Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Mikhail TombakDocumento20 pagineMikhail TombakSamson Ana-MariaNessuna valutazione finora
- Notes For Frca PDFDocumento580 pagineNotes For Frca PDFMithul Vijayaraj100% (3)
- Combo Hospital Coding TestDocumento7 pagineCombo Hospital Coding Testmscorella13% (8)
- Epidemiology QuestionsDocumento7 pagineEpidemiology Questionsbravof86% (7)
- Axa PhilDocumento13 pagineAxa PhilKat EspanoNessuna valutazione finora
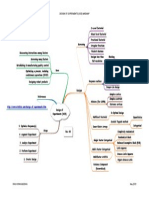
- Design of Experiments (DOE) MindmapDocumento1 paginaDesign of Experiments (DOE) MindmapRavi KiranNessuna valutazione finora
- Failure Mode & Effects Analysis (FMEA) - A3 SizeDocumento1 paginaFailure Mode & Effects Analysis (FMEA) - A3 SizeRavi KiranNessuna valutazione finora
- Failure Mode & Effects Analysis (FMEA) - A3 SizeDocumento1 paginaFailure Mode & Effects Analysis (FMEA) - A3 SizeRavi KiranNessuna valutazione finora
- 8D Problem Solving Methodology1Documento1 pagina8D Problem Solving Methodology1Ravi KiranNessuna valutazione finora
- Tattva BodhaDocumento1 paginaTattva BodhaRavi Kiran100% (2)
- Respiratory Set 2 QDocumento7 pagineRespiratory Set 2 QshaNessuna valutazione finora
- Timing of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialDocumento9 pagineTiming of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialWelly WijayaNessuna valutazione finora
- Full Download Ebook Ebook PDF Medical Surgical Nursing Assessment and Management of Clinical Problems 10th Edition PDFDocumento30 pagineFull Download Ebook Ebook PDF Medical Surgical Nursing Assessment and Management of Clinical Problems 10th Edition PDFgregory.love731100% (38)
- 2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesDocumento4 pagine2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesKindylight KindylightNessuna valutazione finora
- Medical Uses of NitinolDocumento8 pagineMedical Uses of NitinolMarius Alin LupașcuNessuna valutazione finora
- (CPB) Pediatric UpdateDocumento11 pagine(CPB) Pediatric Updateccvped3dNessuna valutazione finora
- Media Files 2015 International Symposium Att G5translating A Lowcost Highquality Multispeciality Hospital Model To New EnvironmentsDocumento13 pagineMedia Files 2015 International Symposium Att G5translating A Lowcost Highquality Multispeciality Hospital Model To New EnvironmentsManashNessuna valutazione finora
- Philippine Nursing Seminars and Training May 2011Documento3 paginePhilippine Nursing Seminars and Training May 2011PhilippineNursingDirectory.comNessuna valutazione finora
- CABG Versus PCI For Complex Coronary Disease: Time To Close The BooksDocumento3 pagineCABG Versus PCI For Complex Coronary Disease: Time To Close The Booksmutiara suciNessuna valutazione finora
- Nejmoa2206606 AppendixDocumento41 pagineNejmoa2206606 AppendixAndikaputra Brahma WidiantoroNessuna valutazione finora
- Combined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFDocumento10 pagineCombined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFIsfan RialdyNessuna valutazione finora
- MidcabDocumento7 pagineMidcabNs PadiludinNessuna valutazione finora
- Blood Lactate Predicts Mortality After Surgical Repair of Type A Acute Aortic DissectionDocumento10 pagineBlood Lactate Predicts Mortality After Surgical Repair of Type A Acute Aortic Dissectiondaia4322746Nessuna valutazione finora
- PIIS0003497504010409Documento2 paginePIIS0003497504010409redaNessuna valutazione finora
- Cardiac Surgeries PPT FinalDocumento55 pagineCardiac Surgeries PPT FinalDumora FatmaNessuna valutazione finora
- CABG x4Documento2 pagineCABG x4Indranil SinhaNessuna valutazione finora
- Minimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarDocumento3 pagineMinimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarBest Heart Bypass Surgery Dr. Gauranga MajumdarNessuna valutazione finora
- Next Step Advanced Medical Coding and Auditing 2017 2018 Edition 1St Edition Buck Solutions Manual Full Chapter PDFDocumento36 pagineNext Step Advanced Medical Coding and Auditing 2017 2018 Edition 1St Edition Buck Solutions Manual Full Chapter PDFmichaelkrause22011998gdj100% (8)
- Heart MafiaDocumento1 paginaHeart Mafiaastf mahboobNessuna valutazione finora
- Heart Transplant Surgery - Docx 2Documento6 pagineHeart Transplant Surgery - Docx 2oguzguneri2010Nessuna valutazione finora
- Heart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsDocumento13 pagineHeart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsJOSHUA DICHOSONessuna valutazione finora
- 2020 The Place of Extracorporeal Life Support In.98996Documento8 pagine2020 The Place of Extracorporeal Life Support In.98996Miky DinuNessuna valutazione finora
- Hartrevalidatie PRL Eng KNGFDocumento52 pagineHartrevalidatie PRL Eng KNGFsilkofosNessuna valutazione finora
- Approved Abbreviations For Use in Clinical Records and Letters PDFDocumento10 pagineApproved Abbreviations For Use in Clinical Records and Letters PDFwhateverworkNessuna valutazione finora
- CABG PCS CodingDocumento3 pagineCABG PCS CodingVikas MaheshwariNessuna valutazione finora