Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Speech & Language Therapy in Practice, Autumn 1998
Caricato da
Speech & Language Therapy in PracticeCopyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Speech & Language Therapy in Practice, Autumn 1998
Caricato da
Speech & Language Therapy in PracticeCopyright:
Formati disponibili
Ice
A positive approach for C0111I11itted professionals
ISSN (online) 2045-6174 www.speechmag.com
quickly and easily
My favourite filin is on tv tonight.
Jma...I what ch I
I I I ......
. ....... door <IIot o:Mct
e r
t
y
d f
g
h
X c V
b
.,..,.
I ....
oa'"
-
cloda .1oiId
u
i
0
j
k I
n m
ox with exclus 'e e.
rough for fast, powerful augmentative communication .
.... i i - ~ .
..
The new DynaVox 3100 with DSS - DynaVox System Software - provides individuals with the speed
and power to communicat e more quickly and easily than ever before. With its large 30.5cm (12-inch)
diagonal display screen . augmentative communicators have the room to access more vocabulary.
And the DynaVox' s processing speed makes communication and page creation fast.
DSS can be found on all new DynaVox devices and software. Driven by DSS.
DynaVox provides hundreds of ready-to-use communication pages Driven
and vocabulary sets. so individuals can begin communi cating soon bll
after they turn on the device. DynaVox also features the fastest. most I I
comprehensi ve word prediction found anywhere. With a searchable. "concept-tagged" dictionary
of more than 128.000 word forms. DSS word prediction allows individuals to access vocabulary
DSS even comes with Song Manager. so users can create and sing songs by
placing notes on sheet music.
To find out more about the power and speed of the DynaVox 3100. and for a
demonstration contact
SUNRISE
Sunrise Medical Umited
Sunrise Business Park. High Street, Wollaston, West Midlands DY8 4PS England
Tel 01384 44 6789 Fax 01384 44 67 99
ISSN (online) 2045-6174 www.speechmag.com
I
www.soi.co.uk/s/speechmag
AUTUMN 1998
(publication date 3 I st August)
ISSN 1368-2105
Published by:
Avril Nicoll
Lynwood Cottage
High Street
Drumlithie
Stonehaven
AB393YZ
Tel/fax 01569 740348
e-mail:
avrilnicoll@sol.co.uk
Production:
Fiona Reid
Fiona Reid Design
Straitbraes Farm
St. Cyrus
Montrose
Printing:
Manor Group Ltd
Unit 7, Edison Road
Highfield Industrial Estate
Hampden Park
Eastbourne
East Sussex BN23 6PT.
Editor:
Avril Nicoll RegMRCSLT
Subscriptions and advertising:
Tel/fax 01569 740348
Avril Nicoll 1998
Contents of Speech & Language
Therapy in Practice reflect the views
of the individual authors and not
necessarily the views of the publish
er. Publication of advertisements is
not an endorsement of the adver
tiser or product or service offered.
Any contributions may also appear
on the magazine's Internet site.
Cover pictures:
Popular ch ildren's tv
Programmes .......
II
CONTENTS
.-::--
News/
Comment 2
Pushing for
more 4
Susan Gooding was recently
diagnosed with ReU' s Syndrome.
Speech and language therapist
Val Levens, Susan and her
mother Jennifer Gooding suggest
an open mind is needed.
www
speechmag 7
The new Speech 8- Language
Therapy in Practice Internet site
offers added value for subscribers.
Tracheotomy
and dysphagia 8
Stephanie Haynes and Judi
Hibberd explain a procedure
devised to inform assessment.
Low tech MC I I
Even experienced communica
tion aid users can struggle to
express complex views. Joan
Murphy describes the impact of
a low tech tool.
Reader Offer 15
Win RDLS III
Service
development 16
The success of Dr Deb Gibbard's
Parent-based Intervention
Programme, discussed in the
Summer 98 issue, has led to the
development of an evidence
based service.
Reviews 18
Learning difficulties, autism,
mathematics, child language,
education, aphasia.
Further Reading 20
Adolescents
Dysarthria 21
Speech and language therapist
Judi Hibberd and chartered
physiotherapist
Claire Jinks
argue
therapists can
maximise the
success of
tongue and lip
exercises by
adopting the
principle of
specificity.
.COVER STORY
How I view
children's
television 24
Four therapists discuss positive
aspects of television and video for
pre-school children and how the
subject of TV exposure might be
approached with parents.
MyTop
Resource 30
Julie Coley
describes how she
took an idea for a
piece of
equipment to
production.
WINTER '98 will be published on 30th November 1998
IN FUTURE ISSUES
drama articulation Right from the Star-t
progl'essive neurological disease dysphagia in ALD
SPEECH & LANGUAGE THERAPY IN PRACflCE AUTUMN 1998 1
ISSN (online) 2045-6174 www.speechmag.com
N EWS & COMMENT
Happy browsing
This issue marks a new venture for Speech & Language Therapy
in Practice with the launch of its Internet site. There are so
many ways the web could be exploited to enhance therapists'
practice, but that depends on readers contributing, I hope
students will make their pages a success and that all readers
will take this new opportunity to send in tips on a quarterly
theme. The first is ideas and resources jor Circle Time; you are
welcome to send as few or as many as you like and do not
have to have access to the Internet to participate as the end
result will be listed in a later issue of the magazine.
The Internet has had its fair share of critics but has
revolutionised society as television did before. Speech and
language therapists continue to have concerns about the
impact of television exposure on the development of
selective attention and speech and language. While it would
not be realistic to expect parents to ban television altogether,
we should perhaps have some knowledge of the programmes
available to the pre-school audience so we can guide viewing
selection. How I view children's television recommends
techniques for increasing parental understanding of the
positive and negative influences of TV exposure.
Improving child language is also the aim of Deb Gibbard's
development of evidence based practice across a service. Her
initial research was prompted by dissatisfaction with high
waiting lists and long waiting times. As has been demonstrated
before in this magazine, the only effective way of tackling
such problems is on a whole service level.
Val Levens has questions about the way her service delivery to
adults with a learning disability has changed. She believes the
discovery of Susan Gooding's abilities - and therefore
appropriate management - may have happened sooner had
the focus been different. Interestingly, the client herself is
more circumspect, accepting that time was as much a factor.
Another article demonstrating how our clients are truly our
best teachers comes from Joan Murphy. Her use of the humble
doormat has already improved the lives of many people; often
simple ideas are the most effective and flexible. Moving from
low tech to high tech, Stephanie Haynes and Judi Hibberd's article
may appear to be of interest only to those working in a very
specialised area. However, their systematic approach to decision
making, including the involvement of
other professionals, has wider applications.
Judi Hibberd again shows the benefits of
working with colleagues in other
disciplines in her article with chartered
physiotherapist Claire Jinks.
Whether on the pages of the magaZine
or those of the web, I wish you happy
browsing!
Avril Nicoll
Editor
Lynwood Cottage, High Street, Drumlithie
Stone haven AB39 3YZ
teilansaifax 01569 740348
e-mail avrilnicoll@sol.co.uk
or appointed by law
finn
An occupational therapist has been appointed
as client liaison manager in a law firm's
personal injury department.
I n what is believed to be the first such
appointment in the UK, Jayne Heslop will
liaise between lawyers and clients and represent
clients to other agencies such as employers,
schools and the Department of Social Security.
She believes the gap in services offered by the
NHS and the legal profession, particularly in
the field of catastrophic injuries, will be lessened
tlnough her work for Irwin Mitchell Solicitors.
Ready, steady, read
A scheme to provide schools with free reading
books has entered its second year.
The Ready Steady Read
l
catalogue comprises
over 200 books chosen with expert help from
the Department for Education and
Employment. Sponsors WH Smith are provid
ing a budget for more than 400 UK primary
schools to purchase books from the catalogue.
As the children move through the five year
scheme, the previous books are left for the next
year's intake.
For a copy of the catalogue tel. 0171 409 3222.
Technology aids
developing cOlmtries
The remote uniting of experts around the
world for an epilepsy symposlUm has given an
indication of how technology is advancing.
Group videoconferencing equipment brought
together a London, Warsaw and Senegal
audience to discuss the challenges for
epileptology in the 21st century in Europe,
Africa and developing countries. The conference
was organised by TEAM (Towards Education
for All with Multimedia), a non-profit
organisation recently established to enable the
exchange of global medical-education
opportunities using the latest technology, with
partlcular emphasis on developing countries.
Thi' videoconferencing facilities were provided
by PictureTel.
For further information on their products
see www.picturetel.com or tel. 01753
723701.
Reporting accidents and
ill health
New guidance gives healthcare workers specific
information on the reporting of work-related
accidents and occupational ill health in hospi
tals, nursing homes and general practice.
The Health & Safety Executive (HSE) believes
it only receives reports on 37 per cent of
accidents to employees in health and social
work. Its report answers basic questions about
what kind of events need to be reported and
whose responsibility it is to report them.
For information on The Reporting of
Injuries, Diseases and Dangerous
Occurrences Regulation 1995: Guidance for
employers in the healthcare sector tel. HSE
InfoLine 0541 545500.
SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUMN 1998 2
ISSN (online) 2045-6174 www.speechmag.com
Abuse advice
A national helpline
Three speech and language therapists have been
awarded scholarships by the HSA Charitable
Trust.
The awards help health care professionals pay
towards their fees
study for further
awards totalling f 160,000 were presented to 75
recipients by Tessa Sanderson.
Back L - R: Speech and langllage the rap)! award
winners Sasha Bemrose, Stella Kiszka and Valerie
Bmoks.
Front L - R: Ian
Sanderson and Philip
Trost Chairman.
Recognising eye problems
fessionals
people.
the Blind
lUords
ma,
sionals can obtain copies of the booklets Half
NEWS
~
and information
1 pack for profes
sionals working
with deaf children
The N.rionLll Deaf
who may be at risk
Childrefl'5
of abuse have been
Society
launched.
The NSPCC and The National
Deaf Children's Society
(NDCS) have collaborated to
produce the advice line A Voice
for Deaf Children and the pack
Safe in Your Hands. Deaf chil
dren can be more vulnerable
to neglect and abuse as they
may be less able to disclose
and come into contact with
more non-family members
than other children.
Advice line: tel . 0181 801 7211,
Tuesday and Thursday, 9am-5pm.
Safe in Your Hands from
Information Department,
NDCS, 15 Dufferin Street,
London EC1 Y 8PD, price 15.
NSP C
A ~ ~ ~ .
ps
and expenses when they
qualifications. This year
Adam, HSA Chaimllln, Tessa
Howard, HSA Charitable
A campaign to prevent avoidable
sight loss is targeting health pro
working with older
The Royal National Institute for
(RNIB) booklet Your
could save their sight
explains the effects of glauco
diabetic retinopathy,
cataracts and macular degener
ation and how health profes
sionals can help. The Eye
Health Campaign in general
aims to raise awareness of
the importance of regular
eye tests, especially among
higher risk groups.
Your words could save their
sight is free and health profes
an hOllr cOllld save YOllr sight and Open your eyes and get a good
eye test to distribute to the public. Tel. RNIB Helpline, 0345669999.
Signalong at work
Workplace notices to complement manual signs have been
unveiled by Signalong.
Pilot notices, consisting of written words combined with
Rebus-style symbols, have been developed as an extension of
the Signing the Way to Work Project. Signalong is a sign-sup
porting system based on British Sign Language (for the Deaf) .
The signs will be of use to anyone who is unable to read
English. Details: Signalong, tel. 01634 819915.
SIGNALONG Development Manager Gill Kennard (centre) with
her artist / researchers Kay Meinerrazhagen (right) and Linda
Hall (left) at the launch of the new workplace notices.
A2endafor
mange
Foll owing
qllalitative
research inw what
life is like for
people with a
commllnication
impairment, an
umbrella grallp
of commllnication
chariti es ha.s
produced an
agenda for change.
The research, commissioned from
City Uni versit), by the 42 member
Communications Forum, fOllnd
that, whatever the communication
disabilit), those interviewed all
faced the same barriers across
education, employment, financial
matters and everyday life. In addition
to continlling to publicise the needs
of people with communication
impairment, the agenda for change
means the forum will campaign for:
I better training for health,
education and social care
professionals and better partnership
between professionals, clients and
families
2. the right w accessible information
and support, including interpreters,
a.ssistants and technical aids
3. changes in disability educaLion
and legislation to take more account
of commul1ication impairment.
Communications Forum, PO Box
854, 3 Dufferin Street, London
EelY 8NB.
AFASIC
30th
birthdaycal
The national volllntary
organisation representing
children and YOllng people with
speech and language
impairments and their families is
demanding better services.
To mark the occasion of its 30th
birthday, AFASIC, fOllnded by
speech and language therapist
Margaret Greene, is holding an
Awareness Week beginning on
20th September. Six key issues
have been identified:
1. the need for early intervention
2. the shortage of specialist
educational provision
(partiCl/lar/y for 11 years +)
3. how to ensllre a smooth
transition into adllithood
4. the lack of clarity in law over
who is responsible for providing
help
5. the need for better initial and
continuing edllcation of
professionals
6. the shortage of speech and
language therapy in most areas of
the UK.
AFASIC, tel. 0171 236 6487.
SPEECH & lANGUAGE THERAPY IN PRACTICE AlffiJMN 1998 3
ISSN (online) 2045-6174 www.speechmag.com
ALD
adutt
For- year-s ft
was assumed
that Susan
Retfs
Gooding had
a pr-ofound
leaming
S drome:
disabilfty Her
speech and
language
tne feelings
therapist,
Val Levens,
Susan her-self and
and her
mother- Jenny
outcomes
share the
expenence
of revealing
the realfty
Open to Leaming
Val Levens wants to prevent other clients like Susan having to wait for a successful
outcome of therapy. In a highly personal account of her Invo7vement With thiS case, she
examines the wider implications for the professIOn.
