Potrebbero piacerti anche
- Patch Tweak. Exploring Modular Synthesis (Kim Bjørn, Chris Meyer)Documento368 paginePatch Tweak. Exploring Modular Synthesis (Kim Bjørn, Chris Meyer)Guiga Jovuá100% (6)
- The Shepherd - Karl JenkinsDocumento7 pagineThe Shepherd - Karl JenkinsAlesagas100% (4)
- Virginia PCRDocumento3 pagineVirginia PCRdandude505Nessuna valutazione finora
- Virginia PCRDocumento3 pagineVirginia PCRdandude505Nessuna valutazione finora
- PEAC Rheumatology - Approach To A Patient With Joint PainDocumento34 paginePEAC Rheumatology - Approach To A Patient With Joint PainSdNessuna valutazione finora
- The Delvers Guide Wagon Sheet Form Fillable PDFDocumento2 pagineThe Delvers Guide Wagon Sheet Form Fillable PDFJhon Jairo ReveloNessuna valutazione finora
- 5625 Operator Manual GEHL Skid SteerDocumento92 pagine5625 Operator Manual GEHL Skid Steeraugustuswg75% (4)
- New York State FR PCRDocumento2 pagineNew York State FR PCRdandude505Nessuna valutazione finora
- New York State PCRDocumento3 pagineNew York State PCRdandude505Nessuna valutazione finora
- NAS1330 Rev 10Documento5 pagineNAS1330 Rev 10mxNessuna valutazione finora
- General notes on isolators and earth switchesDocumento1 paginaGeneral notes on isolators and earth switchessparkCENessuna valutazione finora
- MD80 Ata28-00 A3c Fuel SysDocumento1 paginaMD80 Ata28-00 A3c Fuel Sysreza mirzakhaniNessuna valutazione finora
- UT-M-T03-35000 (R1) - Model - pdf2Documento1 paginaUT-M-T03-35000 (R1) - Model - pdf2Abid KayaniNessuna valutazione finora
- Column footing schedule and detailsDocumento1 paginaColumn footing schedule and detailsDipanjan SomeNessuna valutazione finora
- DIS DR-2: Losure Summary PageDocumento4 pagineDIS DR-2: Losure Summary PageZach EdwardsNessuna valutazione finora
- A320 Ata 21 (2) CattsDocumento1 paginaA320 Ata 21 (2) CattsabmedhussNessuna valutazione finora
- Lndustri: National Aerosp Ce StandardDocumento2 pagineLndustri: National Aerosp Ce StandardDinesh Bhandari100% (3)
- Scan Feb 4, 2022Documento1 paginaScan Feb 4, 2022zunijemNessuna valutazione finora
- UT-M-T01-15000 (R1) - Model - pdf2Documento1 paginaUT-M-T01-15000 (R1) - Model - pdf2Abid KayaniNessuna valutazione finora
- 5Th and 7Th Floor Plan: Scale 1:300Documento1 pagina5Th and 7Th Floor Plan: Scale 1:300Princess Gonzales LansangNessuna valutazione finora
- 日產零件手冊F04 02Documento702 pagine日產零件手冊F04 02James HuangNessuna valutazione finora
- B737max8 Corrected FaclivDocumento9 pagineB737max8 Corrected FaclivNGUYỄN BìnhNessuna valutazione finora
- PROCESSDocumento1 paginaPROCESSanujs_87Nessuna valutazione finora
- CP - VISTA HUB BGC - 08112017-ModelDocumento1 paginaCP - VISTA HUB BGC - 08112017-ModelAngelo AguinaldoNessuna valutazione finora
- Power Plant Fire Safety MapDocumento1 paginaPower Plant Fire Safety MapmakNessuna valutazione finora
- 4Th and 6Th Floor Plan: Scale 1:300Documento1 pagina4Th and 6Th Floor Plan: Scale 1:300Princess Gonzales LansangNessuna valutazione finora
- Plano de Taller Grande SerigrafiaDocumento1 paginaPlano de Taller Grande SerigrafiatwoemNessuna valutazione finora
- Emco Winnc Heidenhain TNC 426 Conversational The Emco Winnc Heidenhain TNC 426Documento282 pagineEmco Winnc Heidenhain TNC 426 Conversational The Emco Winnc Heidenhain TNC 426AyoubNessuna valutazione finora
- Ng-De - 25+270 - (1X30) - Sub 202-SS 202Documento1 paginaNg-De - 25+270 - (1X30) - Sub 202-SS 202krishna jhaNessuna valutazione finora
