Potrebbero piacerti anche
- Human Factors in Surgery: Enhancing Safety and Flow in Patient CareDa EverandHuman Factors in Surgery: Enhancing Safety and Flow in Patient CareTara N. CohenNessuna valutazione finora
- Risk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsDa EverandRisk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsNessuna valutazione finora
- Basic Principles of Patient Safety-Overview-Self-Study Module-2013 PDFDocumento35 pagineBasic Principles of Patient Safety-Overview-Self-Study Module-2013 PDFfmta100% (1)
- Adverse Event: Wirsma Arif Harahap Surgical OncologistDocumento49 pagineAdverse Event: Wirsma Arif Harahap Surgical OncologistAhmad Fakhrozi HelmiNessuna valutazione finora
- Patient Safety: Suryani Yuliyanti FK UnissulaDocumento69 paginePatient Safety: Suryani Yuliyanti FK UnissulaaliNessuna valutazione finora
- Patient Safety: Suryani Yuliyanti FK UnissulaDocumento70 paginePatient Safety: Suryani Yuliyanti FK UnissulaHanarine Wijadja100% (1)
- 2 Faktor Kecelakaan Praktek Anestesi Di Kamar Bedah Rev Aprl 09Documento42 pagine2 Faktor Kecelakaan Praktek Anestesi Di Kamar Bedah Rev Aprl 09rokhmantoNessuna valutazione finora
- 15 QsDocumento4 pagine15 Qsujangketul62Nessuna valutazione finora
- Technology in Nursing Final PaperDocumento15 pagineTechnology in Nursing Final Paperapi-272621489Nessuna valutazione finora
- Lecture 10 Patient Safety and TechnologyDocumento86 pagineLecture 10 Patient Safety and TechnologyHussein ShamiNessuna valutazione finora
- Reducing False Alarms in Intensive Care Units: A Scoping ReviewDocumento8 pagineReducing False Alarms in Intensive Care Units: A Scoping ReviewPASANTIA UAONessuna valutazione finora
- Patient Safety and Quality Improvement 101Documento81 paginePatient Safety and Quality Improvement 101Manasi PandaNessuna valutazione finora
- 3, Patient Safety - Dr. Santoso S., Spa, MarsDocumento55 pagine3, Patient Safety - Dr. Santoso S., Spa, Marsendang wildayaniNessuna valutazione finora
- Patientsafety-200908151455 PPT Jino UpdatedDocumento27 paginePatientsafety-200908151455 PPT Jino UpdatedjinoNessuna valutazione finora
- Awareness and Prevention of Error in Clinical Decision MakingDocumento4 pagineAwareness and Prevention of Error in Clinical Decision MakingJASMIN RNNessuna valutazione finora
- Systems and Medical Error DidacticsDocumento29 pagineSystems and Medical Error DidacticsBisakha DeyNessuna valutazione finora
- Medical Mistakes Jordan Keith 1Documento7 pagineMedical Mistakes Jordan Keith 1api-451579732Nessuna valutazione finora
- Falls Sustained During Inpatient Rehabilitation After Lower Limb Amputation Prevalence and PredictorsDocumento12 pagineFalls Sustained During Inpatient Rehabilitation After Lower Limb Amputation Prevalence and PredictorsFaeyz OrabiNessuna valutazione finora
- Errors Fall Into Predictable Patterns Communication Planning ExecutionDocumento25 pagineErrors Fall Into Predictable Patterns Communication Planning ExecutionMilan GajeraNessuna valutazione finora
- Konsep SBLDocumento30 pagineKonsep SBLkeperawatancileungsiNessuna valutazione finora
- Graling, Sanchez - 2017 - Learning and Mindfulness Improving Perioperative Patient SafetyDocumento5 pagineGraling, Sanchez - 2017 - Learning and Mindfulness Improving Perioperative Patient SafetyDave SainsburyNessuna valutazione finora
- Eip First DraftDocumento10 pagineEip First Draftapi-338437548Nessuna valutazione finora