R
eviewing the events of the ten years I have known
Grappling with the system
Susan, it is the feelings that leap out at me. Fear, frus
The special care unit used by Susan had a custodial philosophy
tration, humility, hope, anxiety and inadequacy - that
rather than a developmental one. I went through the - almost tra
is enough to be going on with, isn't it? Too touch
ditional - grappling with a system I was not truly part of and had
feeling for an article, perhaps.
no power in. I attempted staff training, I built good relationships
Outcomes - now that strikes a better note. What is the outcome?
with the staff team and we achieved some success together before I
Ten years ago Susan was confidently labelled by all except her
changed my post from a site based to a referral based one and so
mother as having a profound learning disability. She used the spe
spent less time in the day centre.
cial care unit of her local learning disability day centre and Social
Eight years ago, one of the day centre officers heard about Rett's
Services respite services. She could move her clasped hands to tap
syndrome and mentioned it to the parents of two women using the
acup signalling "Give me more to drink" and sometimes used
centre. Susan and the other lady were both formally diagnosed and
facial expression to indicate emotional states. Most frequently
we began to look in the literature. The Rett's Society (Resource 2)
Susan smiled when helped to walk around the centre. She could
was very helpful in giving us a framework to work within, but the
also frown, turn her head away and draw her knees up to signal a
literature was depressing reading. Skills are lost from around a year
negative state.
of age and although there was some information about women
Now, she independently uses a Toby Churchill Octet (Resource 1)
with Rett's, I found nothing positive except that eye contact
for basic care messages. More complex communications are sig
appeared especially good in the 15-30 year olds (Resource 3).
nalled by hand pointing to cards with words on them, arranged in
topics, or by pointing to letters on an alphabet board. Commrtrnent surprise and g u i ~
Susan chooses her clothes, presents for others, meals from a recipe What we had was a mass of literature, high commitment from
book, and is able to provide feedback to carers, family and friends Susan's mother and a collection of our observations of Susan her
on her perception of interactions with them. self. The family bought an lntrowlker aid (Resource 4) and, by the
SPEECH & LANGUAGE THERAPY LN PRACTICE AUTUMN 1998 4
ISSN (online) 2045-6174 www.speechmag.com
ALD
time I met them, had worked out that touching with
finger tips was difficult, while a side to side fist
movement, using an adapted switch, was good for
Susan. Seeing she could sometimes use her hand
meaningfully was a surprise to me. We used sym
bols with words at first, and it was - the pattern
being very clear now? - Jenny, Susan's mother, who
real.ised that her daughter could use the words alone.
I think I left guilt out of the list of feelings above, but
it was at this point family, friends and I experienced
a deal of it. Why had we not seen sooner what she
might be capable of? Why hadn't we done something?
This happened against a background of considerable
cynicism from some of the workers involved with
Susan and her care. I recall her word board being
handed to me with the phrase, "Here's her bleeding
ouija board".
'ng ln.c.oV'YY"lailon
Collectl II I I I I
Val Levens is Speech &
Language Therapy CO-Manager
for Thames Gateway NHS Trust
at the Speech & Language
Therap1' Department, Medway
Hospital, Windlllill Road,
Gillingha m, Kent ME7 5 N l ~
wi. 01634833711.
was needed was a positive movement to ' remind' her
arm how to work
Open to learning
In acknowledging the range of feelings those
involved with Susan have gone through, I see that
sometimes they have got in the way, but on other
occasions they have been a spur. In either case,
ignoring them did not help much. I was part of a
team where the key players were Susan, her mother
and CheryL the visiting support worker. The ideas,
the vision, and the drive came from Jenny, Susan's
mother, and I learnt much from her, not least that
many of us do not listen to families as much as we
think we do. We need to be open to learning as well
as being keen to teach.
[t is, to misquote Jane Austen, a truth universally
acknowledged that a person in need of a communi
c c
cation system is in lor a long wait belore we get it
With the benefit of hindsight, I see now that my role was to collect
and arrange the info rmati o n and ideas given me along the way. 0
one had the whole answer packaged for us - and sometimes we did
not recognise at once the value of what had been given. The posi
tive relationship built with a worker who visits Susan at home has
been hugely significant and the first forum for communicative suc
cess. Along the way we learnt from a visit to a multidisciplinary
Rett's team at Radlett (Resource 5), and from an appoimmenl at the
Charing Cross Hospital Augmentative Communication Centre
(Resource 6). It seems important that Susan has relatively good
mobility and has never had fits. These facts may be linked to her
current level of functioning.
For a long time, Susan was able to spell out letters or choose words/
phrases more easily if her hand was supported by someone else.
This made very l.ive to me the debate about functional communi
cation and its validity. For that, as well as other reasons, it is pleas
ing to see she now requires that support less often, and not at all
with the Octet. I wonder now if, instead of the support of a hand, what
right. As Susan describes herself, a number of factors need to come
together for things to work. There are physical issues - where to
place it, how best to touch it; intellectual ones - what to put into it;
and oceans of people factors, including getting a circle of people
really list ening and willing to be directed by the communicator.
Preventing the wart
A more systematic approach, early on, could have saved Susan
time. If I had managed to get signs and symbols used in the day
centre, this might have given us a due to follow sooner. Making
contact with families earlier, rather than seeing liaison with the
centre as my focus might also have been more productive.
I would like to see this article as part of preventing the wait for oth
ers who have Rett's. There is the central issue about the possible
spin-offs of good communication practice in day centres and how
that is best achieved.
I am very grateful for what I have learned from Susan and Jenny.
... ........... ... ... .. ... ................................................ continued over/ea(
ESOURCE UPDATE. ..RESOURCE UPDATE. ..RESOURCE UPDATE..
New communication aid
A new low-cost communication aid storing up to eleven user Uvin with
defined messages has been developed,
The Tana Talker is a lightweight hand-held device which also Par.l.son'S
A new booklet is aimed
has a dedicated alarm button. Recordings of up tofive seconds
at people who have each are stored on a microchip rather than a tapefor high
been associated with quality sound reproduction. They can be made by a person of
Parkinson's disease for
Cost: 175 (+ VAT if applicable)
the users choice.
some years.
Details: Masterswitch (UK) Ltd, 8 Dorset Road, London N15 5Al Moving On is an A-Z of
- -------------------1 practical advice about
Learning disability resources
A new book alms to help staff decide whether the sexual
behaviour of male clients with learning disabilities is abusive
or unacceptable,
Response-ability Is a practical guide for staff to work through
in groups and consider how serious the situation is and how
best to manage it while co-ordinating services and profes
sional input to support and contain the man in the least
restrictive setting.
Its publisher, Pavilion, has also revised two other resources,
one a training paCkagefor staff working with people in Joss
and grief situations, the other a sex education paCkagefor
working with people with learning disabilities. A newassess
ment, teaching and evaluation package to help care workers
discuss issues Of 1/1 health with groups of people with learning
disabilities is also available.
Response-ability costs 35.95, Looking at LOss 59.95,
Sex and the 3 Rs 85 and Feeling Poorly 145, all plus 10
per cent pap from Pavilion Publishing tel. 01273 623222.
day to day living and
the ever changing
nature of Parkinson's.
Researched by health
and welfare profession
als and members and
staff of the Parkinson's
Disease Society (PDS),
the guide covers issues
including medical treat
ments, finance and
employment. The
Society intends it to be
a definitive reference
guide for all involved
with Parkinson' s.
Moving On is free from
the PDS, tel. 0171 931
8080.
Cog neuro workbooks
Photocopiable workbooksfor use with adults with
acquired neurological disorders have been produced
by a speech and language therapy department.
Based on the cognitive neuropsychological model
of language processing, the seven workbooks were
developed over two and a half years by the thera
piSts and their assistant. They cover odd one out,
semantic circles, verbs, object selection and word
association and range in price from 76 to 26
with a full set costing 84 including pap.
Order fonn from Speech 8- language Therapy Dept,
Stobhill NHS Trust, Balomock Road, Glasgow G21 3UW.
Insurance for self-emploved
A guide to insurancefor people who are seU
employed or partners in a business has been
recognised by the Plain English Campaign. Issues
and choices are explained through case studies.
For a free copy of 'Zurich's Guide to Self Employed
and Partnership Rnancial Security, tel. 0345 626624.
Advice in Punjabi
The British Stammering Association's leaflet "Does
your young child stammer?"for parents Of chil
dren under 5, is available on audiotape translated
into Punjabi. Urdu, Gujarati, Bengali and Somali
translations will be available in due course.
150 eaCh, 5 for 4 from BSA, 15 Old Ford
Road, London E2 gPJ.
SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUM 1998 5
ISSN (online) 2045-6174 www.speechmag.com
I
Never give up
Sue Gooding describes her path to independent communication and says she still
has much she wonts to achieve.
Recently I have obtained a computer which
last five years my life has had a dramatic
am a young lady in my thinies. Within the
allows me to have a voice. This was a goal I
change for the better. [have been lucky. had in my mind for many years. My Mum
My family and friends have been very sup asked if I would have been able to communi
portive to try and give me a better life. cate sooner if the right people had come
When I was young Mum knew [ could under together earlier and I do not think so. I came
stand cenain things. I felt I was trapped. My to the point when I knew I could do it but
mind knew but my body and condition needed a way. It was about a year before
stopped me from leading an independent Cheryl, my best friend, staned to work with
life. I am not angry or bitter, just relieved I me. With Mum's pushing and ideas and
can now be understood. Cheryl's understanding and patience we got
It has taken my determination and my there.
Mum's and friends' patience for me to get to There are still goals I have and I am working
where I am now. [ have had to work hard try towards them, like holidays, life experiences
ing to get my hand to do what my mind and independence. It is made easier now
wants it to. It is very frustrating. I have to because I have a voice. If you know someone
concentrate everything down through my arm to make my hand who might be trapped never give up on them. They have a per
work while still thinking about what I am going to say. sonality inside.
Pushing for more
Jennifer Gooding explains what she has learnt over the years from working with
her daughter.
A
s I did not know Sue had Rett
Syndrome until she was 30
years old, I concentrated
mainly on her physical dis
abilities because I perceived
she was always happier if she was on the
move. It was only later in her life that I had
ideas about her intelligence and then was pre
vented from helping by the fact that, in addi
tion to no voice, Sue could not move her
hands normally but kept them clasped
together. Her eyes were always very expressive
and I used them to help tell me what to do.
However, Sue has taught me never to presume
there is no intelligence and always to push to
achi eve more.
Sue, we discovered when she was 30, could
already read, tell the time, knew her colours
and had a knowledge that most of us are
taught through our school days and life. She
had used her intelligence while trapped in her
body and had catalogued all sons of informa
tion gleaned from conversations overheard,
television, music and books.
My main thought is to always have an open
mind and be prepared to learn or even tum
everything on its head and stan again. J feel
very humble and very gratefu I for Sue's miracle.
Resources
1. Toby Churchill Ltd, 20 Panton Street, Cambridge CB2 I HP, tel. 01223 567117. The Octet is priced at 380 (plus VAT if applicable).
2. The Rett's Society can be contacted at tel. 01487 843110.
3. This anicle has deliberately focused on an individual rather than the syndrome she happens to have. For funher information on up-to
date understanding of the condition, readers are referred to:
Reilly, S. (Feb. 1998) Rett Syndrome. Bulletin. Royal College of Speech & Language Therapists.
4. lntrotalker is available from Liberator Ltd, Whitegates, Swinstead, NG33 4PA, price 1100.
5. The Rett Therapy Clinic at Harper House Children's Service in Radlett, Herts is run by Horizon NHS Trust. For information, tel. 01487 843110.
6. Charing Cross Hospital Communication Aid Centre, tel. 01818461057. 0
Questions
What is required for a successful For AAC therap>, to work, physical,
outcome using alternative and
.1I11MWII intellectual antf people factors all have to
augmentative communication (AAC)'? come together at tPJe right time.
What role can a therapist play in a A therapist can collect and arrange
complex case? information and ideas, including what may
not immediately appear useful.
Where should a therapist start Therapists may find it most productive to
'fjI1iM1 work with and listen to families from an early
when planning how to improve
communication practice in day
stage.
centres?
SPEECH & LANGUACE THERAPY IN PRAcnCE AUTUMN 1998 6
ISSN (online) 2045-6174 www.speechmag.com
WEB SITE
www.sol.co.uk/s/speechmag
e-mail avrilnicoll@sol.co.uk
Speech & Language Therapy in Practice now has a
complementary 7nternet site. The site provides regularly
updated general information on the magazine and offers new
opportunities for readers to share ideas.
top tips on a theme*
Featuring in the Autumn 98 speechmag:
student section*
Top Tips for Circle Time
reprinted articles*
an edited open forum As the new term starts, therapists working in education
subscribing
would appreciate ideas and useful resources for Circle
Time. Even if you have just one suggestIon, please send
contributing / what
it If everyone contributes, everyone benefits.These will
readers want
be added as they come in to the \Neb site, then listed in
books for review I
the Spring 99 issue ofthe magaline
SPEECH & LANGUAGE THERAPY TN PRACTICE ALITUM 199 7
ISSN (online) 2045-6174 www.speechmag.com
DYSPHAGIA
Ing
and la
With the aid of case examples, Stephanie
Haynes and Judi Hibberd explain a
standardised proced re devised to
infonn dysphagia assessment in patients
with a tracheotomy.
A
t Walsgrave, a busy hospital with three intensive
treatment units (rrus), the speech and language
therapy department is regularly asked for swallow
ing assessments of patients with a tracheotomy.
The first decision we have to make is whether a
patient's respiratory status is such that they can
cope with a dysphagia assessment. Then, in addition to the normal
symptoms of dysphagia associated with neurological problems, the
following points should be considered when a patient has a tra
cheotomy:
1. Tethering of the larynx due to the tracheotomy tube causing
reduced laryngeal elevation and risk of aspiration.
2. Poor subglottic pressure because of the open stoma, leading to
problems with building up enough pressure in the chest cavity to
achieve adequate tongue base retraction and initiate a swallow
sequence safely.
3. Poor oxygen saturation levels can result in difficulty with the sus
pension of respiration for long enough to swallow safely.
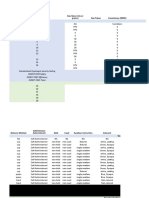
We have therefore been using a tracheotomy checklist (figure 1)
developed in conjunction with physiotherapists to improve dys
phagia management. This provides a formal, standardised proce
dure, based on clinical evidence.
Part 1 of the form is used to gather information which can then be
discussed with a physiotherapist and a decision made as to whether
the patient's respiratory status allows a swallowing assessment to
be carried out safely. All the information required can be obtained
from nursing staff, medical notes and the patient's marquette mon
itor. Each hospital has its own monitors and nursing staff should
be consulted regarding the set up of monitors in each area as Lraces
can be adjusted and colour changed to suit individual units. Each
monitor will have its screen divided into two. The left section is a
trace from a lead attached to the patient; the right is a numerical
read-out of that trace. Figure 2 explains the terms used in Part 1 and
their significance for the assessment.
Once the Part 1 information has been gathered, a physiotherapist
should be consulted on the level of the patient's respiratory status.
