Potrebbero piacerti anche
- Bagpipe LV 1-5Documento228 pagineBagpipe LV 1-5Sathia Kdms100% (2)
- Kaged Muscle Magazine Issue 1Documento41 pagineKaged Muscle Magazine Issue 1hashimhafiz1100% (1)
- Reynold A. Nicholson - The Mystics of IslamDocumento65 pagineReynold A. Nicholson - The Mystics of IslamLuminon SamanNessuna valutazione finora
- Synthesis Essay Coming To Grips With GenesisDocumento11 pagineSynthesis Essay Coming To Grips With Genesisapi-259381516Nessuna valutazione finora
- Multi Organ Dysfunction SyndromeDocumento40 pagineMulti Organ Dysfunction SyndromeDr. Jayesh PatidarNessuna valutazione finora
- Kehamilan MolaDocumento88 pagineKehamilan MolaYhanna UlfianiNessuna valutazione finora
- Gestational Trophoblastic DiseaseDocumento40 pagineGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- Managing Placenta Accreta: Incidence and PathophysiologyDocumento9 pagineManaging Placenta Accreta: Incidence and PathophysiologyAslesa Wangpathi PagehgiriNessuna valutazione finora
- GTD Case StudyDocumento9 pagineGTD Case StudyZnarf Izlah Sadanreb100% (1)
- Compiled LecsDocumento24 pagineCompiled LecsNur SetsuNessuna valutazione finora
- Gestational Trophoblastic Disease (GTD) Part I: Molar PregnancyDocumento88 pagineGestational Trophoblastic Disease (GTD) Part I: Molar Pregnancyhafidzz1100% (1)
- Gestational Trophoblastic Disease (GTD) : MWU Department of Obs & Gyn, DR - Mohammed HDocumento54 pagineGestational Trophoblastic Disease (GTD) : MWU Department of Obs & Gyn, DR - Mohammed HSisay FentaNessuna valutazione finora
- Ovarian TorsiDocumento8 pagineOvarian TorsiSebastian GandyNessuna valutazione finora
- Ectopic PregnancyDocumento34 pagineEctopic Pregnancyannu panchalNessuna valutazione finora
- CP Hydatidiform MoleDocumento13 pagineCP Hydatidiform Molesweetheart_joannieNessuna valutazione finora
- Salivary Gland 2001 01Documento36 pagineSalivary Gland 2001 01theibban89Nessuna valutazione finora
- H Mole Case PresentationDocumento12 pagineH Mole Case PresentationjisooNessuna valutazione finora
- John Tidy: 21 The Role of Surgery in The Management of Gestational Trophoblastic DiseaseDocumento17 pagineJohn Tidy: 21 The Role of Surgery in The Management of Gestational Trophoblastic DiseaseRana RaydianNessuna valutazione finora
- Antepartum Haemorrhage: Learning ObjectivesDocumento12 pagineAntepartum Haemorrhage: Learning Objectivesياسر كوثر هانيNessuna valutazione finora
- Antepartum HemorrhageDocumento12 pagineAntepartum HemorrhageMohammed AbdNessuna valutazione finora
- Mola Hidatidosa NcbiDocumento4 pagineMola Hidatidosa NcbiRekno DwiNessuna valutazione finora
- CDH Modern MXDocumento11 pagineCDH Modern MXphobicmdNessuna valutazione finora
- Hydatidiform Mole: AuthorsDocumento7 pagineHydatidiform Mole: AuthorsIdo KurniawanNessuna valutazione finora
- Ectopic PregnancyDocumento39 pagineEctopic PregnancyFecky Fihayatul IchsanNessuna valutazione finora
- Jurnal Mola HidatidosaDocumento8 pagineJurnal Mola HidatidosaDebby SofianaNessuna valutazione finora
- 9.5 Hydatidiform Mole: 9 Abnormalities of Early PregnancyDocumento6 pagine9.5 Hydatidiform Mole: 9 Abnormalities of Early PregnancyIssa HalifaNessuna valutazione finora
- Diagnosis and Treatment of Gestational Trophoblastic Disease PDFDocumento11 pagineDiagnosis and Treatment of Gestational Trophoblastic Disease PDFAlexeySAgNessuna valutazione finora
- Anesthetic Considerations in HELLP Syndrome PDFDocumento14 pagineAnesthetic Considerations in HELLP Syndrome PDFGustavo ParedesNessuna valutazione finora
- Ectopic Pregnancy6Documento47 pagineEctopic Pregnancy6Muhammad AbeeshNessuna valutazione finora
- Transient Thyrotoxicosis in Molar PregnancyDocumento2 pagineTransient Thyrotoxicosis in Molar PregnancyWilliam OttoNessuna valutazione finora
- Tubalpregnancy DiagnosisandmanagementDocumento12 pagineTubalpregnancy DiagnosisandmanagementAndreaAlexandraNessuna valutazione finora
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocumento4 pagineEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyFebrinata MahadikaNessuna valutazione finora
