Potrebbero piacerti anche
- A Case Report: Dept of Anesthesiology GGHDocumento10 pagineA Case Report: Dept of Anesthesiology GGHAhsan MohammedNessuna valutazione finora
- Carotid Sinus Massage - MuraliDocumento31 pagineCarotid Sinus Massage - MuraliAhsan MohammedNessuna valutazione finora
- Qualities of A Good CitizenDocumento12 pagineQualities of A Good Citizenmohammed jemal100% (1)
- 08CIV Chapter 05Documento59 pagine08CIV Chapter 05Ahsan MohammedNessuna valutazione finora
- Civic Duties Powerpoint 3Documento7 pagineCivic Duties Powerpoint 3the highest man in the chatNessuna valutazione finora
- B ScanDocumento135 pagineB ScanAhsan Mohammed75% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Robocon 2010 ReportDocumento46 pagineRobocon 2010 ReportDebal Saha100% (1)
- All Associates Warning Against ChangesDocumento67 pagineAll Associates Warning Against Changesramesh0% (1)
- Health Education and Health PromotionDocumento4 pagineHealth Education and Health PromotionRamela Mae SalvatierraNessuna valutazione finora
- Department of Education: Weekly Home Learning Plan Grade Ii Fourth Quarter Week 8Documento8 pagineDepartment of Education: Weekly Home Learning Plan Grade Ii Fourth Quarter Week 8Evelyn DEL ROSARIONessuna valutazione finora
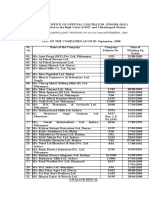
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Documento4 pagineStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20Nessuna valutazione finora
- Ana White - PLANS - A Murphy Bed YOU Can Build, and Afford To Build - 2011-03-03Documento20 pagineAna White - PLANS - A Murphy Bed YOU Can Build, and Afford To Build - 2011-03-03Ahmad KamilNessuna valutazione finora
- SWOT Analysis of Solar Energy in India: Abdul Khader.J Mohamed Idris.PDocumento4 pagineSWOT Analysis of Solar Energy in India: Abdul Khader.J Mohamed Idris.PSuhas VaishnavNessuna valutazione finora
- Chapter 2Documento22 pagineChapter 2Okorie Chinedu PNessuna valutazione finora
- Deluxe Force Gauge: Instruction ManualDocumento12 pagineDeluxe Force Gauge: Instruction ManualThomas Ramirez CastilloNessuna valutazione finora
- Positioning for competitive advantageDocumento9 paginePositioning for competitive advantageOnos Bunny BenjaminNessuna valutazione finora
- Desert Power India 2050Documento231 pagineDesert Power India 2050suraj jhaNessuna valutazione finora
- ROPE TENSIONER Product-Catalog-2019Documento178 pagineROPE TENSIONER Product-Catalog-2019jeedanNessuna valutazione finora
- SiBRAIN For PIC PIC18F57Q43 SchematicDocumento1 paginaSiBRAIN For PIC PIC18F57Q43 Schematicivanfco11Nessuna valutazione finora
- Human Resouse Accounting Nature and Its ApplicationsDocumento12 pagineHuman Resouse Accounting Nature and Its ApplicationsParas JainNessuna valutazione finora
- The Botanical AtlasDocumento74 pagineThe Botanical Atlasjamey_mork1100% (3)
- Honors Biology Unit 2 - Energy Study GuideDocumento2 pagineHonors Biology Unit 2 - Energy Study GuideMark RandolphNessuna valutazione finora
- 27 MARCH 2020: Assignment 5 Question PaperDocumento4 pagine27 MARCH 2020: Assignment 5 Question PaperShadreck SandweNessuna valutazione finora
- Unit 1 - Introduction To BankingDocumento17 pagineUnit 1 - Introduction To Bankingc08Nessuna valutazione finora
- Ks3 Science 2008 Level 5 7 Paper 1Documento28 pagineKs3 Science 2008 Level 5 7 Paper 1Saima Usman - 41700/TCHR/MGBNessuna valutazione finora
- The Learners Demonstrate An Understanding Of: The Learners Should Be Able To: The Learners Should Be Able ToDocumento21 pagineThe Learners Demonstrate An Understanding Of: The Learners Should Be Able To: The Learners Should Be Able ToBik Bok50% (2)
- Rhodes Motion For Judicial NoticeDocumento493 pagineRhodes Motion For Judicial Noticewolf woodNessuna valutazione finora
- Amar Sonar BanglaDocumento4 pagineAmar Sonar BanglaAliNessuna valutazione finora
- Tygon S3 E-3603: The Only Choice For Phthalate-Free Flexible TubingDocumento4 pagineTygon S3 E-3603: The Only Choice For Phthalate-Free Flexible TubingAluizioNessuna valutazione finora
- Emergency Room Delivery RecordDocumento7 pagineEmergency Room Delivery RecordMariel VillamorNessuna valutazione finora
- Common Size Analys3esDocumento5 pagineCommon Size Analys3esSaw Mee LowNessuna valutazione finora
- Amana PLE8317W2 Service ManualDocumento113 pagineAmana PLE8317W2 Service ManualSchneksNessuna valutazione finora
- Inventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Documento10 pagineInventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Wiro SablengNessuna valutazione finora
- 2007 Bomet District Paper 2Documento16 pagine2007 Bomet District Paper 2Ednah WambuiNessuna valutazione finora
- WWW - Istructe.pdf FIP UKDocumento4 pagineWWW - Istructe.pdf FIP UKBunkun15Nessuna valutazione finora
- Ali ExpressDocumento3 pagineAli ExpressAnsa AhmedNessuna valutazione finora