- Expert Laboratory Information SystemsDocumento8 pagineExpert Laboratory Information SystemsVeera ManickamNessuna valutazione finora
- Wrong Site Surgery PaperDocumento18 pagineWrong Site Surgery Paperapi-297065332Nessuna valutazione finora
- Medical Errors, Negligence, and LitigationDocumento54 pagineMedical Errors, Negligence, and LitigationEman ElmahdyNessuna valutazione finora
- Occupational Hazards in Health Care ProfessionalsDocumento33 pagineOccupational Hazards in Health Care Professionalsdocshirin100% (1)
- Reducing Human Error QPDocumento10 pagineReducing Human Error QPPradeepNessuna valutazione finora
- Root Cause AnalysisDocumento6 pagineRoot Cause Analysisapi-317112295100% (1)
- Patient SafetyDocumento133 paginePatient Safetydrabhimanyu_b6956100% (1)
- 2015 AsaDocumento136 pagine2015 AsaFrits Dede SinagaNessuna valutazione finora
- Medication Errors: by DR Bharat MalhotraDocumento36 pagineMedication Errors: by DR Bharat MalhotraASHISH KUMAR YADAVNessuna valutazione finora
- Patient SafetyDocumento92 paginePatient Safetywiwid0% (1)
- JC Frailty As A Risk Predictor in Cardiac SurgeryDocumento30 pagineJC Frailty As A Risk Predictor in Cardiac SurgeryFaizan Ahmad AliNessuna valutazione finora
- Patient Safety: What Should We Be Trying To Communicate?Documento32 paginePatient Safety: What Should We Be Trying To Communicate?cicaklomenNessuna valutazione finora
- Patient SafetyDocumento19 paginePatient SafetyDudang Erawan Suseno100% (1)
- FMT001 Prevention of Medical ErrorsDocumento43 pagineFMT001 Prevention of Medical ErrorsgailgonesouthNessuna valutazione finora
- Radiation Oncology Incident Learning SystemDocumento4 pagineRadiation Oncology Incident Learning Systemapi-484763634Nessuna valutazione finora
- The Swollen Extremit A Systematic Approach To The Evaluation of A Common ComplaintDocumento28 pagineThe Swollen Extremit A Systematic Approach To The Evaluation of A Common ComplaintnyjonesNessuna valutazione finora
- Human Error in Anaesthesia: Whose Fault Is It Anyway?: Protective Ventilation in The ORDocumento9 pagineHuman Error in Anaesthesia: Whose Fault Is It Anyway?: Protective Ventilation in The ORNadia UlmeanuNessuna valutazione finora
- RoilsDocumento4 pagineRoilsapi-585462575Nessuna valutazione finora
- Cohoon 2011Documento15 pagineCohoon 2011abroud.amina.999Nessuna valutazione finora
- Safety Part 1 Culture Lesson Patient Safety Human FactorsDocumento54 pagineSafety Part 1 Culture Lesson Patient Safety Human FactorsMaria Victoria A. PraxidesNessuna valutazione finora
- 1.what Is Patient Safety 6th March, 2023Documento32 pagine1.what Is Patient Safety 6th March, 2023hum JavedNessuna valutazione finora
- Hopkins ThesisDocumento5 pagineHopkins ThesisWriterPaperSingapore100% (2)
- Kuliah Patient Safety 3 Oktober 2014Documento63 pagineKuliah Patient Safety 3 Oktober 2014Ridho Frihadananta WardhanaNessuna valutazione finora
- Patient Safety (Keselamatan Pasien)Documento92 paginePatient Safety (Keselamatan Pasien)Siti SalasiahNessuna valutazione finora
- Operating Room EnviromentDocumento8 pagineOperating Room EnviromentBruno AlcaldeNessuna valutazione finora
- Ophthalmologic EmergenciesDocumento241 pagineOphthalmologic Emergenciesسہاجہدةه لہلہهNessuna valutazione finora
