazione finora
- Introduction To Cobit Framework - Week 3Documento75 pagineIntroduction To Cobit Framework - Week 3Teddy HaryadiNessuna valutazione finora
- What Role Does Imagination Play in Producing Knowledge About The WorldDocumento1 paginaWhat Role Does Imagination Play in Producing Knowledge About The WorldNathanael Samuel KuruvillaNessuna valutazione finora
- Prevention of Power Theft Using Concept of Multifunction Meter and PLCDocumento6 paginePrevention of Power Theft Using Concept of Multifunction Meter and PLCMuhammad FarhanNessuna valutazione finora
- Cambridge IGCSE: PHYSICS 0625/62Documento12 pagineCambridge IGCSE: PHYSICS 0625/62EffNessuna valutazione finora
- Paper 11-ICOSubmittedDocumento10 paginePaper 11-ICOSubmittedNhat Tan MaiNessuna valutazione finora
- Baumer Tdp02 Tdpz02 Ds enDocumento4 pagineBaumer Tdp02 Tdpz02 Ds enQamar ZiaNessuna valutazione finora
- Poster PresentationDocumento3 paginePoster PresentationNipun RavalNessuna valutazione finora
- His 101 Final ReportDocumento15 pagineHis 101 Final ReportShohanur RahmanNessuna valutazione finora
- Heart Attack Detection ReportDocumento67 pagineHeart Attack Detection ReportAkhil TejaNessuna valutazione finora
- Second Language Learning in The Classroom PDFDocumento2 pagineSecond Language Learning in The Classroom PDFThanh Phương VõNessuna valutazione finora
- The Role of IT in TQM L'Oreal Case StudyDocumento9 pagineThe Role of IT in TQM L'Oreal Case StudyUdrea RoxanaNessuna valutazione finora
- Cooperative LinuxDocumento39 pagineCooperative Linuxrajesh_124Nessuna valutazione finora
- Project 2 Analysis of Florida WaterDocumento8 pagineProject 2 Analysis of Florida WaterBeau Beauchamp100% (1)
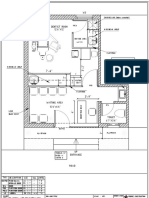
- Dental Clinic - Floor Plan R3-2Documento1 paginaDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)