If it is felt that it is unsafe to carry out a swallowing assessment, the
reasons should be documented in the patient's medical notes.
If a swallowing assessment is to be carried out, the speech and lan
guage therapist records the information in Part 2 of the checkJisl:
The type of tracheotomy tube.
The frequency of suction. This information may need to be gath
ered from nursing staff, physiotherapists and medical sources.
For a cuffed tube, whether the cuff is deflated; if not, if it is med
ically safe to deflate it, whether this is tolerated and, if so, for how
long. (It is preferable to assess with the cuff down, as this generally
causes the patient less trauma. However, the assessment can pro
ceed with the cuff inflated or partially deflated - see Logemann,
1996).
After completing this, the speech and language therapist may
decide not to proceed with the assessment if (a) there are excessive
secretions or (b) it is unsafe to deflate the cuff.
Part 3 of the checklist concerns the use of the 'blue dye' test
(Gi,Jardeau et aL 1995). The results of this test should be interpret
ed conservatively and monitored carefully, as experience indicates it
is not wholly reliable. The blue dye test should be carried out in
conjunction with a standard bedside evaluation of swallowing.
The two case examples (see page 10) illustrate how the checklist
works in pradice. In case A it was decided not to proceed with a dys
phagia assessment after Part 1 of the checkJist was completed on the
grounds the risk of aspiration was too high. In case B, the swallow
ing assessment was judged safe after Part 1 was completed and the
remainder of the checklist aided assessment and review until the
swallow was found to be safe.
The checklist has improved the management of tracheotomy
patients in Walsgrave Hospital, Coventry. It helps ensure a stan
dardised approach to tracheotomised patients with dysphagia,
based on objective medical evidence.
SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUMN 1998 8
ISSN (online) 2045-6174 www.speechmag.com
DYSPHAGIA
Figure I . Tracheotomy checklist
Coventry Healthcare NHS Trust
TRACHEOTOMY CHECKLIST
NAME: DATE:
Part 1:
RESPIRATORY STATUS:
VENTILATED BY: SELF-VENTILATED
CMV
SIMV
SPONT
PCV
FRACTION OF INSPIRED 0 2 (Fla. ):
a. SATS: with mask:
Haemoglobin level:
(Note: Normal 0, Sats = 90+, FlO, 20%)
MONITOR:
ASSISTED
BY CPAP
SUPPLY: mask I cannulae
normal air:
ECG trace I
Blood pressure trace
----- --,
Central venous pressure
O. sats
I- - - -- - - -
I
I
,
I
Pulmonary artery capillary pressure
Respiratory rate
!
PHYSIO'S OPINION RE-RESPIRATORY STATUS:
Part 2:
TYPE OF TRACHEOTOMY:
Name: Size:
Mini I Cuff I Fenestrated I Speaking Tube
FREQUENCY OF SUCTION:
CUFF DEFLATED? yes I no Is it medically safe to deflate? yes I no
Tolerated? yes I no How long?
Part 3:
Note: Suction before deflating cuff via tracheotomy and oropharynx
Cuff deflation - amount of air
Reaction to cuff deflation
Ability to breathe by occlusion of tube (Note: only do with cuff down)
Voice quality
Swallow: Dye in water
Suction %
Dye in semi-solid
Suction %
Not e: Remember to re-inflate cuff.
Figure 2 - Explanation of Part I of
checklist (terms corresponding with
those on the checklist are in bold)
Respiratory status:
Ventilated either by Continuous
Mandatory Ventilation (CMV),
Synchronised Intermittent
Mandatory Ventilation (SIMV),
Spontaneous ventilation (Spont) or
Pressure Controlled Ventilation
(pcV) . (See Dikeman & Kazandjian,
1995.)
or
Self-ventilated
or
Assisted by Continuous Positive
Airway Pressure (CPAP)
These various methods all keep the
alveoli open and therefore affect
the oxygen saturation and fraction
of inspired oxygen.
FlO. is fraction of inspired oxygen.
The higher the percentage of oxy
gen being given, the more depen
dent the patient is on respiratory
assistance and the less likely they
are to have a safe swallow (Eibling
& Gross, 1996).
The oxygen saturation (0. sats)
number is only useful in conjunc
tion with haemoglobin (Hb) level
( normal level - female: 12-14, male:
14-16). The saturation level needs
to be 90 per cent or above. Below
this level, respiration cannot be
safely suspended.
Monitor:
The lCG trace is the heart activity
shown as a trace and the rate
shown as a numerical value. Any
change and the return to the nor
mal pattern should be observed.
Arterial PressuJ'CZ I blood pressure
trace. The lead enters the patient's
arm and will be mar1<ed ' arterial line' .
It is advisable not to bend the
patient's arm during assessment, as
this may adversely alter the trace.
Low blood pressure would signify
poor respiratory volume and so
coughing would be difficult.
The central venous pressure
(CVP) level is set by the doctor
responsible for the patient's care. It
will not affect the assessment.
Oxygen saturation (0. salS) levels
are measured by a device clipped
onto the patient's finger. The read
ing should be 90 per cent or
above.
Pulmonary artery capillary pres
sure ( PACP) tests the internal pres
sure of the left ventricle and will
not affect the swallow.
The normal respiratory rate is
approximately 12 - 16 breaths per
minute.
Stephanie Haynes and fudi Hibberd are speech and language therapists Swallowing Management o f Tracheotomised and Ventilator
with Coventry Healthcare NHS Trust. Dependent Adults, Singular.
Eibling, D,E, and Gross, R, D, (1 996 ) Subglotti c Air Pressure: A Key
Acknowl edgement
Component of SwaJlowing Eft1ciency, An nals of Otology, Rhinology
We wou,ld like to thank all those who responded to our request in
and Laryngology 105 (4) ,
the September 1997 Bulletin of the Royal Col lege o f Speech &
Gil ardeau, c., Kazandjian, M,S" Bach, l.R" Dikeman, K,)" WilJ ig.
Language Therapists for information about tracheoto my protocols
T. N" Tucker, LM, (1 995 ) The Evaluati on and Management of
and guidelines, We felt this anicle would be a good way of passi ng
Dys phagia, Seminars in Neurology 15 ( 1),
on the format we have devel oped,
Loge mann, l ,A, ( 1996) Evaluati on and. Treat ment of Swalim',;ng
References Disorders, Advanced Sessio n and Interpreting Videofluoroscopic
Di keman, K. l , and Kazandji an, M,S, (1995 ) Communica tio n and Swall ow Studies, "see over (or case ~ - ...
SPEECH & LANGUAGE THERAPY IN PRACfICE AUTUM 1998 9
ISSN (online) 2045-6174 www.speechmag.com
- -
- ----
--
DYSPHAGIA
Case A
IS, aged 72 years, was admitted with sudden onset of chest pain
and a history of angina. He required a uiple coronary anery bypass
graft which was performed within three days of admission. Post
operatively, he was admitted into ITU but there was some difficul
ty in weaning him off the ventilator. The doctors wished to start
oral feeding as soon as possible. However, it was discovered that IS
was not responding well and he was subsequently referred to
speech and language therapy for a swallowing assessment. This
occurred at four days post operatively, after he had been uansferred
to the high dependency unit.
Using Part 1 of the form, infonna tion was gathered from the med
ical notes, nursing kardex, nursing staff and physiotherapists.
Coventry Healthcare NHS Trust
TRACHEOTOMY CHECKLIST
NAME: DATE:
Part 1 :
RESPIRATORY STATUS:
VENTILATED BY:
ASSISTED
CMV BY CPAP
SIMV
SPONT
PCV
FRACTION OF INSPIRED 0, (FlO.): 40% SUPPLY: mask / cannulae
0 , SATS: with mask: BB% normal air:
Haemoglobin level: 9
(Note: Normal 0, Sots = 90+, FlO, 20%)
MONITOR:
ECG trace 120
Blood pressure trace
Central venous pressure
0 , sats 88%
Pulmonary artery capillary pressure
-
Respiratory rate
25
PHYSIO' S OPINION RE-RESPIRATORY STATUS:
Not safe to carry out aS6essment
... " .......... .. .. ", .......... .. . . . . . . . , . . . . . . . . . . . . . . .. ..... ........ .. ................
" .
IS was self-ventilated, the oxygen saturation levels were 88 per cent,
the fraction of inspired oxygen was 40 per cent and the haemoglo
bin level was 9, showing that respiration was compromised and IS
would be unlikely to be able to suspend respiration for long
enough to swallow safely.
IS was also unable to tolerate the cuff being deflated for more than
a few minutes at a time, and required half-hourly suction. The
monitor read ings showed an erratic heart rate and an increased res
piratory rate. In discussion with the physiotherapists it was decid
ed that IS's condition made a swallowing assessment unsuitable at
this time.
The information recorded on the form thus enabled a judgement
to be made against carrying out a swallowing assessment, on the
grounds that ri sk of aspiration was too high.
CaseB
GB, aged 59 years, was admitted to lTU with multiple fractures after
a road uaffic accident. A cr sca n showed a large subdural
haematoma in the right parietal region. This was evacuated and
post operatively GB was tracheotomised because of a compromised
respiratory sta
Coventry Healthcare NHS Trust
rRACHEOTOMY CHECKLIST
tus. He was
NAME: DATE:
then referred to
speech and
Part 1:
RESPIRATORY srATUS:
language thera
vtNTlLATED BY: GVENTlLArV
ASSISTED
CMV BY CPAP
py for a swal
SIMV
lowing assess
SPONT
PCV
ment. GB was
not on a moni
FRACTION OF INSPIRED 0, (FlO,): 24% SUPPLY: mask / cannula.
tor but the rest
O. SATS: with mask: normal air: 92'7.
Haemoglobin level : 11
of the form
(Nore: Normal 0, SalS =90+, FlO, 20",{,)
was used to
MONITOR: gather the nec
ECG trace
essary informa
Blood pressure trace
I
Central pressure t ion.
0. salS
The oxygen sat
Pulmon;'ry-artery copillOl'Y pressure
Respiretory rate uration levels
were 92 per
PHYSIO'S OPINION RERESPlRATORY STATUS,
.. QKt.Q.. p.ro.cccd. ............. cen t, the frac
Part 2:
tion of
TYPE OF TRACHEOTOMY:
Nam@rtex
Size, 9 inspired oxy
Mini Cuff Fenestrated I Speaking Tube
gen was 24 per
FREQUENCY OF SUCTION: three - four times daily cent and the
haemoglobin
CUFF DEFlATED@no Is rt medically sate to denate? yes I no
Tolerated@no How long? all the time level 11; suc
tion was used
Part 3:
NOlO: 5uaion befOre deflarjng 0Jff "" lIOcheDuxrrt , r;! OO1>jJharynx infrequently at
this stage of
Cuff deflation - amount of air
cuff already deflated
Reaction to cuff deflation GB's recovery.
Ability to bredthe by occiusioo of tube (Noa::odt Co .... 0Jff dawn) 0 K
The tracheoto
Voice quality weak and hoarse
Swallow: Dye in water my cuff was
Suction 12% from oropharyn< & tracheotomy
deflated and
Dye in semi-solid
Suction % Not done GB tolerated
Note: Remember [0 cuff. N / a this well. It was
therefore
decided, in discussion with the physiotherapists, that it would be
safe to conduct a swallowing assessment.
Oral movements were observed to be mildly reduced in speed,
strength and accuracy. With a liquid swallow, using the 'Blue Dye'
test, GB showed good antidpation and good lip closure. The oral
phase was slightly slow and initiation of swallowing was mildly
delayed. Laryngeal elevation was incomplete. GB attempted to ini
tiate a further swallow to clear the pharynx. On suctioning, small
amounts of the blue dye were suctioned from the oropharynx and
the tracheotomy, indicating an unsafe swallow.
It was felt that the laryngeal elevation was incomplete due to teth
ering of the larynx by the tracheotomy tube and reduced tongue
base retraction. GB was reviewed regularly. Shortly after the initial
assessment, the uacheotomy tube was removed. Reassessment of
his swallowing indicated it was now safe. 0
Questions
What particular aspects of a
Problems with laryngeal elevation, initiation of the
tracheotomy influence swallowinGJ :.; swallow and suspension of respiration
ability'? can occur in patients with a tracheotomy.
Why is a tracheotomy checklist A formal checklist based on clinical evidence
. useful? improves patient management through offering
a standardised approach.
Who should be involved in decision Speech and language therapists must take
11111111111 account of medical, nursing and physiotherapy
making about swallowing
assessment in patients with a assessment and opinion.
tracheotomy?
10 SPEECH & lJ\NGUAGE THERAPY IN PRACflCE AUTUM N 1998
ISSN (online) 2045-6174 www.speechmag.com
AAC
Even
experienced
communication
aid users can
struggle to
express
complex views.
Joan Murphy
describes the
impact a low
tech tool
developed to
address this has
had on the
lives of people
with severe
communication
difficulties.
Tall<ing
Mats :
Speech and
angua e
researc
in practice
I
n 1996 the Alternative and Augmentative
Communication (MC) research team at
the University of Stir"ling received a grant
from the Gannochy Trust to examine peer
interaction of adult MC users in a resi
dential setting. Following the first part of the
research, involvi ng detailed observations of the
ni ne users who volunteered to participate, we
wished t o obtai n the clients' views and percep
tions about our findings. Although many were
experienced communication aid users, we
were aware they might still have difficulty
expressing their views about some of the com
plex issues we wished to ask them about,
either because they did not have the explicit
vocabulary in their devices or penhaps because
they had not had to think about these matters
previously.
The 22 iss ues we wished to discuss (Resource
I) included
residents ignoring each other
communication at mealtimes
reluctance to use communication aids
talking to staff rather than other residents
the use of pre-stored phrases in MC
pnvacy.
Having just acquired Boardmaker"HA software
(Resource 2), we decided to try to produce a
range of picture symbols representing these
issues. It was important they could be present
ed in a clear. interactive and accessible way as
we wanted the MC users to be able to con
sider the points in question and express their
views in their own time in an unambiguous way.
The framework we came up with proved so
successful that many people have encouraged
me to develop it for a range or clients. This has
resulted in the production of a booklet and
video package, Tolking Mots (Resource 3).
True representation
The basIC jus consists of three sets of picture
symbols pres _ ed to the person with the
communication drfficulty by attachrng the pic
tures to textured mats. The client can then
select them, move them around and change
them until s/he is happy the picture
on the final mat truly represents mat meant.