- Tubo - Ovarian ProcessDocumento7 pagineTubo - Ovarian ProcessRosel RomarateNessuna valutazione finora
- Chemical Pleurodesis For Malignant Pleural EffusionDocumento6 pagineChemical Pleurodesis For Malignant Pleural EffusiondarmariantoNessuna valutazione finora
- Tse 2012Documento14 pagineTse 2012alexg_298379Nessuna valutazione finora
- Kobayashi 2014Documento7 pagineKobayashi 2014Mauricio Lopez MejiaNessuna valutazione finora
- Benign Gestational Trophoblastic DiseaseDocumento31 pagineBenign Gestational Trophoblastic Diseaseبسيل أبوهلالNessuna valutazione finora
- Guideline AUB 1 PDFDocumento6 pagineGuideline AUB 1 PDFzahrara90Nessuna valutazione finora
- Consumptive CoagulopathyDocumento20 pagineConsumptive Coagulopathyilvan yanuarNessuna valutazione finora
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocumento16 pagineWorld's Largest Science, Technology & Medicine Open Access Book PublisherdkasisNessuna valutazione finora
- Gestational Trophoblastic DiseaseDocumento6 pagineGestational Trophoblastic DiseaseSJ IraaNessuna valutazione finora
- BR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older ChildrenDocumento45 pagineBR J Haematol - 2016 - New - Guidelines On Transfusion For Fetuses Neonates and Older Childrensanjeev kumarNessuna valutazione finora
- Causes: Gestational Trophoblastic Disease ChoriocarcinomaDocumento7 pagineCauses: Gestational Trophoblastic Disease ChoriocarcinomajudssalangsangNessuna valutazione finora
- Polyhydramnios Sem5Documento9 paginePolyhydramnios Sem5Siti Nur AmirahNessuna valutazione finora
- Mini-Review: Neonatal PolycythaemiaDocumento3 pagineMini-Review: Neonatal PolycythaemiaElizabeth HendersonNessuna valutazione finora
- Vanderpol 2016Documento6 pagineVanderpol 2016Andy esNessuna valutazione finora
- Ectopic Pregnancy - MedscapeDocumento31 pagineEctopic Pregnancy - Medscapeantonio91uNessuna valutazione finora
- Untitled 1Documento16 pagineUntitled 1Nita Corry AgustineNessuna valutazione finora
- Advancesinsurgeryfor Abdominalwalldefects: Gastroschisis and OmphaloceleDocumento12 pagineAdvancesinsurgeryfor Abdominalwalldefects: Gastroschisis and OmphaloceleSitti HazrinaNessuna valutazione finora
- Ectopic Pregnancy22Documento43 pagineEctopic Pregnancy22Sunil YadavNessuna valutazione finora
- Nipple Discharge 3Documento3 pagineNipple Discharge 3Dima PathNessuna valutazione finora
- EG0800339 Hyperhomocysteinemia in Recurrent Miscarriage: Kh. R. Gaber, M. K. Farag, S. ET. Soliman, M. A. Abd Al-KaderDocumento6 pagineEG0800339 Hyperhomocysteinemia in Recurrent Miscarriage: Kh. R. Gaber, M. K. Farag, S. ET. Soliman, M. A. Abd Al-KaderElena VisterniceanNessuna valutazione finora
- Polyhydramnios An UpdateDocumento7 paginePolyhydramnios An UpdateGenio RachmadanaNessuna valutazione finora
- BR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortDocumento9 pagineBR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortJustine ObedNessuna valutazione finora
- Trial of Labor Compared With Elective Cesarean.12Documento10 pagineTrial of Labor Compared With Elective Cesarean.12Herman FiraNessuna valutazione finora
- Amniotic FluidsDocumento7 pagineAmniotic FluidsMazlina MaidinNessuna valutazione finora
- New Et Al-2016-British Journal of HaematologyDocumento45 pagineNew Et Al-2016-British Journal of HaematologyClara Bordes GarcíaNessuna valutazione finora
- Chapter 10Documento9 pagineChapter 10Kanishka SamantaNessuna valutazione finora
- E MedicineDocumento10 pagineE MedicineAnggie Pradetya MaharaniNessuna valutazione finora
- Histological Diagnosis of Hydatidiform Moles: Histological Changes of Complete and Partial Moles AreDocumento8 pagineHistological Diagnosis of Hydatidiform Moles: Histological Changes of Complete and Partial Moles AreClareen JuanicoNessuna valutazione finora
- Amniotic Fluid Embolism ArticleDocumento3 pagineAmniotic Fluid Embolism ArticleShailesh JainNessuna valutazione finora
