Potrebbero piacerti anche
- Smoller Et Al-2008-American Journal of Medical Genetics Part C - Seminars in Medical Genetics PDFDocumento9 pagineSmoller Et Al-2008-American Journal of Medical Genetics Part C - Seminars in Medical Genetics PDFJeannie WalshNessuna valutazione finora
- Epidemiology of SchizophreniaDocumento13 pagineEpidemiology of SchizophreniaSri AgustinaNessuna valutazione finora
- Schizophrenia A Concise Overview of Incidence, Prevalence, and MortalityDocumento10 pagineSchizophrenia A Concise Overview of Incidence, Prevalence, and MortalitySri AgustinaNessuna valutazione finora
- Social AnxietyDocumento21 pagineSocial AnxietyRini DewiNessuna valutazione finora
- Becker 2007Documento6 pagineBecker 2007Stroe EmmaNessuna valutazione finora
- Intentos Suicidas en EEUU en Pacientes Con Diagnosticos de TCA Segun DSM-VDocumento13 pagineIntentos Suicidas en EEUU en Pacientes Con Diagnosticos de TCA Segun DSM-Vsamira6alvarado6zebaNessuna valutazione finora
- Dimensions of Anxiety Symptoms in Romanian Young Adult Subjects From Brasov CountyDocumento4 pagineDimensions of Anxiety Symptoms in Romanian Young Adult Subjects From Brasov CountylmplmpNessuna valutazione finora
- McElroy Et Al. (2016)Documento11 pagineMcElroy Et Al. (2016)voooNessuna valutazione finora
- The Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsDocumento7 pagineThe Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsGeorge WinchesterNessuna valutazione finora
- Prevalence of Depression and Anxiety in SLE PDFDocumento14 paginePrevalence of Depression and Anxiety in SLE PDFRidho PratamaNessuna valutazione finora
- A Systematic Review of The Mortality of DepressionDocumento12 pagineA Systematic Review of The Mortality of Depressionadri90Nessuna valutazione finora
- Course of OCDDocumento16 pagineCourse of OCDShwetank BansalNessuna valutazione finora
- Epidemiological Surveys of Autism and Other Pervasive Developmental Disorders: An UpdateDocumento18 pagineEpidemiological Surveys of Autism and Other Pervasive Developmental Disorders: An UpdatepipejaramilloNessuna valutazione finora
- Duration of Depressive Symptoms and Mortality Risk The English Longitudinal Study of Ageing ElsaDocumento6 pagineDuration of Depressive Symptoms and Mortality Risk The English Longitudinal Study of Ageing ElsaAishwarya PuttaNessuna valutazione finora
- Personality disorder global perspectiveDocumento5 paginePersonality disorder global perspectiveAmalia PutriNessuna valutazione finora
- Attention Bias Modification Treatment For Adolescents With Social Anxiety DisorderDocumento6 pagineAttention Bias Modification Treatment For Adolescents With Social Anxiety DisorderMarc TermoNessuna valutazione finora
- Marital Status and Risk For Late LifeDocumento13 pagineMarital Status and Risk For Late LifeHargo PsyNessuna valutazione finora
- Beesdo Baum2012Documento15 pagineBeesdo Baum2012akzarajuwanaparastiaraNessuna valutazione finora
- Neuroasia 2013 18 (3) 231Documento8 pagineNeuroasia 2013 18 (3) 231Marcus Wong KSNessuna valutazione finora
- Anxiety Disorders in WomenDocumento52 pagineAnxiety Disorders in WomenZakkiyatus Zainiyah100% (1)
- Out 11Documento13 pagineOut 11Etika Tunjung KencanaNessuna valutazione finora
- Prevalence of Personality Disorders in The General Adult Population in Western Countries Systematic Review and Meta AnalysisDocumento7 paginePrevalence of Personality Disorders in The General Adult Population in Western Countries Systematic Review and Meta AnalysisFavio AndradeNessuna valutazione finora
- Epidemiology of PTSD Version 3Documento4 pagineEpidemiology of PTSD Version 3vemec31798Nessuna valutazione finora
- Association Between Specific Childhood Adversities and Symptom Dimensions in People With Psychosis - Systematic Review and Meta-AnalysisDocumento11 pagineAssociation Between Specific Childhood Adversities and Symptom Dimensions in People With Psychosis - Systematic Review and Meta-AnalysisSusana Pérez ReyesNessuna valutazione finora