The three picture sets are
I. Issues
2. Emotions
3. Inruences
The issue/s to be discussed can be anything
from a simple choice about daily living to a
complex matter relating to li fe e e ts. The
range of emotions allows the client to describe
his / her feel ings about each issue; the number
and subtlety wi ll depend on ability and age. The
Inruences include a range of factors which
might have either a positive or negative effect
on the issue being discussed.
Flexible framework
The framework is very flexible as it is up to
the people using the Talking Mots to decide
which issue/s, emotions and influences to
include. Once identified, they can be created
using whichever pictorial representation is
most suitable. Boardmaker picture commu
nication symbols are attractive, flexible and eas
ily modified but any picture symbols familiar to
the cl ient could be used provided they are
clear and illustrate the issues being discussed.
The mats I used are textured doormats which
can be bought in any hardware shop. They
were chosen because pictures with Velcro
TU
tabs on the back can be attached to them and
moved around. This means people can I era.
build up a picture of their views which t G
SPEECH & lANGUAGE THERAPY IN PRACTICE 199 11
ISSN (online) 2045-6174 www.speechmag.com
AAe
Case - Frances
Frances has cerebral palsy and uses a whole range of communication methods, including her communication aid, voice, eyes
and facial expression. As her speech and language therapist I wanted to know what she felt about using the telephone
and how best I could help her. Because I knew her residential situat ion I was able to make up a range of pictures which
might be relevant t o her .The Tolking Mots helped her explain what she thinks about using the telephone - what she
finds helpful and what difficulties she has. A lthough Frances is an experienced AAC user. it takes her a lot of time and
effort to express complex thoughts.
The first mat allowed Frances to
indicate broadly what she felt about
using the issue being d iscussed - the
telephone - by eye pointing to the most
appropnate emotion picture. Frances
indicated that she was fairly content
using the telephone but that she still had
a few problems.
.IV ai, - f!J I
These are the range of influences which
were presented on the second mat.
_ 'gj" [I, [ij]
ilEa II II
This IS the final mat which Frances
gradually bui lt up by eye pointing to the
influences she considered important
and whether they were positive or
negative. The things which Frances
found positive and helpful when using
the telephone were
having enough time
having privacy
using pre-stored phrases
havi ng altered the voice to achieve
maximum clarity on the phone
using the answering machine.
The difficulties for her were
how to end the conversation
problems when her communication
aid breaks down.
She also added it is difficult when the
person she is calling does not realise
she is using a communication aid and
does not give her enough ti me t o
explain thi s. She felt great satisfaction in seeing her views gradually taking shape and being clearly ill ustrated on the final
mat.
These views were used to plan further work with Frances. She is now a member of a small group of Lightwnter users
who are working on communication strategies including telephone use. She also attends College where one of her
courses looks at telephone skills
12 SPEECH & LANGUAGE THERAPY IN PRACTI CE AUTUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
AAC
then consider; change and confirm in their own
time. For people with a physical disability this
design removes the effort needed to finger
point, operate a switch or access a keyboard
the participant can simply eye point and the
communication partner can do the selecting
and moving of the picture sym bols.
Talking Mats do not replace someone's com
munication aid / MC device. Al l the people
who have used the mats have done so in con
Junction wrth both their existing MC devices
(where they have them) and non verbal meth
ods of communi cation such as facial expression
and gesture.
Wide use
Onginal ly for adults With cerebral palsy using
high tech communicat ion aids, the mats have
since been employed by a variety of people,
both children and adults with a wide range of
communicat ion difficulties, in one to one situa
tions and in groups. The case examples (I - 3)
illustrate how they have been used with t hree
different people who are shown in the video
accompanying the booklet.
Talking Mats have also been used with a num
ber of other people in slight ly different ways,
for example wrth people with learning difficul
ties by presenting fewer picture symbols at one
time, The act of physically moving the picture
symbols on the mats seems to help people
organise their thoughts In a logical way and
all ows them to take ti me to consider and alter
them if they wish. One man wrth severe learn
ing difficulties used the mats to talk about his
weekly routine. He described clearly, by care
fully choosing and positioning the pictures on
the mats, how he likes gardening best but
does not enJoy the radio which is continually
played in t he day centre he attends.
At present I am using Talking lv10ts with a man
who has 'locked in syndrome'. He uses a low
tech communication book With eye pointing
but finds t he same picture symbols with the
mats al low hi m to produce a more concrete
representation of what he is feeling. His wife
and I have pinned a mat to his wa ll so that,
when he explains his feelings, his choice of PiC
tures can be left on the wall mat and staff on
different shifts can see at a glance what he is
feeling. Because it is visual and attractive the
staff take more notice and know it is his view,
not just someone else's interpretation.
A number of people have expressed an inter
est in using the Talking Mots wrth other client
groups including children wrth language disor
ders, children and adults with learning disabili
ties, patients on acute wards, patients in a long
stay hosprtal and people with degenerative ill
nesses.
The Talking Mots framework is being incorpo
rated into a project triggered by the ChiTdren
in Scotland Act. This requires that children be
consulted in decisions affecting them, and the
project's aim IS to develop training materials to
enable staff who work with children to involve
"""""""""""""" ".."continued overleaf
Case 2 - Betty
Betty had had a stroke which resuh:ed in severe expressive dysphasiaAs she was
about to be discharged ITom hosprtal she was anxious about communicating
once she went home.The Tolking Mats were used to help Betty explain what she
feh: about her communication wfth hosprtal staff, family and friends. She also
described what factors helped and hindered her communication.
This final mat shows that Betty felt her communication wrth hosprtal staff was
OK but that she had more d i f f i c u ~ wrth family and friends. The factors
which she felt helped her were using
drawing
facial expression
humour
wrrting
gesture.
The things which made communication more difficult for her were
people not giving her enough time
too much noise'
toO' many people at once.
She fehr a bit unsure about using her low tech communication book at home.
Using tne' Tolking Mots clearly helped Betty think about her communication
and express her views. These views were used in various ways - to make
suggestions to those who communicated with Betty. to help her communicate
more functionally and to help her speech and language therapist plan her
therapy. The mats helped therapy and ward staff to be aware that she had
definite views despite her severe dysphasia. As a result they took more care
with the noise levels in the ward and took account of her different reactions
to different people.
SPEECH & lANGUAGE THERAPY IN PRACTICE ALfru \ t998 13
ISSN (online) 2045-6174 www.speechmag.com
Me
Case 3 - Jamie
Jamie is a teenager who has cerebra palsy and normally uses a
low t ech symbol book Jamie has no useful speech and is unable
to use his hands for pointing. He eye points t o the left for 'yes'
and to the ri ght for 'no'. Jamie's teacher and school helpers gave
me a list of all his school activities which I transferred into
Boardmaker pictures.
Jamie's m at was pinned to the wall directly in 1Tont of him so he
could eye point to the four emotion pictures to tell me which of
his school actJvrties he liked best whi ch were OK which were
boring and which ones he really hated.The activity pictures were
shown toJamie one at a time allowing him time to indicate what
he fett about each one. Jamie is normally easily distracted but he
enjoyed using the mats, concentrated well and considered each
response carefully
Jamie confinmed this final mat really did express hi s feelings
about school and he w as delighted to show rt to hi s teacher:
h: was very helpful to let hi s teacher and his Mum see the
whole video ofJamie using the mats and Jamie himself has also
looked at rt - over and over again!
There w ere several offshoots. After w atching the video Jamie,
his teacher and his Mum were all more aw are of hi s desire and
abilrty to communicate and the need to stretch him.
Subsequently hi s low tech communication book has had sev
eral new pages added and he is using rt wrth a wider range of
people. His speech and language therapist and teacher are also
looking at a more advanced high tech system as they feel the
A/phoTo/ker does not contain enough vocabulary for him.The
computer w ork in class has been changed to be more moti
vating and, although he still gets physiotherapy. he no longer
gets massage
l
.. continued from previous page . .. .... .......... .... ........ .. .. .
them in making decisions about their own lives
and the services they use. This project is fund
ed by 'Children in Scotland' and further infor
mation can be obtained from Jane Griffrths, tel.
0131 667 4496.
Talking Mats therefore appear to have the
potential to help many people with communica
tion difficulties in many situations. I am exploring
the idea of using them to develop a tool for
assessing people's views in relation to their qual
rty of life. I would welcome comments from
anyone about ways they have used the Talking
Mats or any ideas for further development
For (urther in(ormation contact Joan Murphy,
Research Speech and Language Therapist,
Psycholog'; Department, University o( Stirling,
joan.murphy@stir.ac. uk
Note: In this article, MC stands for augmenta
ti ve and alternative communication and
describes any method of communication which
supplements impaired speech or handwriti ng,
such as a symbol book or electronic aid.
Resources
I. A description of all the issues discussed and
the results of the interJi ews have been written
up in the booklet Improving augmented commu
nication Vlithin an organisation, available from the
MC Research, Uni versity of Stirling, price [10.
2. The Picture Communication Symbols (PCS) are
1981- 1997 Mayer Johnson Co, PO Box 1579,
Solana Beach, CA 92075, USA, and are used
with permrssion.
3. The Talking ots package is availabl e from the
MC Research, UnIVersity of Stifling. price [23.
4.The Lightw ter is available from Toby Churchill
Ltd, 20 Parrton Street. Cambridge CB2 IHRtel.
01223 567 11 7 It is priced at 380 (plus VAT if
applicable).
5. The AlphaTalker is available from Liberator
Ltd., Whitegates, Swinstead NG33 4PA. price
[ 1275 (+ VAT if appli cable). 0
Questions
What do 1",11,; ... " t.A..,.... ..::.
AAC users are given the opportunity to consider,
provide AA
express and change their views and feelings about
that thei complex issues.
In hruAi ,I", When carers see how clients really feel about very
Talking Mats lW specific situations they are more motivated to
carers' perceptio ___ appropriately and make changes where
a "'VII;:7. pOSSible.
Which client groups are
Mats can be adap,ted for anyone who needs to
Although initially intended for AAC users, Talking
Talking Mats most
suitable for? address complex issues.
14 . SPEECH & LANGUAGE THERAPY IN PRACTICE ALITUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
READER OFFER
About the RDLS III:
This new revision of RDLS for the age range 15
months to 7 years is by a team of researchers and
practitioners from the Department of Linguistic
Science at Reading University. Toys, full colour
pictures and finger puppets are all included.
The Comprehension Scale comprises 62
items grouped into I 0 sections:
single words
relating two named objects
agents and actions
clausal constituents
attributes
noun phrases
locative relations
verbs and thematic role assignment
vocabulary and complex grammar
inferencing,
Competition rules:
The completely
revised and
restructured
Expressive Scale
has 62 items in 6
sections:
simple words
verbs, phrases
inflections
clausal elements
auxiliaries
complex
strucures.
,
I. Entrants must subscribe to Speech &Language Therapy in Practice
and only one entry is allowed per subscriber number.
2, Entries must be received by the editor on or before 30th
September 1998.
3. A speech and language therapist nominated by the editor will select
the winning entry but will not know who the entrants are.
4. The winner will be notified by 5th October 1998.
5. The winner must agree to provide either a review ofthe assessment
or a case study based around it to Speech & Language Therapy in
Practice by 20th December 1998.
RDLS III is available (rom NFER-Nelson, Darville House, 2 Oxford Road East
Windsor; Berks SL4 IOF, tel. 01753 85896/ .
Reader Offer Reader Offer Reader Offer ~ ~ I
~ e e c h &Language
Therapy in Practice has
a copy of the Reynell
Deveropment Language
Scales III, courtesy of
NFER-Nelson, for a
winning subscriber. The
authors have radically
updated and revised this
assessment (norrrallL
priced at .375 +VAl)
while retaining the most
popular features of the
original editions.
To enter, simply state,
using no more than 30
woras, why you should
win this equipment.
Send this with your
name and subscriber
number to Avril Nicoll,
Speech &Language
Therap}!. in Practice,
FREEPOST SC02255,
STONEHAVEN AB39 3ZL
or e-mail to
avrilnicoll@sol.co.uk
Please note the winner
will also be required to
review the assessment
or provide a case study
based around it for the
Spring 99 issue.
Offer Reader Offe
SPEI!CJI.'IN'iIQl,fo.GE TI-IERAPY IN pR....cn --E lffiJM! 199- 15
ISSN (online) 2045-6174 www.speechmag.com
C HILD LANGUAGE
From
The success of Dr Deb Gibbard's
Parent-based Intervention
Programme, discussed in the
Summer 98 issue, has led to the
development of an evidence
based service. In this follow-up
article, she explains how.
PORTSMOUTH
HealtlCare ____,.'/a:-.___
T R us T
16 SPEECH & LANGUAGE THERAPY IN PRAcnCE AUTUMN 1998
uring the mid 1980's,
Portsmouth HealthCare
NHS Trust found there
were large waiting lists
and lengthy waits for
treatment for pre-school
children with language
delays. Most children at that time received
direct intervention in terms of their lan
guage remediation and therapists did not
actively involve parents in intervention. It
became evident that a more effective and
efficient method of managing the service
was necessary.
A proposal to offer an indirect method of
service delivery, working through the par
ents of language-delayed children within
gJoups, was initiated. This was to include
control conditions as well as a comparison
with direct intervention. A research proto
col was prepared and formal approval
sought for the research, including that of
the ethics committee. The research was
also registered with the University of
Portsmouth.
In 1986 the research project was underway.
It ran until 1992 and found that parent
based intervention was an effective
method of service delivery. Gibbard
(1994) contains details of the evaluative
research. The speech and language therapy
service then needed to consider how the
findings could be implemented locally and
hence how the service could begin to deliv
er evidence-based health care. Figure 1
illustrates the process that took place dur
ing the research phase of this work.
Following completion of the research
project, the Parent-based Intervention
Programme (see Resources) was developed.
This focuses not only on the theory, back
gJound and rationale for working with par
ents, but also on the practical procedures
and information necessary to implement
the progJamme. The development of this
prOgJamme gave the service the potential
for other speech and language therapists in
the Trust to use parent-based approaches.
A training session was given to all paedi
atric staff working as pan of the health cen
tres team and it was ascertained that sever
al speech and language therapists were
interested in running parent-based cours
es. Their main concerns were the organisa
tional and practical aspects of running
groups. As the Parent-based Intervention
Programme had not yet been published,
traInIng sessions were provided.
Guidelines were also drawn up on issues
such as administrative systems and evalua
tion procedures. Additionally, there were
some concerns over the handling of
gJoups, so individual support meetings
were offered to address these.