- Patients Benefit While Surgeons Suffer: An Impending EpidemicDocumento8 paginePatients Benefit While Surgeons Suffer: An Impending EpidemicMiguel Fernando ALban VasquezNessuna valutazione finora
- Research Proposal Final Edit 1Documento5 pagineResearch Proposal Final Edit 1api-484027891Nessuna valutazione finora
- Introduction - JackyDocumento35 pagineIntroduction - JackyJackylou B Tuballes RrtNessuna valutazione finora
- Common Occupational DisordersDocumento9 pagineCommon Occupational DisordersDinesh ReddyNessuna valutazione finora
- Safety Ketepatan Pengelolaan KesalahanDocumento184 pagineSafety Ketepatan Pengelolaan KesalahannadyaNessuna valutazione finora
- Relationship BetweenvolemwDocumento6 pagineRelationship Betweenvolemwcandra wNessuna valutazione finora
- Brief History of Patient Safety Culture and ScienceDocumento4 pagineBrief History of Patient Safety Culture and ScienceHoli100% (1)
- PT - 1980 220X Reeusp 52 E03406Documento8 paginePT - 1980 220X Reeusp 52 E03406Carlos MullerNessuna valutazione finora
- Chapter 12 - Patient Safety - APIC Text OnlineDocumento30 pagineChapter 12 - Patient Safety - APIC Text OnlineManalAbdelazizNessuna valutazione finora
- Repetitive Strain Injury LANCET 2007Documento8 pagineRepetitive Strain Injury LANCET 2007Alfredo Luiz CostaNessuna valutazione finora
- Continuous Quality Improvements and SafetyDocumento3 pagineContinuous Quality Improvements and Safetyapi-518020510Nessuna valutazione finora
- 12 Strokes: A Case-based Guide to Acute Ischemic Stroke ManagementDa Everand12 Strokes: A Case-based Guide to Acute Ischemic Stroke ManagementFerdinand K. HuiNessuna valutazione finora
- Aeloiza - Matus-Analysis and Design of New Harmonic Mitigation ApproachesDocumento180 pagineAeloiza - Matus-Analysis and Design of New Harmonic Mitigation ApproachesAnonymous NGXdt2BxNessuna valutazione finora
- Some Notes On Three-Phase Transformers Olaf Lyngdahl OlsenDocumento44 pagineSome Notes On Three-Phase Transformers Olaf Lyngdahl OlsenAnonymous NGXdt2BxNessuna valutazione finora
- The Effect of Design Features On Centrifugal Pump EfficiencyDocumento5 pagineThe Effect of Design Features On Centrifugal Pump EfficiencyAnonymous NGXdt2BxNessuna valutazione finora
- Moody DiagramDocumento1 paginaMoody DiagramAnonymous NGXdt2BxNessuna valutazione finora
- Backwater CurvesDocumento38 pagineBackwater Curvesdist2235Nessuna valutazione finora
- Power Electronics in Electricity To IEC61000-3-13Documento310 paginePower Electronics in Electricity To IEC61000-3-13Anonymous NGXdt2BxNessuna valutazione finora
- 61rl97 - Strongly Buoyant Plume Similarity and 'Small Fire' VentilationDocumento24 pagine61rl97 - Strongly Buoyant Plume Similarity and 'Small Fire' VentilationAnonymous NGXdt2BxNessuna valutazione finora
- Electrical Safety - 8Documento52 pagineElectrical Safety - 8Anonymous NGXdt2BxNessuna valutazione finora
- Increasing Induction Motor Drives Efficiency - Understanding The Pitfalls - BelmansDocumento17 pagineIncreasing Induction Motor Drives Efficiency - Understanding The Pitfalls - BelmansAnonymous NGXdt2BxNessuna valutazione finora
- CMFF09WS MTA4 SheardetalDocumento9 pagineCMFF09WS MTA4 SheardetalAnonymous NGXdt2BxNessuna valutazione finora
- K Principles of Short-Circuiting For Human ProtectionDocumento1 paginaK Principles of Short-Circuiting For Human ProtectionAnonymous NGXdt2BxNessuna valutazione finora
- 001 Presentation Martin DoppelbauerDocumento18 pagine001 Presentation Martin DoppelbauerAnonymous NGXdt2BxNessuna valutazione finora