- Kessler 2005Documento11 pagineKessler 2005mccg1478Nessuna valutazione finora
- Lehtinen 1994Documento4 pagineLehtinen 1994HARINI KNessuna valutazione finora
- Appi Ajp 2010 09050627Documento8 pagineAppi Ajp 2010 09050627FebniNessuna valutazione finora
- Kuehner 2016Documento13 pagineKuehner 2016Claudio AnguloNessuna valutazione finora
- Fonseca-Pedrero, Et Al., 2011Documento15 pagineFonseca-Pedrero, Et Al., 2011Diana StrambeiNessuna valutazione finora
- Assessment of Social Anxiety: A Controlled Comparison Among Social Phobics, Obsessive-Compulsives, Agoraphobics, Sexual Disorders and Simple Phobics"Documento3 pagineAssessment of Social Anxiety: A Controlled Comparison Among Social Phobics, Obsessive-Compulsives, Agoraphobics, Sexual Disorders and Simple Phobics"Aiman RashidNessuna valutazione finora
- Autistic Traits in The General Population: A Twin StudyDocumento7 pagineAutistic Traits in The General Population: A Twin StudyVi KekaNessuna valutazione finora
- Antisocial Personality Disorder: An Evolutionary Game Theory AnalysisDocumento12 pagineAntisocial Personality Disorder: An Evolutionary Game Theory AnalysisFernanda PastorínNessuna valutazione finora
- Cassidy Suicidality Schizophrenia 2018Documento11 pagineCassidy Suicidality Schizophrenia 2018Juan InsignaresNessuna valutazione finora
- Violence and Schizophrenia: Examining The Evidence: References ReprintsDocumento7 pagineViolence and Schizophrenia: Examining The Evidence: References ReprintsMarco AntonioNessuna valutazione finora
- Brohan 2010Documento8 pagineBrohan 2010RosarioBengocheaSecoNessuna valutazione finora
- ERQ PrevalenceDocumento2 pagineERQ PrevalencePhương Anh Cao HoàngNessuna valutazione finora
- MetaanalisisDocumento8 pagineMetaanalisisreant79Nessuna valutazione finora
- Life Events and PsychosisDocumento21 pagineLife Events and PsychosisSheyla Milagros Rivera CaveroNessuna valutazione finora
- Demencia en Gente Muy MayorDocumento6 pagineDemencia en Gente Muy MayorJimenaNessuna valutazione finora
- Comorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFDocumento24 pagineComorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreaming0% (1)
- Chang 2018Documento14 pagineChang 2018spaciugNessuna valutazione finora
- (2007) Adult Females (Females) (Males) : France PrevalenceDocumento25 pagine(2007) Adult Females (Females) (Males) : France PrevalenceADIL ALNUWISERNessuna valutazione finora
- Scales For ProdromeDocumento15 pagineScales For Prodromedrkadiyala2Nessuna valutazione finora
- Childhood Trauma Predicts Multiple High Lethality Suicide - 2019 - PsychiatryDocumento6 pagineChildhood Trauma Predicts Multiple High Lethality Suicide - 2019 - PsychiatryBelen MatteNessuna valutazione finora
- Alzheimer S Dementia - 2015 - Bubu - P1 257 Obstructive Sleep Apnea and Alzheimer S Disease A Systematic Review andDocumento1 paginaAlzheimer S Dementia - 2015 - Bubu - P1 257 Obstructive Sleep Apnea and Alzheimer S Disease A Systematic Review andDebbie CharlotteNessuna valutazione finora
- Unperceived Intimate Partner Violence and Women's HealthDocumento7 pagineUnperceived Intimate Partner Violence and Women's Healthjerdionmalaga1981Nessuna valutazione finora
- The EU-AIMS Longitudinal European Autism Project (LEAP) : Clinical CharacterisationDocumento21 pagineThe EU-AIMS Longitudinal European Autism Project (LEAP) : Clinical CharacterisationceliaNessuna valutazione finora
- Voice and Gender Incongruence, Relationship Between VocalDocumento6 pagineVoice and Gender Incongruence, Relationship Between VocalClaudia TorresNessuna valutazione finora
- Researching The Cultural Reaction On Mental Ill PatientsDocumento8 pagineResearching The Cultural Reaction On Mental Ill Patientsmail9967Nessuna valutazione finora