During 1996, three paediatric speech and
language therapists ran trials of their own
parent-based intervention courses at the
health centres / clinics where they were
based, with participants drawn from existing
caseloads at these and neighbouring clin
ISSN (online) 2045-6174 www.speechmag.com
CHILD lANGUAGE
ics. These raised a number of issues that
required further consideration, including
the timing of courses, evaluation of the ser
vice development and the information
given to other professionals. It was felt
that health visitors in particular could offer
support to the service on this approach to
intervention, so would need to understand
the rationale behind it and the type of
child it might be suitable for. Such points
raised during the pilot stage (see figure 2)
have been of benefit when considering
how to facilitate service development
across the Trust.
The results of the pilot stage contributed to
the planning process for full sen-ice devel
opment. A series of meetings took place,
providing information on parent-based
intervention to all health visitors across the
Trust. Through individual prior arrange
ment and agreement with their nine team
leaders, a presentation on parent-based
intervention was given at each team's staff
meeting. The health visitors were able to
raise queries and were provided with a
written summar), of the key points.
Alongside this, an annual plan of parent
based intervention courses was co-ordinat
ed. This ensured courses would be run in
a variety of locations across each of the
three divisions of the Trust. Courses were
also planned to take place on different
days of the week, at different times of the
day. In this way, a parental choice option
was included as parents had the conve
nience of being able to select which course
they wished to attend, providing their first
choice was not already over-subscribed.
Figure 3 summarises the senrice develop
ment which has I.ed to evidence-based
practice. Parents who were unable to
attend - or who did not wish to be includ
ed in this method of intervention - were
offered review and advice sessions. This
general care is current practice offered
locally for language-delayed children of
the age range suitable for parent-based
intervention, rather than placing them on
a waiting list.
Further work is unden'llay on continuing
evaluation of the parent-based interven-
Questions
When p-Ianning a new
type of service, what
factors need to be
considered'?
What does 'best
practice' really mean'?
How can robust clinical
effectiveness be
demonstrated'?
tion service devel.opment, making maxi
mum use of the evaluative data resulting
from course implementations. One of the
additional aims of further evaluation will
be to determine relative cost I benefit
ratios of parent-based intervention groups
and general care. Although the effective
ness of parent-based intervention has been
clearly demonstrated (Gibbard, 1994),
there is a need for further experimental
development to demonstrate robust clinical
effectiveness (clinical uials establishing that
research evidence can be replica ted in sub
sequent studies by subsequent researchers,
and is hence generalisable). whilst also
balancing th is with seroice needs and cur
rem practice . Therefor a comparative pilot
study has been designed. which it i - hoped
wiIl lead to a fu ll multj-centre randomised
conuol uial in due our
Although further eva luation of this ervice
development may be angoin, the research
stage of the process identified what Ro eni
(1996) terms a potentially powernll prac
tice. functionally equivalent to best prac
tice. Best practice here represents integrat
iog and applying emerging empirical data
and research into everyday application, in
essence. developing an evidence-based ser
vice. This service development in
Portsmouth HealthCare NHS Trust pro
vides an excellent and very specific example.
Resources
'The Parent-based Interven tion Programme
- a group approach for language-delayed
children' (1998) is available from Winslow.
47.50 (tel. 0800 243755 for orders).
References
Gibbard, OJ (1998) Parent-based
approaches - the case for language goals.
Speech & Language Therapy in Practice,
Summer 98.
Gibbard. 0.1 . (1994) Parental-based inter
vention with pre-school language-delayed
children. European Journal of Disorders of
Communication, 29,131-150.
Rosetti, L.M. (1996) Communication inter
vemion - from birth to thTee. London,
Singular Publishing Group.
Figure I - Research stage
research proposal and protocol
development
!
approval sought from relevant
bodies
!
registration of research with
university
!
research project
!
evaluation
!
writing-up and dissemination of
results
!
service development: pilot stage
(see Figure 2 )
Figure 2 - Service development: pilot stage
consideration of application of
research findings
!
development of Parent-based
Intervention Programme
!
training of all health centre team
paediatric staff
!
implementation: pilot stage
!
evaluation: pilot stage
service
(see Figure 3)
Figure 3 - Service developrnent
review of pilot stage
!
information to all relevant health
professionals
!
co-ordinated annual plan of courses
!
ongoing empirical evaluation
!
EVIDENCE-BASED PRACfICE
Answers
Service planners should consider a system of evaluation,
and aim to provide intervention that is clinically effective
and efficient to run.
Best practice means blending the evidence of emerging
research with the everyday needs of a service and clients.
Research must be shown to be generalisable and
replicable.
SPEECH & lANCUACE THERAPY IN PRAcnCE AUTUMN 199 17
ISSN (online) 2045-6174 www.speechmag.com
REVIEWS
A good
recommendation
Assessing Communication
Oare Latham & Ann Miles
David Fulton Publishers
ISBN 1-85346-503-8 [/299
Thi s is a useful practical book for teach
ers and speech and language therapists
working with chi ldren with severe, pro
found and multiple learning difficulties. It
came out of a culmination of seven
years of working together at Redway
School. Ann Miles is both an experi
enced teacher and a co-ordinator for
alternative and augmentative communi
cation (Me). Her coll eague Clare
Latham is a speech and language thera
pist. The book is based on detailed
assessment of communication. Forms
can be photocopied for use within
schools.
There are four bands: pre-verbal; first
meaning; words, signs and symbols;
expanding communication skills. The
pre-verbal section IS divided into pre
intentional and intentional communica
tion. There IS a sound theoretical back
ground based on the work of Bruner
on the functional theory of language
acquisition. The assessment emphasises
the need for observation and liai son
w h all staff and parents I carers to
form a cohesive picture of the chi ld's
total communication. Other assessment
results for example, Reynell,
Derbyshire Language Scheme - can be
included in the appropriate sections. All
aspects of MC are included such as
objects of reference , SWitch use,
microtechnology, gesture, signs, symbols
and speech output devices in the rele
vant bands. The assessment leads on to
'Guide to Future Planning'.
For this assessment to be successful it
would need to be used throughout a
school or nursery and thus have full
support of the head teache" teaching
and auxiliary staff It draws information
together and helps staff and parents
focus on the child's communication and
bring about more effective future plan
ning. It comes Into Level One of the
National Cunriculum English and can be
adapted to the 5 - 14 CUrriculum in
Scotland.
I plan to share thiS with a nursery
teacher colleague and run a pilot
assessment of the nursery children with
severe and complex difficulties. Thi s is a
good recommendation from a practis
ing therapist who, like everybody el se,
has too much to do in insufficient time.
Ann Gosman is a speech and language
therapist with Orkfley Health Boord
LEARNING DIFFICULllES AUTISM MATH EMATICS
Not a must-have
Autism-POD Creative Ideas During
the School Years - Revised and
Expanded.
Janice I. Adams
Available (rom Winslow
Order ref / 63-2778-98 [1999
This is essentially a resource book for teach
ers, cl inicians and carers who already have an
understanding of autism-POD The author has
collated ideas and strategies from parents and
professionals who have found these approach
es useful. It is relati vely jargon free with the
layout mostly in li st form rather than long
pieces of text
The book is in two parts. Part One is divided
into sections dealing with communication,
social skills, behaviour and coping with transi
tions from one environment or situation to
another. The strength of this part is that It
does not claim to be the definitive guide and
by using the ideas you will solve your teach
ing problems. It does however help you iden
tify types of behaviour you may have faced
when teaching autistic children and offers dif
ferent strategies to try.
I felt many of the ideas would be more applic
able in special schools or units which have a
high teacher I assistant to pupil ratio, as much
preparation and monitoring seems to be
required to put the ideas into practice.There
also seems to be an emphaSIS on individual
rather than group working. Speech and lan
guage therapists may fi nd the strategies includ
ed In the sections "Augmentative
Communication" and "socialisation" of partic
ular interest and value.
Part Two deals with the process of mOdifying
a child's curriculum It also includes sample
worksheets, checklists and plans which may
help in developing a personalised programme
for each chi ld, but some material is perhaps
more appropriate to the Canadian rather than
the UK education system The author gives a
list of contents at the beginning but the layout
of what follows is confusingThere is agreat deal
of Information which I found difficult to access n
any logical way, which was disappointing.
The author suggests a "specialised student
profile" is crucial to the personalised planning
process and gives pointers as to the kind of
information you need to record. I partICularly
liked t he section "Functional life skills".This is
clearly presented and gives ideas, for example
about the ski lls necessary for deal ing with
money or operating tape recorders and tele
visions, and suggests appropriate materials for
teaching purposes.
Thi s book would be a resource "extra" t o dip
Into when one's own creativity is flagging,
rather than a "must have", although I would
probably bring it to the attention of parents
and carers.
Jane Jones is a specialist speech and language
therapist at Royal Aberdeen Children's Hospital.
A challenging read
Elementary Mathematics and Language
Difficulties - A Book for Teachers,
Therapists and Parents
Eva Grauberg
Whurr
ISBN I 861560486 [19.50
Thi s ambitious book aims to set out the learning
characteristics of children with language difficul
ties, relate these to likely problems In the maths
syllabus and increase the reader's repertoire of
methods to helpThe first section works from the
research literature through to teaching strategies.
Chapters look in turn at difficulties in symbolic
understanding, organisational skills, memory and
a selection of other topics. This is a challenging
read but its organisation allows the reader to dip
in with a particular child's difficulties in mind. The
Ideas are densely packed and some experience in
working with language disordered children will
certainly help.
Section two is intended mainly for reference.
With practical suggestions for work in areas such
as early numbe" money and time. At times a
rationale (for the sequence of teaching concepts,
for example) is clarified only in section two and
it would be a mistake to read a topic in either
section alone. Many activities have detailed
instructions for making matenals, incl udi ng a few
useful photocopy masters. There are familiar and
many novel ideas. some Instantly appealing while
others will demand pa 'ence in application. Wise
cautions are often added b t here remain a few
actiVities which a therapist would wish to adapt
slightly before recommending.
The book is intended for professionals and par
ents of children with language difficulties from
pre-school to age 14. In a special ist setting it will
stUTlula e rich dialogues between experienced
teachers and therapists. Mainstream curriculum
co-ordinators and SENCOs should also find valu
able ideas, although their application in large
classes may appear daunting and explicit links
ith the National CUrricu lum are not made.
Therapists giving mainstream support will be
helped to understand the challenges facing the
chi ld and will find theoretical underpinnings for
some frequently given advice. The non-specialist
teacher however' is not guided to approach
speech and language therapists in this area.
Occupational therapists might also have been
mentioned in t he sections en organisational skills.
Parents and t hose worki ng with pre-school chi l
dren may be deterred from sifting out ideas
clearly applicable to them.
An extensive reference list is given. Suggestions
for further reading are made within the text but
might have been usefully summarised at the end
of each chapter: On the whole this is a demand
ing but stimulating book which answers some rel
evant questions for educators of children with
language difficulties.
Linda Edwards is senior speech and language thera
pist at St Piers in Lingfield, Surrey, a residential cen
tre (or children with epilepsy and other special needs.
18 SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
REVIEWS
Very little overlap
Language Intervention in the Classroom
Donna D. Nlermt and Barbaro Culotta
Smgular
ISBN 1-56593-6/9-1 [3350
Speech and Language Difficulties in Education
Pam Fleming, Carol Miller and j annet Wright
Winslow
ISBN 0 863881823 {695
One would expect the bones of these two books to be
similar: Both texts aim at highlighting speech and language
intervention wrthin education; both are targeting a col
laborative approach between the speech and language
therapist and teacher with the emphasis on integrated
a'ld inclUSive school ng.Yet there is very little overlap.
Speech and Language Difficulues In Education is the
simpler book. A mere 38 pages in length, including
the bibliography, the booklet very brieOy introduces
themes which it hopes wil l "promote understanding
between practitioners and result in more effective
provision for the children".
The aim undoubtedly works provided you are happy
JUst to go with the flow. The booklet skims along over
issues such as IndiVi dual Education Plans, ways of
working and the setting of therapy objectives linked
with classroom wOI-k but prOVi des ery Irttl e Oesh on
the bones. If you are searching for practical Ideas and
strategies in order to develop and expand the themes
that It covers, then the book IS less rewarding.
Language Intervention in the Classroom Invites more
thoughtful reading.To illustrate the Indl vidual isati on of
collaborati ve language intervention, the authors have
woven the case study of 'Courtney' throughout the
text.The book is replete with models, adaptive lesson
plans and assessment procedures which contai n
many sound ideas, suggestions and frameworks.
Howevec the chapter embracing phonological con
nections betvveen language and reading may be the
least useful for many speech and language therapists.
It gives a straightforward and up to date appraisal of
t he topic but may well be restating what many prac
titioners already know, and the Ideas It offers for
designing a phonological awareness training pro
gramme are famili ar and routi ne.There are additi on
al drawbacks for I-eaders in the UK. Many of the
examples used to illustrate how to create adapta
tions 0 texts and lessons for language disabled stu
dents, are heavily rooted in American literature and
history. Furthermore, the 'topic web' approach out
I! ed in ItS final chapter may largely be precluded by
our need to deliver within the remit of the National
Curriculum. Nevertheless, there is more than suffici ent
meat in the text to satisfy- the reader:With minor adap
t a ~ o n s , the i tervention strategies outlined are applica
ble, to different subjects across year groups - particu
larly in areas such as enhanCing the comprehension of
discourse and expository and narrative texts.
Acknowledging the persistent vulnerability that chil
dren with spee h and language di fficulties experience
during the school years creates an essential neeo for
collaboration between teachers and speech and lan
guage therapi sts. W ith such a chal lenge and its inher
ent choices, t his text helps to facilitate the interaction
and a Ivate coll ective expertise.
Susan ydeWnghtls a speech and language therapisti
teacher 0[ Dawn House School, Rainwol1h Notts.
EDUCATION CHILD LANGUAGE EDUCATION
An easy read
Let's Talk: Learning Language in
Everyday Settings
Roy McConkey & Penny Pnce
Souvenir Press
ISBN 0285650238
[9.99
Thi s 247 page Jargon-free paperback is pri
marily written with parents of normal, lan
guage delayed or handicapped children in
mind. It is also useful for speech and lan
guage therapy students, newly qualified ther
api sts and therapists with little experience in
earl y language development. The authors
suggest t hat therapi sts or teachers may use
this book, with the accompanying videos, t o
run a parent-child workshop.
It is an 'easy' read, and is suitable as a refer
ence book For example, you may only need
to refer to the section relating to one word
level expressive language development.
Visual indicators are pro Ided along the
sides 0 pages, enabling the rea er to fl ick
through and locate the required secti on.