- Microsoft PowerPoint - Motor Protection Principles 101308.Ppt - Motor Protection PrinciplesDocumento35 pagineMicrosoft PowerPoint - Motor Protection Principles 101308.Ppt - Motor Protection PrinciplesPaneendra Kumar0% (1)
- Electrical Safety - 8Documento52 pagineElectrical Safety - 8Anonymous NGXdt2BxNessuna valutazione finora
- Michael Kilby Systems & Rolling Stock Manager Fireworthiness - An Integrated Solution 11 March 2009Documento38 pagineMichael Kilby Systems & Rolling Stock Manager Fireworthiness - An Integrated Solution 11 March 2009Anonymous NGXdt2BxNessuna valutazione finora
- Study On Comfort FansDocumento99 pagineStudy On Comfort FansAnonymous NGXdt2Bx100% (1)
- 1045 McDaid - Pushing The BoundariesDocumento35 pagine1045 McDaid - Pushing The BoundariesAnonymous NGXdt2BxNessuna valutazione finora
- Roff Venting of Burning Enclosures - FRN-0419Documento30 pagineRoff Venting of Burning Enclosures - FRN-0419Anonymous NGXdt2BxNessuna valutazione finora
- Efficient Extraction of Smoke From A Thin Layer Under A Ceiling - FRN-1001Documento20 pagineEfficient Extraction of Smoke From A Thin Layer Under A Ceiling - FRN-1001Anonymous NGXdt2BxNessuna valutazione finora
- En 12101 344 Powered Smoke Exhaust SystemsDocumento6 pagineEn 12101 344 Powered Smoke Exhaust SystemspsmanasseNessuna valutazione finora
- 003 AC RadialDocumento92 pagine003 AC RadialAnonymous NGXdt2BxNessuna valutazione finora
- A Study On The Characteristics of Smoke Control Using Lower Part Pressurization With An Opening in A Large Scale SpaceDocumento9 pagineA Study On The Characteristics of Smoke Control Using Lower Part Pressurization With An Opening in A Large Scale SpaceAnonymous NGXdt2BxNessuna valutazione finora
- 025 Kanchan Finalpaper EEMODS13Documento17 pagine025 Kanchan Finalpaper EEMODS13Anonymous NGXdt2BxNessuna valutazione finora
- Roof Venting. of Burning Enclosures II - Frn-0391Documento12 pagineRoof Venting. of Burning Enclosures II - Frn-0391Anonymous NGXdt2BxNessuna valutazione finora
- 'Protecting Escape Routes - Smoke Shafts V Pressurisation' - Means of Escape - Fire Safety MagazineDocumento6 pagine'Protecting Escape Routes - Smoke Shafts V Pressurisation' - Means of Escape - Fire Safety MagazineAnonymous NGXdt2BxNessuna valutazione finora
- 01 - Dynamic and Real Time Modelling Rob CaseyDocumento16 pagine01 - Dynamic and Real Time Modelling Rob CaseyAnonymous NGXdt2BxNessuna valutazione finora
- 001 Presentation Martin DoppelbauerDocumento18 pagine001 Presentation Martin DoppelbauerAnonymous NGXdt2BxNessuna valutazione finora
- Understanding EMC Basics Webinar 3 of 3 HandoutDocumento6 pagineUnderstanding EMC Basics Webinar 3 of 3 HandoutAnonymous NGXdt2BxNessuna valutazione finora
- 'Protecting Escape Routes - Smoke Shafts V Pressurisation' - Means of Escape - Fire Safety MagazineDocumento6 pagine'Protecting Escape Routes - Smoke Shafts V Pressurisation' - Means of Escape - Fire Safety MagazineAnonymous NGXdt2BxNessuna valutazione finora
- Understanding EMC Basics Webinar 2 of 3 HandoutDocumento8 pagineUnderstanding EMC Basics Webinar 2 of 3 HandoutAnonymous NGXdt2BxNessuna valutazione finora
- Zoll M Series Defibrillator Manual PDFDocumento111 pagineZoll M Series Defibrillator Manual PDFAhmad TanveerNessuna valutazione finora
- Cardiac DefibrillatorsDocumento8 pagineCardiac Defibrillatorsصفا طلال نايفNessuna valutazione finora