- Hydatidiform Mole: BackgroundDocumento11 pagineHydatidiform Mole: BackgroundIlham TaufanNessuna valutazione finora
- Comparison of Transverse and Vertical Skin Incision ForDocumento6 pagineComparison of Transverse and Vertical Skin Incision ForHerry SasukeNessuna valutazione finora
- Cystic FibrosisDocumento69 pagineCystic Fibrosisprapul vankaraNessuna valutazione finora
- 2016 Neonates FinalDocumento91 pagine2016 Neonates FinalherryNessuna valutazione finora
- Gestational Trophoblastic Disease Guideline 12.507Documento9 pagineGestational Trophoblastic Disease Guideline 12.507Issa HalifaNessuna valutazione finora
- 9.5 Hydatidiform Mole: 9 Abnormalities of Early PregnancyDocumento6 pagine9.5 Hydatidiform Mole: 9 Abnormalities of Early PregnancyIssa HalifaNessuna valutazione finora
- Parotid, Submand - Gl.Documento26 pagineParotid, Submand - Gl.Issa HalifaNessuna valutazione finora
- Technical Data Sheet: LPI HVSC PlusDocumento2 pagineTechnical Data Sheet: LPI HVSC PlusNguyễn TấnNessuna valutazione finora
- Practice For Mounting Buses & Joints-374561Documento11 paginePractice For Mounting Buses & Joints-374561a_sengar1Nessuna valutazione finora
- Child DevelopmentDocumento15 pagineChild Development4AndreeaNessuna valutazione finora
- Reading Part 2Documento14 pagineReading Part 2drama channelNessuna valutazione finora
- Automatic Train OperationDocumento6 pagineAutomatic Train OperationAnupam KhandelwalNessuna valutazione finora
- Physics Unit 11 NotesDocumento26 paginePhysics Unit 11 Notesp.salise352Nessuna valutazione finora
- Psle Science Keywords !Documento12 paginePsle Science Keywords !Aftertea CarousellNessuna valutazione finora
- OPTCL-Fin-Bhw-12Documento51 pagineOPTCL-Fin-Bhw-12Bimal Kumar DashNessuna valutazione finora
- Us Navy To Evaluate Anti Submarine Warfare Training SystemDocumento2 pagineUs Navy To Evaluate Anti Submarine Warfare Training SystemVictor PileggiNessuna valutazione finora
- Ruhangawebare Kalemera Godfrey Thesis PDFDocumento116 pagineRuhangawebare Kalemera Godfrey Thesis PDFYoobsan Tamiru TTolaaNessuna valutazione finora
- ETR Series: A Full Spectrum of Products To Solve Your Application NeedsDocumento106 pagineETR Series: A Full Spectrum of Products To Solve Your Application Needs周小安Nessuna valutazione finora
- Veronte Autopilot Kit DatasheetDocumento2 pagineVeronte Autopilot Kit DatasheetEkmedzicNessuna valutazione finora
- Ecall Vs NG EcallDocumento6 pagineEcall Vs NG EcallTrần Văn DũngNessuna valutazione finora
- 988611457NK448908 Vehicle Scan ReportDocumento5 pagine988611457NK448908 Vehicle Scan ReportVictor Daniel Piñeros ZubietaNessuna valutazione finora
- Eco Exercise 3answer Ans 1Documento8 pagineEco Exercise 3answer Ans 1Glory PrintingNessuna valutazione finora
- Test 8 D - Unit 2Documento3 pagineTest 8 D - Unit 2IONELA MIHAELA POPANessuna valutazione finora
- Investigation of Skew Curved Bridges in Combination With Skewed Abutments Under Seismic ResponseDocumento5 pagineInvestigation of Skew Curved Bridges in Combination With Skewed Abutments Under Seismic ResponseEditor IJTSRDNessuna valutazione finora
- Assessment of Diabetic FootDocumento7 pagineAssessment of Diabetic FootChathiya Banu KrishenanNessuna valutazione finora
- Birla MEEP Op ManualDocumento43 pagineBirla MEEP Op ManualAshok ChettiyarNessuna valutazione finora
- Welcome To Our 2Nd Topic: History of VolleyballDocumento6 pagineWelcome To Our 2Nd Topic: History of VolleyballDharyn KhaiNessuna valutazione finora
- Azure Machine Learning StudioDocumento17 pagineAzure Machine Learning StudioNurain IsmailNessuna valutazione finora
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDocumento2 pagineRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNessuna valutazione finora
- Đề 17Documento11 pagineĐề 17Nguyen CuongNessuna valutazione finora
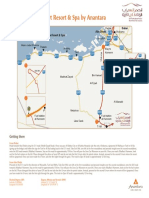
- Qasr Al Sarab Desert Resort Location Map June2012Documento1 paginaQasr Al Sarab Desert Resort Location Map June2012Anant GârgNessuna valutazione finora