The texi focuses on expressive language
from pre eroal stage, to sentences In me
main, but does contain one chapter devoted
to understanding, and some exercises in rel
evant chapters whereby a child's level of
understanding can be assessed.
Each of the seven chapters is divided into
three sections, all starting with "On your
marks"; an outline of the chaptec foll owed
by' 'Get set" which covers the assessment of
the child's current abi lities and the rat ional e
for teaching at that stage. The final section,
"Go", provides a range of everyday activities
and ideasdesigned to encourage the child to
use expressive language. A useful summary is
provided at t he end of each chapter
The Do's and Don'ts of teaching expressive
language are firmly stated, ego observe and
add rather than interfere with the child's play
or utterances.
The authors offer a brief overview of what
is involved in learning to talk, and use adult
analogies to help explain why chi ldren may
be experiencing difficulties ;n learning to talk.
Useful checklists to monitor early communi
cation (preverbal) are cont ained, together
with tables showing exampl es of each stage
of language development. Undergraduates
may fi nd these checklists useful as a basis for
compi ling t hei r own during theil- deveJop
mental pl acements
The book's functional approach offers ide s
and activities SUITable for use in an everyday
working environment again, a Important
aid for undergraduates who need Ideas for
therapy, and woul also like to be abl e to
advise and suggest activities for parents to
continue ith. The ideas within this publica
tion are suitable for those children learning
to use Makaton or Amerind si gn systems.
Julie AndrewsIS a paediatric speech and longuage
therapist With RocJ<jngham Forest NHS Trust_
Useful resource guide
A Practical Guide to Running
Language Groups for Children
Working at Key Stages I to 2 I 2
to 3
Ed. j one RiC/l ords
Worthing Pnonty Core NHS Trus t
ISBN I 90213 1 002 / 003 [15 each
These books are written for teachers and
assistants in mainstream schools who have
children 'Nith speech and language difficul
ties in t heir class. It is written in a largon
free style and is set out clearly into sections
to enable it to be used as a qUick resource,
In the fi rst part, each section describes an
aspect of language diffi culty - listening,
comprehension, expression, social com
munication and literacy - and explains why
it occurs and what Impact this will have on
the child's language and learning. It gives
general tips for devel oping these skill s as
well as more speCific ideas that can be
used in groups. Most of thi S will seem very
familiar to any speech and language thera
pist wod<ing with school children.
The second part of the book goes into
110re detail about how to run a language
group and also explains why someti mes
gro ps can be more effectIVe than indi
vidual therapy. The authors have induded
a list of usetiJl resources, Ihere to obtain
them and what language skills they
address. I liked the Idea of this, but felt it
needed a little mOI-e detail as It does not
tell the reader if the Item is a book game,
picture resource or programme.
The book assumes t hat teachers will be
liaising With a speech and language thera
pist in assessing each child's skills and Ihe
type of intervention they need. Thi s coul d
be a useful resource for therapists to
refer teachers to when reporting assess
ment findings. It is a shame that some of
the pages are not photocopiable, as they
would be suitable when offering training
t o teachers.
As a speech and language therapist work
ing in speCial schools I felt many of the
acti lties and suggestions would not be
surtable for children with lower cognitive
abilities and attention spans. As schools re
organise to int egr-ate chi ldren with learn
ing diffi culties there will be an even wider
range of difficulties In the mainstream
classroom than thi s book addresses.
I was disappointed to fi nd the two books
were almost identical, with the addition of
a few extra ad:!viti es in key stages 2 to 3
being the only difference. I would suggest
only purchasi ng the second book as
teachers can Judge for themselves what
would be a surtable activrty for the level of
their class.
Gil/Ion Welsher 15 a speech and language
therapist wiih the Community Team
Learning DlsabJlity, Newcastie upon F ~
SPEECH & lANGUAGE THERAPY IN PRACTI CE Al.I' ruMN 1998 19
ISSN (online) 2045-6174 www.speechmag.com
FURTHER READING
further reading...on adolescents
This regular feature aims to provide information about articles in other journals which may be of inter
est to readers. Following requests from subscribers for material relating to adolescents, in this issue all
the abstracts refer to this age group.
The Editor has selected these summaries from a Speech & Language Database compiled by Biomedical
Research Indexing. Every article in over thirty journals is abstracted for this database, supplemented by
a monthly scan of Medline to pick out relevant articles from others.
To subscribe to the Index to Recent Literature on Speech & Language contact Christopher Norris,
Downe, Baldersby,Thirsk, North Yorkshire Y07 4Pp, tef. 0 1765640283, fax 01765640556. Annual rates
are: Disks (for Windows 3.1, can run on Windows 95): Institution 90; Individual 48. Printed version:
Institution 60; Individual 36. Cheques are payable to Biomedical Research Indexing.
ADOLESCENT CONVERSATION
Lar;on. VL. & McKinley, N.L. (1998) Characteristics of adolescents' conver
sations: a longitudinal study. am,col Lmg Isties and PhonetJcs 12(3).
This study repons a longitudinal invesugatlon o(conversational behaviours with
In normal adolescents (grade 7/age I . 1] years10 grade 12/age 17-1 8 years).
Four males and (our (emales were swdled l nder tv/a expenmental condwons:
talking WIth an un(amillar adu)[ of the Opposite gender and talking with a peer
o( one's choice. The dow docu en/ed pouerns o( normal development durmg
adolescence across macro, mi roo, and midlevels or conversation.
The results re\iealed that adolescents interacung wr/h a peer were more lIkely
10 use a variety of question type s, more (requent (igurarIVe language expres
sions. and nevI a1d abrupt topic shifts, as well as the commUflfca io (unCtions
o(entertammo. getting In(ormatio1, and gettmg the listener to (eel/believe I do
something. Gender-reiated differences revealed that moles used retums to topiC
and the (uncti ons o( e tin the listener w (eel/believe I do so eth,ng and
entertainJllg more (requently than (en1oies. Grode-level differences revealed
three dominant patterns (0) for some behavIOurs a more or less consistent
trend up (or down) across grades(eg negatiVe Interruptions. abrupt topic shifts);
(b) for other beh iours a more or less equal frequency of occurrence at sev
enth and twe1fth rades. Vllth slgmficant differences In one or more mIddle
grades (eg non-sped(ic language, verbai mazes); and (c) (or still others orela
tJVely ffal pattern wld1 similar IrequenCies o( occurrence at all grades (eg. one
appearance negation, giVing InformaMn),
This stud; contrib led to a (oundaOon o(lortglwdinol research on adolescents' com
munlcaaon, and the authors suggested expoflsion o(this research to provrde (or bet
ter comporisofls between normal adoles(enr:s and Ihose with language disorckrs.
IMPORTANCE OF COMMUNICATION SKILLS
Reed,VA. Bradfield, M.& McAllister. L. (1998)The relative i portance of select
ed communication skills for successful adolescent peer interaCtlons: speech
pathologists' opinions. Clinical Unguisucs and Phonetics 12(3).
This swdy invesugated dl e opinions of speech pothologi ts about the relative
importance o( 14 communrcauon skills (or s'Uccess(ul adolescent peer Interac
tions. The speech pathologiSts generallyranked disco rse management skil!s (eg
seleCtlng appr.opriote conversaoonal topics, employing conversational danfico
[Jon and repol( suategles) as relatIVely hlg in Importance and addressee
focused / empa/hic commumcatJon skills (eg conveying opinrons tactfUlly, using
approprime vocal wne) as relatively lower In Importance. There was less con
sensus among the speech pathologists about the importance o(the two
{lgurotive language I skJlls (comprehending humour, using appro
priQte adolescent slang) . in the discussion, the results o( thiS SI dy ere comrast
ed with those of a previous study involving adolescents' opinIons about the rela
we Importance ( selected commumcation skills (or positNe peer relationships.
Oinical Implications o( the findings are discussed, and avenues (or (lIWre
research are suggested
UNDERSTANDING LECTURES
Ward-Lonergan, J.M., Lil es, BZ & Anderson.A. . (1 998) Ustening compre
hension and recall abilities in adolescents wrth language- Ieaming d.sabllrues
and without disabilities for social studies lectures. journal o( Communication
Disorders 31 ( I ).
Ustening comprehenSion and recall abilities (or sooal studies lectures were
examined and compared in 20 adolescent moles with language-learning dis
abilities (Lill) Q11d 29 without disabilities (WD) Sub)ec viewed two SOCial swd
les leaures with comparison and causation expOSitory discourse SLfuctures and
verbally responded to literal and in(erentwl comprehension questions.
Regardless of lecture type or question type, the group wi/h Lill performed sig
niftcantiy more poorly than did the group WD. Both groups responded accurately
o significantly more Inferential ques ons (or the causOOon lecture over the com
pariso. lecture. Neither group demonstrated 0 Significant difference WIth respect
to /heir response accuracy for the literal questions across lecture types
IN"rERPRETING POOR PLANNING
Pentland, L.. Todd. JA &Anderson,V (1998) The impact of head Injury sever
ityon planning abil ity In olesce ce: a functional analysis. Ne ropsyehological
Rehabtlitntion 8(3).
This study aimed {O Invesllgate the Impact of head Injury (HI) on executNe skills
In adolescents. The sample 'nct ded a mild to moderate HI group (n = 17). a
severe HI group (n = 16). and a rna ched control group (n = 17). S bJects were
dminlStered an IQ est and a complex planmng task. requiring odolescents to
plan on unexpected party. QualitatIVe (eatures or planning strategies and elTor
patterns were recorded. S,gni(lcant group differences were 10ted. witil the severe
group making more errors and using less efficienl. S/[alegles on the planning
task No dIfferences were detected between the mild to moderate group and
controls. altho gh performances were no IndicatIVe of mature planning. Thus,
whde a history o( severe HI is associated with de(rCits in planning skills. this IS
no t so (or milder HI Further. care needs to be taken nor (0 over-interpret poor
planning in this clinical population Without consideri g the normal developmen
tal course o( these skills.
LONG TERM IMPLICATIONS
Stothard. S.E, Snowhng, f"I.J., Bis op. DVM. Chipchase, B.B & Kaplan. CA
(i 998) Language-i npalred preschoolers: a follow-up in 0 adolescence.
j ournal of Speech Language and Hearing Reseorch 41 (2).
This paper repons a longJ! dmo1 (o/low4Jp o( 71 adolescems With a preschool
hlswry o( speech-language originally studied by Bishop &
Edmundson (1987). These children hod been subdiVided at 4 years mto those
With nonveroallQ 2 SD below the mean (General Delay group), and those With
normal nonverbal Intellige ce (SLI group).At age 5;6 /he SLI group was subdi
vlded mto those ....-hose language problems hod resolved. a d those With persis
tent Su. The General Delay group Vias also (ol/owed up.At age 15-16 '1ears.
these children were compared With age-matclled normal-Janguage controls on
a banel'! o( tests o( spoken language and literacy skJffs.
Children 'Nhose language problems had resolved did not dlffe! (rom controls on
tests o( ocabu/ary and language comprehensIon skills. Howeve, they per
formed slgni{icanl less well on tests o(phonological proceng and literacy skill.
ChIldren who sull had Significant language drfficulues at 5;6 hod Significant
impai rments In all aspects o( spoken and wntten longuage (unctioning, as did
children classified as having 0 general delay.These children (ell furrher and (ur
ther be ind thell peer group in vocabulary growth over Dme
WORKING MEMORY
Turkstra, LS. (1998) The effect of sti mulus presentation rate on syntax test
performance in brain-injured adolescents. Aphusiology 12(6).
The purpose of thIS study was to explore how estmg procedure inpuences per
formance after tro malic bram injury. and how chis Inn ence vanes as a (une
uon o( the subject's information-processIng abiilDes. Twelve brQln-lnjured subjeCl5
completed three versions of the Listening I Grammar ubtest of the Test o(
Adolescent Language. In the (lrst condition, sentences were presented at 2-sec
ond Intervals, III the second Ot 4-second intervals, and In the third at variable
intervals controlled by rile subject Scores in each condition were correlated with
measures 0 wor ng memory s orage and processing ability.
Performance In the 2-second condition was significandy Influenced by working
men10ry processing abIlIty. whereas performance Tn the 4-second condition VIas
slgni(lcont/y influenced by working memory storage ability. Both aspects of work
ing memory (on!tibuted TO performance in the vanable condition. although onl'l
processing was siglll(lCanl As a group, subjects With better working memory pro
cessing obrlity preferred the variable interval cond,uon, which allowed greater
pexibility. while subjects With poor processmg ability found it more difficult The
results are discussed in terms of clinical assessmen and intervention.
20 SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
I
ADULT NEUROLOGY
.
peech and language therapists have
all used tongue and lip exercises at
some time and found them lacking.
From a single case study we carried
out on our client SL ( see photo
above), vve belie,oe that lack is specificity
Specificrty is an int egral part of
how physiotherapists look at exercise. Each
muscle has a specifi c functi on and, to carry out
that function effectively, it needs to have
strength and endurance. If a muscle has
strength, it has t he power to perform a func
If it has endurance, it can continue to per
form that function without fatigue
"Strengrh may be defi ned as the maximal effec
ti ve force that can be actively exerted by a
muscle in a specific movement" (Galley &
Forster, 1996). In relation to muscle improve
ment it is important to note "strength will not
be increased by the mere repetition of exer
CISe 0 the same intensrty over a period of
time" (Hellebrandt & Houtz, 1958) as repeti
tion can only Increase endurance. "Endurance
may be defined as the ability to continue a par
ti cular dynamic task accurately for a prolonged
period of time" (Galley & Forster, 1996).
As a principle, specifi city looks at 'the everyday
functi onal needs of a patient. It is decided
which muscles are needed for each function
and exercises are then formulated to promote
strength and endurance of the muscles in ques
tion.Therapy can only be effective if both these
areas are treated.
No improve:lnent
Given hi s history. SL seemed an ideal candidate
for a case tri al usi ng the principle of muscle
specificity for tongue and lip exercises. He was
admitted to hospital in March 1997 following a
mid-brain infarct. This resulted in a left hemipl e
gia, dysarthria and dysphagia. He was nd by
mouth initially with nasogastric feeding, then had
a PEG (percutaneous endoscopic gastrostomy)
tube inserted in May 1997 because he was
unable to swall ow. Throughout his five month
Tongue and lip exercises are frequently recornrnenc::led for clients with dysarthria
and dysphagia but can be of limited functional value. Speech and language
therapist Judi Hibberd and chartered physiotherapist C re Ji argue therapists
can maximise success by adopting the principle of specificity.
stay in hospital SL had regular therapy. Including
tongue and li p exercises (for repetrt:lOn five
times each.three times a day). production of sin
gle syl lable words in lists and thermal stimula
tion. Unfortunately, at the time of his discharge
to a nursing home, 'there had been no improve
ment in erther his dysal'thri or swallow.