- LAFD Field ManualDocumento122 pagineLAFD Field Manualfumptfxn50% (4)
- Pediatric Emergency Assessment Recognition and StabilizationDocumento182 paginePediatric Emergency Assessment Recognition and StabilizationFernando Arancibia100% (2)
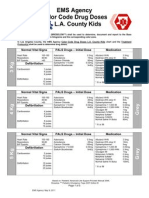
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocumento5 pagineEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNessuna valutazione finora
- Manual of M8000 Veterinary MonitorDocumento151 pagineManual of M8000 Veterinary MonitorCIBMEDICS SASNessuna valutazione finora
- PALS Case Scenario Testing ChecklistDocumento12 paginePALS Case Scenario Testing ChecklistJohn David D. ErguizaNessuna valutazione finora
- The Hong Kong College of Anaesthesiologists Final Fellowship Examination March/May 2006 Examiners ReportDocumento10 pagineThe Hong Kong College of Anaesthesiologists Final Fellowship Examination March/May 2006 Examiners ReportJane KoNessuna valutazione finora
- Makalah Infant Warmer2Documento11 pagineMakalah Infant Warmer2RaffyNessuna valutazione finora
- WHATs New in CPCRDocumento4 pagineWHATs New in CPCRJessicaHernandezNessuna valutazione finora
- VSP PDFDocumento62 pagineVSP PDFMisha KulibaevNessuna valutazione finora
- 10 - Manual Servicio - Nihon Kohden OPV-1500Documento111 pagine10 - Manual Servicio - Nihon Kohden OPV-1500pirihuey1234Nessuna valutazione finora
- QynetiQ Enterprise - User Manual 1.5 (EN) PDFDocumento122 pagineQynetiQ Enterprise - User Manual 1.5 (EN) PDFUlly Rochaya PrabandariNessuna valutazione finora
- VCDocumento147 pagineVCSerjNessuna valutazione finora
- 2021 ACLS Study GuideDocumento20 pagine2021 ACLS Study GuideShane Brown83% (12)
- All Product CatalogueDocumento48 pagineAll Product CatalogueyashwanthbnyashwanthNessuna valutazione finora
- Cardiac Arrest InfographicDocumento2 pagineCardiac Arrest InfographicStef DygaNessuna valutazione finora
- Spek Ecatalog LKPP - Baru PDFDocumento68 pagineSpek Ecatalog LKPP - Baru PDFHendra Mokoginta LieNessuna valutazione finora
- Advanced Cardiac Life Support (ACLS)Documento17 pagineAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNessuna valutazione finora
- ACLS Provider Manual PDFDocumento63 pagineACLS Provider Manual PDFRiley Escobar100% (1)
- Oag Report - Putnam CountyDocumento84 pagineOag Report - Putnam CountyJon CampbellNessuna valutazione finora
- f6 User ManualDocumento104 paginef6 User ManualSreejith SwaminathanNessuna valutazione finora
- 2013 State of Oklahoma EMS ProtocolsDocumento493 pagine2013 State of Oklahoma EMS ProtocolsMarian Ioan-Lucian100% (1)
- Quick Hits For Pediatric Emergency Medicine Zeretzke Bien 2 Ed 2023Documento195 pagineQuick Hits For Pediatric Emergency Medicine Zeretzke Bien 2 Ed 2023kabulkabulovich5Nessuna valutazione finora
- UntitledDocumento42 pagineUntitledapi-867493550% (1)
- Shinova DM8D Defibrillator - User ManualDocumento63 pagineShinova DM8D Defibrillator - User Manualhüseyin vururNessuna valutazione finora
- END ERA: of AnDocumento16 pagineEND ERA: of AnKarthikNessuna valutazione finora
- Zoll E-Series - Service ManualsDocumento96 pagineZoll E-Series - Service ManualsCristian CamiloNessuna valutazione finora
- Crash Cart Inventory ListDocumento2 pagineCrash Cart Inventory ListSalah ElbadawyNessuna valutazione finora
- CPR MCQ 02Documento19 pagineCPR MCQ 02Ryam Taif100% (1)