- B17C B25C A3 All BLACK WHITEDocumento5 pagineB17C B25C A3 All BLACK WHITEMIANessuna valutazione finora
- Master PlanDocumento1 paginaMaster PlanPoorvi ShanthaNessuna valutazione finora
- M&M Editable Character Type ENDocumento2 pagineM&M Editable Character Type ENDeiron McVerityNessuna valutazione finora
- Gij Scarlett Level 20 v2Documento2 pagineGij Scarlett Level 20 v2AbulonNessuna valutazione finora
- Gij RPG Pregen Commando Wizard SheetDocumento2 pagineGij RPG Pregen Commando Wizard SheetColin BraddockNessuna valutazione finora
- Affinity Designer Shortcuts Cheat Sheet (May 2017 Updated)Documento6 pagineAffinity Designer Shortcuts Cheat Sheet (May 2017 Updated)machondaNessuna valutazione finora
- NAD Model 4300 Stereo Tuner ManualDocumento5 pagineNAD Model 4300 Stereo Tuner Manualarkansas23Nessuna valutazione finora
- Testing Evaluation TireDocumento18 pagineTesting Evaluation TiresiritapeNessuna valutazione finora
- 2502 ArriboDocumento64 pagine2502 Arriboerick gonzalezNessuna valutazione finora
- S082252AC 9200i Sistem ElectriDocumento93 pagineS082252AC 9200i Sistem ElectriOmar ReyesNessuna valutazione finora
- 2014 System Wiring Diagrams Jeep - PatriotDocumento69 pagine2014 System Wiring Diagrams Jeep - PatriotAlfonso GarcíaNessuna valutazione finora
- Finish Floor Line: Reflected Ceiling Plan Reflected Ceiling Plan Reflected Ceiling PlanDocumento1 paginaFinish Floor Line: Reflected Ceiling Plan Reflected Ceiling Plan Reflected Ceiling PlanDerf Jayson AdanteNessuna valutazione finora
- LV Adjustii NT) ND) Cation Sepalator: Ai3) Fjlly 125Documento8 pagineLV Adjustii NT) ND) Cation Sepalator: Ai3) Fjlly 125RM HaroonNessuna valutazione finora
- A320 Ata 29 CattsDocumento1 paginaA320 Ata 29 CattsabmedhussNessuna valutazione finora
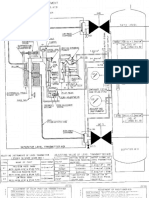
- Limpet Reaction Vessel PDFDocumento1 paginaLimpet Reaction Vessel PDFarajamani78Nessuna valutazione finora
- ZF5HP19FL AtsgDocumento20 pagineZF5HP19FL AtsgJose garcua vargas 2006401321100% (1)
- Sto. Domingo Hea SampleDocumento10 pagineSto. Domingo Hea SampleThan KrisNessuna valutazione finora
- Cycle Time For CY OP-50Documento4 pagineCycle Time For CY OP-50Ramanand YadavNessuna valutazione finora
- Basement Parking: DN DN DN DN DN DN DNDocumento1 paginaBasement Parking: DN DN DN DN DN DN DNKripasindhu BordoloiNessuna valutazione finora
- Capacity SheetDocumento1 paginaCapacity Sheetable.ankit.94Nessuna valutazione finora
- NGL3 CouplingDocumento5 pagineNGL3 CouplingKousik RoyNessuna valutazione finora
- Temporary Storage Areas and Emergency Contact DetailsDocumento1 paginaTemporary Storage Areas and Emergency Contact DetailsmakNessuna valutazione finora
- National Aerospace Standard outlines steel screw marking requirementsDocumento2 pagineNational Aerospace Standard outlines steel screw marking requirementsVéronique RacicotNessuna valutazione finora
- SEMESTER-2 AUTOMOBILE ENGINEERING RESULT PASS/FAIL STATUSDocumento7 pagineSEMESTER-2 AUTOMOBILE ENGINEERING RESULT PASS/FAIL STATUSShashwat ThakurNessuna valutazione finora
- Valve Data SheetDocumento4 pagineValve Data SheetRoy F BastariNessuna valutazione finora
- Boeing-757 Overhead PanelDocumento1 paginaBoeing-757 Overhead PanelAndrewNessuna valutazione finora
- Practical Electronics 1967 02 S OCR PDFDocumento84 paginePractical Electronics 1967 02 S OCR PDFCarlos SoaresNessuna valutazione finora
- A320 Ata 32 (6) CattsDocumento1 paginaA320 Ata 32 (6) CattsabmedhussNessuna valutazione finora