Although i is well known that muscle strength
reduces with age,it is also claimed that regard
less of age. muscle has the capacity to improve
(Galley & Forster. 1996). As SL was 68, we
thou ht It wool be interesting to bear thi s
claim in mind during the trial.
Modification of excm:ises
We be an by Identifying the specific mu scles
used ,n present tongl e and lip exercises
(DaVies & Coupland. 1997; Perlman & Schulze
Delrieu, 1997) (figure I).
We then modified the exercises to ensure
both endurance and stre gth aspects were t ar
get ed (figure 2).
Figure I - Muscles used
lI..."I. ...
1 . Tongue protrusion Genioglossus and Hypoglossus
2. Lateral tongue movement Intrinsic muscles of the tongue assisted
by the Styloglossus
3. Tongue elevation front Intrinsic muscles of the tongue
4. Tongue elevation back Styloglossus
5. Lip closure Orbicularis Oris
6. Lip spread Zygomaticus Major
Figure 2 - ExerCi ses
.
tt... 1
EXERCISE ENDURANCE STRENGTH
utilising repetition utilising resistance
Tongue protrusion Move tongue Push tongue out against
in and out bowl of spoon held by
someone else
Move tongue into Lateral tongue Spatula held by someone else
movement corners of mouth along lateral edge of tongue.
alternately Move tongue into corner of
mouth against spatula
Tongue tip Lift tongue tip out of Using the bowl of a spoon held
elevation mouth toward the by someone else, lift tongue
top lip tip up into spoon bowl
Back of tongue THERASpoon 4 (Kapitex) THERASpoon 4 placed on back
elevation held over back of tongue, of tongue and light resistance
requiring patient to lift used as patient elevates
t ongue to touch it back of tongue
Lip rounding Patient asked to round Facial flex placed in mouth.
li ps as in 000, then Patient required to compress
relax lips then release it
Lip press Patient presses lips Finger stall applicator put
together and lets go between top and bottom
lips and pressed together
SPEECH & LANGUAGE THERAPY IN PRACTICE ALrrv.M N 1998 21
I
ISSN (online) 2045-6174 www.speechmag.com
Figure 5 up press
ENDURANCE
Press your lips
together and let go
STRENGTH
Put the applicator
between your lips
and press it together
and let go
STAGE 1
Baseline:
Work needed:
STAGE 1
Baseline:
Work needed:
STAGE 2
Today's level :
Work needed:
STAGE 2
Today's level:
Work needed:
STAGE 3
Today's level:
Work needed:
STAGE 3
Today's level:
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 5
Today's level:
Work needed:
STAGE 5
Today's level:
Work needed:
STAGE 6
Today's level:
Work needed:
STAGE 6
Today's level:
Work needed:
ADULT NEUROLOGY
Figul'e 3 - Back of tongue elevation uSingTI-lERASpoon 4
ENDURANCE
Lift back of tongue to
(5" i
touch THERASpoon 4
,
-----.. C I
I
STRENGTH
Push THERASpoon 4
down against ba.ck
of tongue whilst
lifting tongue up
STAGE 1
Baseline:
Work needed:
STAGE 1
Baseline:
Work needed:
STAGE 2
Today's level:
Work needed:
STAGE 2
Today's level:
Work needed:
STAGE 3
Today's level :
Work needed:
STAGE 3
Today's level :
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 5
Today's level :
Work needed:
STAGE 5
Today's level:
Work needed:
STAGE 6
Today's level:
Work needed:
STAGE 6
Today's level:
Work needed:
Figure 4 - LIp rcundrng
I
ENDURANCE
Round your lips Into
the shape for 000
and then let go
STRENGTH
Push the flex
together with your
lips, then relax the
flex
STAGE 1
Baseline:
Work needed:
STAGE 1
Baseline:
Work needed:
STAGE 2
Today's level:
Work needed:
STAGE 2
Today's level:
Work needed:
STAGE 3
Today's level:
Work needed:
STAGE 3
Today's level:
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 4
Today's level:
Work needed:
STAGE 5
Today's level:
Work needed:
STAGE 5
Today's level :
Work needed:
STAGE 6
Today's level :
Work needed:
STAGE 6
Today's level :
Work needed:
For improvement of endurance in a muscle, an
exercise must be repeated a number of times.
Endurance is shown by the number of times a
movement can be repeated without resistance,
To improve strength, some resistance is neces
sary. For t he lateral tongue exercise, where a
patient is required to move their tongue from
side to side, this can be applied by holding a
spatula along the side of the tongue, t '1us
requiring them t o push against the spatula t o
move the tongue laterally. In the lip closure exer
cise, resistance can be appl ied by placing a fi nger
stall applicator between open li ps with the
patient pressing the applicator together with the
lips. The amount of resistance necessary. for any
of t he exercises, is unabl e to be quantified at this
point.
Baseline assessment
The aim of the trial was t o improve both swal
lowing and speech. At its commencement a
baseline of ability was documented.
Swall owing assessment showed SL was aspirat
ing. He had a poor oral phase, so liquids were
passing over the tongue base and into an open
ai rway before he could initiate a swallow
sequence. Compensation of a breath hold
al lowed him to have a few SipS safely. but not
enough for adequate hydration. Food was not
pOSSible because tongue control was so poor.
To set a basel ine of ability for the tongue and
lip exercises the overload principle was applied
(Tr-ew. 199 ). Thi s takes a person beyond their
present p }'Sical ability. Thus SL was asked to
carry out each exer-cise until the muscle was
bred or the therapist observed that the move
ment became UI (Qordrnated.The number of
repetitions achIeVed was the baseli ne for that
exerCIse. There was often a marked difference
In the baselines for strength and endurance.
For example,in the tongue protrusion exerCise
SL had an endurance baseline of ten repeti
tions but a strength resistance repetition limit
of only four This may account for- the di screp
ancy that occurs when a pati ent's exercises are
good but speech is still unintelligible, as speech
requires both strength and endurance. In other
exercises (tongue lateral and lip round), SL
achi eved more repetitions wrth resistance, as
range of movement was more limited with
resistance and was therefore less painful.
Goal setting
Due to the severity of SLS condition, the base
line level of ability for each exercise was very
low. We put a time limit on the case study.
deciding to see what SL could achieve in a si x
week peri od rather than setting him a final
numeri cal target.
The patient. speech and language therapist and
physiotherapist set the goal for each exercise
together weekly. Initially a baseline was estab
lished and agoal agreed for the next week We
considered an increase in each exercise by one
repetition per week an achievable target, so
minimising the risk of failure, We stipulated the
goal must be reached at every practice.
22 SPEECH & lANGUAGE THERAPY IN PRACTlCE AUTUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
ADULT NEUROLOGY
Each exercise had a pictorial representation,
details of the baseline and the expected out
come for each week (examples in figures 3,4
and 5), Achievements were charted weekly.
It was up to the patient. his wife and carers
how many times he practised, for example, ten
times aday,once a day or once every two days,
In this case, he never missed a daily practice
except when all work was abandoned during a
two week period of ill ness, A complete set of
exercises was built up gradually, Unfortunately.
lateral tongue movement had to be discontinued
due to a painful right tempora-mandibular joint.
Functional assessment
SL had shown no functlonal improvement at all
over the five months of inpatient thel-apy 1M )
conventional use of tongue and lip exenctses, In
only a few weeks. hovvever. these spe{:lficity exer
cises saw an improvement in every area (figures
6 and 7) and the functional evidence shows SL's
speech is now intelligible to the degree that
trained listeners - staff and family - can under
stand his needs, His swallow is now safe and he
can achieve hydration orally without his breath
held, He can also now take Itquidised food,
lmpIoving
This is only a very srrtall trial in what could
become a large area of research and we hope
the positive results may encourage others into
research,We are now also looki ng Into imprav
ing SL:s breathi ng using the principle of speci
fi city. Studies show subglottiC pressure is impor
tant in a safe swallow (Eibling and Gross, 1996),
Deep br-eathing exercises can teach a patient
how to increase their inspi ration, therefore
increasing the amount of air in their- lungs,
Duri ng s vallowing, respiration is suspended,
t her- efore the increased air in the lungs
improves the thoracic pressure whrch in turn
will have an effect on the subglottic pressure,
The physrotherapist has given exercises tilising
resistance of the intercostal muscles t o pro
mote rib cage expansion. We are also usrng
'huffing' exercises for control of expiration, the
resi stance bei g the adduction of the vocal
cords to produce the 'h ff'.
We have both found the chance to work with
another profession ver instructive and feel
closer contacts between speech and language
...
Questions
What is the principl e of
[
specificity?
How can a baseline be
measured?
ACHIEVEMENT WEEK 6
NOT COMPLETED AS
TOO PAINFUL
Specificity holds that muscle function can only be
improved by building both strength and endurance.
e number of repetitions made until a muscle tires,
with and without resistance, form baselines .
therapists and physiotherapist s should be
encouraged,
References
Davies, D,V and Coupland, R,E, (1997) Gray's
Anatomy. Longmans Press.
Eibling, DE and Gross, R.D, ( 1996) Subgl ottic
Air Pressure: A Key Component of Swallowi ng
Efficiency. Annals o{ Otology, Rhinology and
Laryngology 105 (4),
Galley, PM. and Forster. AL,( 1996) Human
Movement, An Introductor y Text For
Physiotherapy Students, Churchill Livingstone
Press.
Hellebrandt, FA and Houtz, S,j , ( 1956)
Mechanisms of MuscleTraining in Man. Physical
Therapy Review 36 (6).
Hellebrandt, FA and Hout z, S.j. (1958)
Mechanisms of Muscle Trai ning; the Influence of
Pacing. Physlcol Therapy 38 (5),
Perlman, AL and Schul ze-Delrieu, K. ( 1997)
Deglutition and its Disorders. Singular.
Trew, M. (1997) Exercise for Strength and
Endurance - PrinCi ples Agile Conference,
Guildford.
Resources
THERASpoons are available from Kapltex,
tel. 01937 5802 11 .
Contact authors re- the facial flex a 18
Hodgetts Lane, Burton Green, Kenilworth,
Warwickshire CVI8 IPJ,
Which commercially
tw spatUla, facial flex, finger stall applicator and
available p'roducts are HERASpoons can provide resistance in various
useful for p'rovidinq
.!M!MMtttJtongue and lip exercises.
resistance?
SPEECH & LANGUAGE TH ERAPY IN PRt\CfICE UTUM. 1998 23
ISSN (online) 2045-6174 www.speechmag.com
HOW I. ..
Over 21 million
households in the UK
have aTV licence. Uke it
Howl
View
chH os
television
Louise Taylor is a part-time speech and language
therapist with Walsall Community Trust. Her time is
divided between working with children in a
language unit and a community clinic, and running
parent/child interaction groups for those known to
speech and language therapy at a social services
family centre.
Jennifer Bell is a speech and language therapist in
independent practice working in Mid-Devon.
Angela Dunseath is a non-practising speech and
language therapist with two children aged
five and two.
Lynsey Watters is a specialist speech and language
therapist in the Western Isles Health Board, Health
Care Division. She works with children and adults
with special needs / learning disabilities, children
with complex communication difficulties, and has a
particular interest in young children with social
communication disorders.
or not - and and
language therapists in
generaTdo not - the
reality is that atelevision
in every room is not '
uncommon and many
children have one in
their bedroom. To
make the best of this,
therapists need to be
familiar both with what
is avaDable to chDdren at
the crudal pre-school
OII ........ e and With
t niquesfor
discussing television
withparents.
SU!ests
Thefirst cOllb1butor
ways of
ap roappng the subject
of' eleVlSlon
while three otHers
discuss how the
television progtflmmes
Teletubbies and
Playdays and certain
videos can be used
sensib to make a
= n ' ~ ~ ~ n d
language development
24 SPEECH & LANGUAGE THERAPY IN PRACTICE Aun rMN 1998
ISSN (online) 2045-6174 www.speechmag.com
HOWl...
WorkingwiOt parents
" nt-childirJteraqiQn I\Q1 by la ,rt.Pan:nts condude
aHhouehthe (.CJn atron, it cannot
rep cethe1t role astheir child's mmlIDlcation teacher.
== I find it important to be familiar with see it's a good impaner of knowledge and gives good role models
Teletubbies, Rosie and Jim, Brum or whatever for the child, but is generally poor at encouraging effective com
happens to be the latest children's 1V craze, munication between parent and child. It is a one-way channel, 1V
even if it is in name only, with a few sketchy --+child. There is no need for turn-taking, good listening, appropri
details to aid conversation with a pre-school ate eye contact / body language, the ability to talk about the same
client. (Though do beware if you call Po thing, talking clearly, understanding what is being said or being
"Laa Laa" by mistake... ) That does not understood, the prerequisites of good communication.
mean becoming a Tubby addid yourself. In our All eight parents in my 'last group reponed using the television as a
family we rarely have the television on, so most of our infonna ' baby-sitter', switching it on to keep the children occupied while
tion on charaders comes from friends, family or magazines. they carry on with their jobs. This reinforces its role as information
However, we do need to take a sensible approach to toddlers and - provider and entertainer but not as a teacher of effective commu
dare I say it - babies who are avid 1V watchers. Throwing our hands nication. The parents then see how, if it is used as a shared focus,
in the air and saying "Oh no, not another Thomas the Tank fan " or either when it's on or after the programme has finished, they can
dismissing parents' comments such as "He doesn't really play, only encourage good communication skills.
watches videos, he's ever so good at working the video recorder"
will only cause us more difficulties. It is a fad that the majority of Distracting
children will have exposure to 1V / video at some point in their
Another issue discussed is how distracting the 1V can be. A number
day. Rather than ordering a diet of no television for the child, it is of parents have the television on all day, regardless of the pro
more realistic to show how it can be used more effectively. gramme. They report that their children play but repeatedly turn to
One of the ways I do this is during a six week group for parents of chil some way towards strengthening the parent-child relationship and
dren who are new referrals to the service. The children attend too, giv
encouraging good communication between them.
ing us the opportunity to assess speech and language skills and social So next time a parent tells you their child "loves the Teletubbies",
and play development and to begin remediation as appropriate.
don't throw your hands up in horror but discuss how this time may
Alongside this, the parents discuss various topics led by me. These be spent more effectively.
include communication, attention / listening, tum-taking and Ian
Resources
guage and play development, the main thread being to encourage
r
good parent / child interadion.