- Suicidal Behavior Among Adolescents: Correlates, Confounds, and (The Search For) Causal MechanismsDocumento3 pagineSuicidal Behavior Among Adolescents: Correlates, Confounds, and (The Search For) Causal MechanismsDrhouse001Nessuna valutazione finora
- Clinical Research: Epidemiology of Anxiety Disorders: From Surveys To Nosology and BackDocumento10 pagineClinical Research: Epidemiology of Anxiety Disorders: From Surveys To Nosology and BacksmacujaNessuna valutazione finora
- BJP 2001 Chong 29 35Documento8 pagineBJP 2001 Chong 29 35babon3Nessuna valutazione finora
- EpidemioDocumento6 pagineEpidemioFlavian Costin NacladNessuna valutazione finora
- Do Different Orthodontic Malocclusions Affect Patients' Self-Concept and Psychosocial Status?Documento4 pagineDo Different Orthodontic Malocclusions Affect Patients' Self-Concept and Psychosocial Status?Claypella MaskNessuna valutazione finora
- Journal of Affective DisordersDocumento6 pagineJournal of Affective DisordersKyze LQNessuna valutazione finora
- Angermeyer-The Stigma of Mental Illness-Patients' Anticipations and ExperiencesDocumento11 pagineAngermeyer-The Stigma of Mental Illness-Patients' Anticipations and Experiencesstraton_elena755Nessuna valutazione finora
- Schizophrenia and Violence PDFDocumento10 pagineSchizophrenia and Violence PDFTaylor AshermanNessuna valutazione finora
- The Phobia of the Modern World: Nomophobia: "Conceptualization of Nomophobia and Investigation of Associated Psychological Constructs"Da EverandThe Phobia of the Modern World: Nomophobia: "Conceptualization of Nomophobia and Investigation of Associated Psychological Constructs"Nessuna valutazione finora
- Psychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyDa EverandPsychopathology in Women: Incorporating Gender Perspective into Descriptive PsychopathologyMargarita Sáenz-HerreroNessuna valutazione finora
- PCB ConnectorsDocumento83 paginePCB ConnectorsMuhammad ZakaNessuna valutazione finora
- Pangkor Island MapDocumento1 paginaPangkor Island MapMuhammad ZakaNessuna valutazione finora
- OFDM Symbol Timing with PN SequenceDocumento4 pagineOFDM Symbol Timing with PN SequenceMuhammad ZakaNessuna valutazione finora
- MATLab 1Documento9 pagineMATLab 1Muhammad ZakaNessuna valutazione finora
- 2013 Annual Postgraduate Seminar ProgramDocumento1 pagina2013 Annual Postgraduate Seminar ProgramMuhammad ZakaNessuna valutazione finora
- Advanced Filter SynthesisDocumento20 pagineAdvanced Filter SynthesisTaiwo AyodejiNessuna valutazione finora
- Agorphobia, Simple Phobia, and Social Phobia in The National Comorbidity SurveyDocumento10 pagineAgorphobia, Simple Phobia, and Social Phobia in The National Comorbidity SurveyMuhammad ZakaNessuna valutazione finora
- Allen-Bradley PLC System DocumentationDocumento61 pagineAllen-Bradley PLC System DocumentationMuhammad Zaka100% (2)
- Mobile CommunicationDocumento19 pagineMobile CommunicationMuhammad Zaka0% (1)
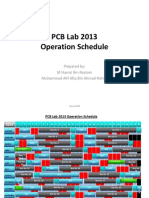
- PCB Lab 2013 - Schedule PDFDocumento2 paginePCB Lab 2013 - Schedule PDFMuhammad ZakaNessuna valutazione finora
- Essential Duas For MuslimsDocumento84 pagineEssential Duas For MuslimsMuhammad ZakaNessuna valutazione finora
- Design of BPF Using Sir With Floating ConductorsDocumento18 pagineDesign of BPF Using Sir With Floating ConductorsMuhammad ZakaNessuna valutazione finora
- Islam and Terrorism - English Book by DR Zakir NaikDocumento5 pagineIslam and Terrorism - English Book by DR Zakir NaikZakir NaikNessuna valutazione finora
- CST FilterDocumento28 pagineCST FilterMuhammad ZakaNessuna valutazione finora
- The Master Stroke To Victory! by Syed Zaid Hamid Shahzad Masood Roomi Madina-e-SaniDocumento16 pagineThe Master Stroke To Victory! by Syed Zaid Hamid Shahzad Masood Roomi Madina-e-SaniMuhammad ZakaNessuna valutazione finora
- 1.6.4 FFT AlgorithmDocumento19 pagine1.6.4 FFT AlgorithmMuhammad ZakaNessuna valutazione finora