- Rrrre'-G,: Periodical Pump Volvo BoosterDocumento4 pagineRrrre'-G,: Periodical Pump Volvo BoosterGanjar PangestiadiNessuna valutazione finora
- Print Section 3 Yamatake SFC For DSTJ TransmittersDocumento13 paginePrint Section 3 Yamatake SFC For DSTJ TransmittersaloordominicNessuna valutazione finora
- Final Ground Floor Plan-ModelDocumento1 paginaFinal Ground Floor Plan-ModelAIML 35 MIHIR MHATRENessuna valutazione finora
- UntitledDocumento41 pagineUntitledPol PolkaNessuna valutazione finora
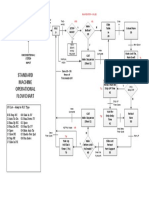
- StandardDocumento1 paginaStandardBlagoja Anna SotirovskiNessuna valutazione finora
- Legal Aspects of EMSDocumento2 pagineLegal Aspects of EMSdandude505Nessuna valutazione finora
- Mandatory ReportingDocumento1 paginaMandatory Reportingdandude505Nessuna valutazione finora
- 95 EVOC Instructor GuideDocumento637 pagine95 EVOC Instructor Guidedandude505100% (1)
- 1994 Curriculum EmtDocumento4 pagine1994 Curriculum Emtdandude505Nessuna valutazione finora
- Wustl PCRDocumento2 pagineWustl PCRdandude505Nessuna valutazione finora
- At The Legal Limit - NYTime..Documento6 pagineAt The Legal Limit - NYTime..dandude505Nessuna valutazione finora
- Home Region 1 Committees Education Resources DP1Documento1 paginaHome Region 1 Committees Education Resources DP1dandude505Nessuna valutazione finora
- AD DeathDocumento25 pagineAD Deathdandude505Nessuna valutazione finora
- EMS On-Call Pay and The FLSADocumento3 pagineEMS On-Call Pay and The FLSAdandude505Nessuna valutazione finora
- Advice For New EMT's - Pink..Documento12 pagineAdvice For New EMT's - Pink..dandude505Nessuna valutazione finora
- Boston PCRDocumento1 paginaBoston PCRdandude505Nessuna valutazione finora
- Umass Lowell PCRDocumento1 paginaUmass Lowell PCRdandude505Nessuna valutazione finora
- New Hampshire PCRDocumento2 pagineNew Hampshire PCRdandude505Nessuna valutazione finora
- Mount Holyoke PCRDocumento1 paginaMount Holyoke PCRdandude505Nessuna valutazione finora
- Va Tech Standby ReleaseDocumento2 pagineVa Tech Standby Releasedandude505Nessuna valutazione finora
- Johns Hopkins PCRDocumento1 paginaJohns Hopkins PCRdandude505Nessuna valutazione finora
- Va Tech Standby ReportDocumento1 paginaVa Tech Standby Reportdandude505Nessuna valutazione finora
- GSA Federal Specification for Star-of-Life Ambulance KKK-A-1822EDocumento110 pagineGSA Federal Specification for Star-of-Life Ambulance KKK-A-1822EphilcogabiNessuna valutazione finora
- Mass Event Zone PlanningDocumento9 pagineMass Event Zone Planningdandude505Nessuna valutazione finora
- Continuing Education ManualDocumento33 pagineContinuing Education Manualdandude505Nessuna valutazione finora
- Rice University's Public Access Defib ProposalDocumento13 pagineRice University's Public Access Defib Proposaldandude505Nessuna valutazione finora
- Laws of The House of GodDocumento2 pagineLaws of The House of Goddandude505Nessuna valutazione finora
- Paramedic Assist Course OutlineDocumento6 pagineParamedic Assist Course Outlinedandude505Nessuna valutazione finora
- Treatment Protocols 704.JUNE.08Documento161 pagineTreatment Protocols 704.JUNE.08dandude505100% (3)
- Sick Ems HumorDocumento13 pagineSick Ems Humordandude505100% (1)
- EmtbnscDocumento681 pagineEmtbnscGel OmugtongNessuna valutazione finora
- Deep Vein Thrombosis: Causes Treatment Complications PreventionDocumento5 pagineDeep Vein Thrombosis: Causes Treatment Complications PreventionRaghav Suri100% (2)
