Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Symmetrir and Order. Reasons To Live According The LodgeDocumento6 pagineSymmetrir and Order. Reasons To Live According The LodgeAnonymous zfNrN9NdNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- MRI Adult SpineDocumento16 pagineMRI Adult SpineFarkhan Putra IINessuna valutazione finora
- Hydraulic Excavator: Engine WeightsDocumento28 pagineHydraulic Excavator: Engine WeightsFelipe Pisklevits LaubeNessuna valutazione finora
- ESG Conundrum PDFDocumento30 pagineESG Conundrum PDFVijay Kumar SwamiNessuna valutazione finora
- Spinal Manipulative Therapy For Chronic Low-Back PainCD008112Documento178 pagineSpinal Manipulative Therapy For Chronic Low-Back PainCD008112Farkhan Putra IINessuna valutazione finora
- Labor Analgesia An UpdateDocumento86 pagineLabor Analgesia An UpdateFarkhan Putra IINessuna valutazione finora
- Acr Technical Standard For Diagnostic Medical Physics Performance Monitoring of Magnetic Resonance Imaging (Mri) EquipmentDocumento4 pagineAcr Technical Standard For Diagnostic Medical Physics Performance Monitoring of Magnetic Resonance Imaging (Mri) EquipmentFarkhan Putra IINessuna valutazione finora
- Defining Acute Mild Head Injury in Adults - A Proposal BasedDocumento9 pagineDefining Acute Mild Head Injury in Adults - A Proposal BasedPaijo SusenoNessuna valutazione finora
- MRI WristDocumento14 pagineMRI WristFarkhan Putra IINessuna valutazione finora
- MRI MSK InfectionsDocumento9 pagineMRI MSK InfectionsFarkhan Putra IINessuna valutazione finora
- Lightning and Its Association With The Frequency of Headache in Migraineurs: An Observational Cohort StudyDocumento9 pagineLightning and Its Association With The Frequency of Headache in Migraineurs: An Observational Cohort StudyFarkhan Putra IINessuna valutazione finora
- Chronic Migraine Revised Appendix Criteria ICHD 2Documento5 pagineChronic Migraine Revised Appendix Criteria ICHD 2Farkhan Putra IINessuna valutazione finora
- Treatment HeadacheDocumento6 pagineTreatment HeadachehverdianNessuna valutazione finora
- 1941 Iraq and The IlluminatiDocumento4 pagine1941 Iraq and The IlluminatiZaneWeltonNessuna valutazione finora
- The Life Cycle of Brent FieldDocumento21 pagineThe Life Cycle of Brent FieldMalayan AjumovicNessuna valutazione finora
- ELS 15 Maret 2022 REVDocumento14 pagineELS 15 Maret 2022 REVhelto perdanaNessuna valutazione finora
- Crop Science SyllabusDocumento42 pagineCrop Science Syllabusbetty makushaNessuna valutazione finora
- Chapter5A TorqueDocumento32 pagineChapter5A TorqueShuq Faqat al-FansuriNessuna valutazione finora
- School of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Documento12 pagineSchool of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Pramod ShawNessuna valutazione finora
- CV - Mohsin FormatDocumento2 pagineCV - Mohsin FormatMuhammad Junaid IqbalNessuna valutazione finora
- Notes 3 Mineral Dressing Notes by Prof. SBS Tekam PDFDocumento3 pagineNotes 3 Mineral Dressing Notes by Prof. SBS Tekam PDFNikhil SinghNessuna valutazione finora
- You'Re My Everything - Glenn FredlyDocumento2 pagineYou'Re My Everything - Glenn FredlyTommy Juliansyah MarsenoNessuna valutazione finora
- Epson EcoTank ITS Printer L4150 DatasheetDocumento2 pagineEpson EcoTank ITS Printer L4150 DatasheetWebAntics.com Online Shopping StoreNessuna valutazione finora
- MODULE 8. Ceiling WorksDocumento2 pagineMODULE 8. Ceiling WorksAj MacalinaoNessuna valutazione finora
- Fortigate System Admin 40 Mr2Documento115 pagineFortigate System Admin 40 Mr2KhaleelNessuna valutazione finora
- Design of Ka-Band Low Noise Amplifier Using CMOS TechnologyDocumento6 pagineDesign of Ka-Band Low Noise Amplifier Using CMOS TechnologyEditor IJRITCCNessuna valutazione finora
- Install NoteDocumento1 paginaInstall NoteJose Ramon RozasNessuna valutazione finora
- MATLAB For Data VisualizationDocumento63 pagineMATLAB For Data Visualizationfahmi fawjiNessuna valutazione finora
- School Form 8 Grade 3Documento20 pagineSchool Form 8 Grade 3Mimi Ng PinasNessuna valutazione finora
- Proposal For A Working Procedure To Accurately Exchange Existing and New Calculated Protection Settings Between A TSO and Consulting CompaniesDocumento9 pagineProposal For A Working Procedure To Accurately Exchange Existing and New Calculated Protection Settings Between A TSO and Consulting CompaniesanonymNessuna valutazione finora
- Thesis Statement On Lionel MessiDocumento4 pagineThesis Statement On Lionel Messidwham6h1100% (2)
- PNP Loan Application Form February 2021 16Documento6 paginePNP Loan Application Form February 2021 16Wilhelm RegaladoNessuna valutazione finora
- New Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)Documento42 pagineNew Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)stan.isgod99Nessuna valutazione finora
- Blank Freeway Walls Replaced With Local Designs - Press EnterpriseDocumento5 pagineBlank Freeway Walls Replaced With Local Designs - Press EnterpriseEmmanuel Cuauhtémoc Ramos BarajasNessuna valutazione finora
- Majan Audit Report Final2Documento46 pagineMajan Audit Report Final2Sreekanth RallapalliNessuna valutazione finora
- Probset 3 KeyDocumento7 pagineProbset 3 KeyhoneyschuNessuna valutazione finora
- Project 2 Analysis of Florida WaterDocumento8 pagineProject 2 Analysis of Florida WaterBeau Beauchamp100% (1)
- Anglo Afghan WarsDocumento79 pagineAnglo Afghan WarsNisar AhmadNessuna valutazione finora
- TextdocumentDocumento254 pagineTextdocumentSaurabh SihagNessuna valutazione finora
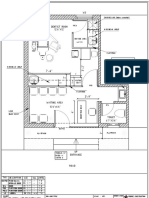
- Dental Clinic - Floor Plan R3-2Documento1 paginaDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)