- F8DB F089:Fungal InfectionsDocumento6 pagineF8DB F089:Fungal InfectionsPharmacist Ehab HammadNessuna valutazione finora
- What Causes Failure To Thrive in A Child?Documento1 paginaWhat Causes Failure To Thrive in A Child?Bhie BhieNessuna valutazione finora
- Diagnosa DokterDocumento1 paginaDiagnosa Dokteranton nioNessuna valutazione finora
- ANHE 426 Introduction To Animal Diseases NewDocumento65 pagineANHE 426 Introduction To Animal Diseases NewSamuel MutungaNessuna valutazione finora
- 155 (Milla, Sara)Documento24 pagine155 (Milla, Sara)Nourma Kusuma WinawanNessuna valutazione finora
- Science-9-Q1 M2 - Efren Agdinaoay JRDocumento29 pagineScience-9-Q1 M2 - Efren Agdinaoay JRLiezl ValienteNessuna valutazione finora
- Worksheet #3 VOCABULARYDocumento2 pagineWorksheet #3 VOCABULARYAngel Angeleri-priftis.Nessuna valutazione finora
- Communicable Disease NursingDocumento23 pagineCommunicable Disease NursingWinter SparkleNessuna valutazione finora
- Karol The Great Plague 15 01 15Documento4 pagineKarol The Great Plague 15 01 15api-276953527Nessuna valutazione finora
- Diphtheria 1Documento24 pagineDiphtheria 1Anam AbidNessuna valutazione finora
- Case Simu 104Documento4 pagineCase Simu 104Princess Levie CenizaNessuna valutazione finora
- Leprosy CHNDocumento14 pagineLeprosy CHNPhillip ChingNessuna valutazione finora
- Balzano1997 PDFDocumento8 pagineBalzano1997 PDFPaulina Sobarzo VegaNessuna valutazione finora
- Dane Diagnostics (P) LTD: Covid-19 Test ReportDocumento1 paginaDane Diagnostics (P) LTD: Covid-19 Test ReportSreesobh SreeNessuna valutazione finora
- Infection Prevention and Control at NICU Slide Deck 2.8.2018 PDFDocumento134 pagineInfection Prevention and Control at NICU Slide Deck 2.8.2018 PDFRevathi DadamNessuna valutazione finora
- Chapter 16 Infections of The Eye and Nervous SystemDocumento10 pagineChapter 16 Infections of The Eye and Nervous SystemEanna ParadoNessuna valutazione finora
- Viral Myositis: Causes, Symptoms, DiagnosisDocumento3 pagineViral Myositis: Causes, Symptoms, DiagnosisemirkurtalicNessuna valutazione finora
- 04 Prof DR Cissy Vaksin Untuk Mencegah Pneumonia Pneumokokus - ColourDocumento40 pagine04 Prof DR Cissy Vaksin Untuk Mencegah Pneumonia Pneumokokus - ColourYuuki Putri HidayatNessuna valutazione finora
- 1 Outbreak InvestigationDocumento48 pagine1 Outbreak InvestigationAbdul Charis Konoras100% (1)
- QN BNK Og PeadDocumento39 pagineQN BNK Og PeadZemen addiss100% (2)
- P3 MicroDocumento14 pagineP3 MicroDaniel GalitzineNessuna valutazione finora
- Abbreviations and Symbols Commonly Used by Health Practitioners ActivitiesDocumento10 pagineAbbreviations and Symbols Commonly Used by Health Practitioners ActivitiesAprilia PratiwiNessuna valutazione finora
- ObsernDocumento1 paginaObsernGobi NavaNessuna valutazione finora
- Investigatory Project BiologyDocumento31 pagineInvestigatory Project BiologyRonaldNessuna valutazione finora
- Coronavirus FactsheetDocumento8 pagineCoronavirus FactsheetJm2345234029Nessuna valutazione finora
- New Flu Shot Approved by FDADocumento6 pagineNew Flu Shot Approved by FDAHaraprasad NanjundappaNessuna valutazione finora
- Clinical Case 38-Chronic Pelvic PainDocumento2 pagineClinical Case 38-Chronic Pelvic Painselina kalenderNessuna valutazione finora
- Public Health Model PptDocumento10 paginePublic Health Model PptSurendra SanapNessuna valutazione finora