For information on training in the parent-child interadion ther
apy approach, contact Sarah Hulme or Keena Cummins, Principal
A one-way channel
Speech & Language Therapists at Hunter Street Health Centre, 8
The subject of television is raised along with others such as dummy
Hunter Street, London WC1 1BN, tel. 0171 5304336.
sucking, the effect of a child's place in the family and other sib
Figure 2 is based on Reynell's levels of allention as quoted in
lings, various toys and books. The parents are encouraged to con
Working with Children's Language by Jackie Cooke & Diana
sider if the television is a good facilitator for communication using
Williams, ISBN 0 86388 025 8, available from Winslow price
a successful communication checklist (Figure 1). Generally they 22.45.
SPEECH & LANCUACETHERAPY IN PRACTICE AUTUM 1998 25
Figure I - Successful communication checklist
COMMUNICATION SKILLS
If your child Ie good at the68 thlnge put a t ick ,/
If your child ie not eo good at t hem put a dot.
CONCENTRATION
EYE CONTACT .,/
UNDERSTANDING / 60DY LANGUAGE
.-.-// --
--
\
TALKING CLEARLY .---- (SUCCESSFUL COMMUNICATION)
- TAKING TURNS
TALKING A50UT - '--
THE SAME THINGS
\
LISTENING
HEARING
Figure 2 - Approximate attention levels (see Resources)
Levell (0-1 year) Extreme distractibility when child's attention flits from one object,
person or event to another.
Level 2 (1-2 years) Child can concentrate on a task of his own choosing. His attention is
Single-channelled and he must ignore all extraneous stimuli.
Level :3 (2-3 years) Child cannot listen to adult's directions while he is playing but he can
shift his whole attention to the speaker and back to the game with the
adult's help.
Level 4 (3-4 years) Child must still alternate his full visual and auditory attention between
the speaker and the task but he now does this spontaneously.
Level 5 (4-5 years) Child's attention now two-channelled, that is, he understands verbal
instructions related to the task without interrupting his activity to
look at the speaker. His concentration span may still be short but he
can be taught in a group.
Level 6 (5-6 years) Auditory, visual and manipulatory channels are fully integrated and
attention is well established and sustained.
see what is on the television, in
effect, being constantly distracted
by both the auditory and visual
stimulation it gives oul. Another
common comment is that their
child ignores them when the 1V is
on. We discuss this and I relate it
to how allention develops (Figure
2) so they understand the chil
dren may not be able to share
their attention with the television
and their parents talking.
As the course progresses, the par
ents build up for themselves a
framework of how to use the tele
vision in the most positive way by
a) using it as a shared focus
b) reducing the time the televi
sion is on and
c) being aware that their child may
not be able to cope with more than
one focus of attention.
Generally the parents come to their
own conclusions that the television
provides us with some useful and
important infonnation but is not a
communication teacher - that is
their role. There will never be a real
substitute for quality time spent
playing and talking with children,
but time spent watching a child's
favourite programme together and
talking about it afterwards will go
ISSN (online) 2045-6174 www.speechmag.com
It
Dipsy
HOW L.
ieletubbies has a
combined daily audience
of just under two million.
Playdays has a daily
average of one and a half
million viewers. ihese
figures. from BARB
(Broadcasters' Audience
Research Bureau).
exclude viewers aged
under four.
Fiends or friends?
diffirult to remember a that has
stimulated as mltCtl debate. BeD speech and
language therapists should rejOice In the Thletubbies.
Although they have been with us for so lit file. [n this land naughtiness is accepted and dealt with by humour
tle time, already they seem to be a part of and good sense.
life; for some toddlers they are the only
'proper' speech and language facilitator in Semantic links
their lives. I am talking of course about When the windmill appears we recognise it signals, as usual, a visit
the Teletubbies. Have Po, Laa Laa,
to the real world of everyday children. In this experience children
and Tinky Winky ever been on a Hanen
share their activities which add to the viewers' ideas of the wider
course? It seems probable - "Observe, Wait, Listen" world and to their vocabulary. Enjoying the new, we make patterns
(Manolson, 1992). Here we have the observant Baby Sun watching and connections and forge semantic links. There is always a begin
over and orchestrating proceedings, while the Teletubbies wait for
ning, a middle Jnd an end to these interludes and when we see the
each other, take turns and give each other time to talk; "listen"
sequence again there is always something new we missed the first
say the speaking tubes, then "listen" and "listen" again; repeti
time round.
tion is crucial for Teletubbies. Parents often say "but it's so boring,
The programme itself is a useful vehicle for teaching colour, size,
it 's the same thing over and over" - much like talking with emer
shape and number concepts and places due emphasis on rhyme
gent speakers, unfortunately.
and music, both crucial for language and learning. At other times,
Teletubbi es just watch and demonstrate the value of being quiet in
Familiar and regular the company of another person. jung would approve. When a
Moreover, Teletubbies are interesting and enthusiast.ic whether the young child settles down to watch with a parent s/he can begin the
subject matter is tubby custard or hiding from the scary bear. The long and difficult task of learning to attend and concentrate at an
story line is familiar and the routine regular, much like a day in the early stage in life; watching wall to wall cartoons does not offer an
life of a fortunate toddler, and there are equivalent training.
unexpected treats. Teletubbies enjoy high People sometimes say Teletubbies holds
self esteem; they support each other and Teletubbies is broadcast on BBC2 children back from speaking properly. I
are co-operative and considerate, useful each Monday to Friday at 7am and suspect. with guidance from an aware
attributes for living in a family. They like lOam. This programme is appropriate parent, any child will move to a more
group hugs and laugh a lot. They eat at for an age range of eighteen months appropriate activiry at the right time
the same time as each other and converse and over. even - for some children - up simply because s/he wants to find out
around the table; this is wonderful for to four years. After this. the average more than the Teletubbies can teach.
speech and language development. child would be better occupied taking Speech and language therapists can
Socially, Teletubbies will soon be ahead a walk in the park and talking with an rejoice that, at long last, there is a pro
of us unless we watch out. Even little Po interesting adult. The programme is gramme on TV that not only can be used
can succeed and enjoy home life in such best watched in the company of a as a teaching aid for parents, but actively
company. Everyone can ftnd one parent who is prepared to talk about fosters speech and language develop
Teletubby to identify with: active Po with It afterwards and also play the games ment in the young child.
her scooter, Laa Laa always dancing and and sing the songs again and again
singing and who loves her ball, dark and yet again.
Resources
skinned Dipsy sporting a high hat, and Manolson, A. (1992) It Takes Two to
the tall, sensitive Tinky Winky with his
Talk. The Hanen Centre: Toronto.
elegant red handbag. The combined elements offer endless scope Information on training in the Hanen approach is available from
for stories which are always familiar but can change when new sit
Anne McDade, The Hanen Program UK / Ireland, 9 Dungoyne St,
uations are added to what is already known. Verbs have a high pro-
MaryhilL Glasgow G20 aBA, tel. 0141 946 5433.
26 SPEECH & lANGUAGE THERAPY IN PRACTICE AunJMN 1998
ISSN (online) 2045-6174 www.speechmag.com
HO\V I. ..
in
When
Dynamic viewing
chDdren
approached to write about a quality
children's programme, a suitable subject didn' t spring imme
diately to mind. Arguably this could be due to a lack of imagination
on my part, or perhaps it is symptomatic of the relative scarcity of
stimulating viewing available to the younger audience. There are
those who do not allow their children any exposure to televi sion,
and admittedly some of the offerings are appallingly bad. However,
banning TV is a little like prohibiting sweets in that it becomes the
forbidden fruit and develops a mystique and desirability far beyond
its worth. There is no reason why a carefully selected, age appropri
ate programme viewed with an adult shouldn't be a good language
learning opportunity for a child. ,.._r--------...._______--, gest they join in with a s ng or game. This
A non-threatening context
For the two to five year age bracket,
cal bias with role-play, action rh ymes and
familiar songs, whilst on Thursdays at the ' Patch Stop' Peggy visits
an outdoor location such as a park beach or farm. Although each
episode can be viewed as a self-contained unit, featuring the famil
iar puppet characters throughout the series provides continuity. In
this way the programme offers a good balance between pre
dictability and novelty which gives children a great many opportuni
ties both to comment on the familiar and perhaps experiment with
new vocabulary and sentence constructions in a non threatening con
text. Even before the programme begins there can be opportunity for
discussion. My children enjoy speculating about which stop it will be
today and whether their favourite character will be featured.
Infinite possibilities
The puppet characters are cleverly thought out, each with its own
distinctive traits. Poppy the talkative cat loves being read to and
will often interject during a story to request clarification or stress a
key word. Why Bird, as the name suggests, is continually asking
questions whilst Peggy the doll has a penchant for reciting rhymes
and a creative flair, frequently making simple things that can easi
ly be replicated at home. Once children can identify with the char
acters there are infinite possibilities for introducing new experi
ences in a familiar context. This is exploited to the full, with the
characters visiting I ca ti on such as the hospital, airport and den
tal surgery, provi di ng lo ts of opportunity for discussion afterwards.
The characters are also important for introducing humour which I
feel is vital, as a giggling child is invariably a relaxed child who is
more likely to relate the humorous experience at a later date using
whatever language sjhe h s avai lable.
Playdays also makes good u e of r Ie-pia scenarios to act out
familiar stories and songs and I fi nd ch il dren are keen to replicate
and develop these themes fu rther_Indeed we have a bag of dress
ing up clothes which is frequent! unearthed after the programme.
The presenters and puppets often addr ss the viewers directly, to sug
1 feel it is vital that an adult views the episode with the child to
become familiar with the characters and format, thereby providing
a frame of reference for discussion. Such shared attention in a rest
ful setting creates an environment in which children feel free to
contribute but are under no direct pressure to speak The adult can
also answer any queries as they arise and help with additional activ
ities. In my experience the follow up work stimulates more varied
conversation than the programme itself.
In my view, children's TV exposure should be selective, stimulating
and shared with an interested adult and not a solitary substitute for
more fruitful occupations. To impose a blanket ban on TV viewing
denies children exposure to their own popular culture and renders
them speechless at nursery school when asked about their favourite
Teletubby or Playdays stop. For those unable to sleep at night
haunted by the repetitive strains of the Teletubbies theme tune,
Playdays may offer a viable alternative. It is a thoughtful and varied
mix of story, song, role-play and creative activity that is inherently
appealing to children, and a little healthy competition for Tinky
Winky and co. When children are encouraged to be dynamic rather
than passive viewers, such programmes can potentially provide a
rich language learning experience as well as a useful stimulus for
even more rewarding extension activities.
seems to be very effective. as children in
this low pressur :.ituation are more likely
to participate. It's ill nazing how well my
children will respond to a request from
Poppy the cat
l
Each episode invariably
ends with a suggestion for follow up activi
ties related to the day's theme. This could
involve pretend play, reciting a story or a
craft acti vity.
Conversation stimulated
One example is Playdays. It has three central
puppet characters: Poppy the cat, Peggy the
rag doll and an inquisitive parrot called
Why Bird along with a supporting cast of
equally colourful hu mans. There is a
Playdays bus that visits a different 'stop'
each day and the programme develops
along a new theme. On Wednesdays, for
example, the ' Roundabout Stop' has a musi
Playdays is screened on BBC
Television on weekday afternoons
at 3.30 pm. BBC Children's
Magazines also produces a
Playdays publication which
complements the programme and
is compatible with the early stages
of the National Curriculum.
Valuable videos
Lvnsev \NiJtters wants us to adcJe Parents in Jhejr selection of suitable videos
C:1hd subJec:tingthem to the pressure of
unrealistic expeaauons.
Have you seen Pingu? You have? So what's ing services, but let's look more closely at what they offer.
it all about then? I have been exposed to J spend much of my time working with very young ch ildren. aim
Pingu videos in one of my workplaces for the past ing to develop preverbal slGlls such as listening, anti cipation rum
four and a half years. and am still unclear as to whether he is speak talGng, vocal and motor imitation and gesture both in an info
ing some Antarctic dialect or just nonsense. It is easy to disregard way and with formal signing. To develop these, carers are encOlli
videos and children's programmes as non-constructive childmind- aged to create an environment which includes repeti tion. rouun
SPEECH & LANGUAGE THERAPY IN PRAGnCE AuruW, 199- 27
ela Dunseath finds the mix of story, roie1'lay and creative activity
ydays makes it one of thefeN quality programmes available to young
ISSN (online) 2045-6174 www.speechmag.com
HOWL
opportunities to communicate,
so on. Many parents and carers find it difficult
to create such an environment consistently,
due to pressures of work, family and time. We
should not increase the pressure by having
unrealistic expectations of carers; if the reality
is that children will spend much of their time
watching 1V and videos, we should perhaps
guide parents in their selection.
When considering language development,
professionals may question the value of pro
grammes / videos in which the characters do
not communicate using speech, giving the
reason that children need an accurate model
to develop accurate speech. (Isn't this one of
the major concerns about Teletubbies1) Few
of us over thirty will fail to recall The
Clangers, those pink knitted inhabitants of a
small blue planet, whose system of communication consisted of
high pitched whistling. Remember the Soup Dragon, Iron Chid,en
and blue string pudding? My argument is that they remain in our
long-term memory, although they did not utter a word of recog
nisable speech. (Interestingly, there is anecdotal evidence that
adults, when watching The Clangers without the voice-over, can
understand what they are saying, and speakers of different lan
guages are convinced The Clangers are speaking their language. For
more information see www.Clangers.co.uk - a truly fascinating
website, where I feel sure you will spend many a happy houri)
Voice-over essential
The fundamental difference between these two examples, and the
reason Tdo regard Pingu as inanity whilst waxing lyrical about The
Clangers, is the existence (or non-existence in Pingu) of the voice
over, which can help create that 'environment' essential to the
development of pre-verbal skills.
The video environment can and should encourage:
1. Repetition
For young children, repetition is crucial. People who walk past my
dinic room must shake their heads in disbelief as they hear the
same words and phrases over and over. We know that 'scripting'
techniques in therapy increase comprehension and confidence to
communicate - videos which allow the child to hear the same
words, phrases, songs and stories are bound to have the same
have purchased the Makaton Nursery
Rhymes video. Even the children who, for
whatever reason, do not continue using
Makaton, will remember the signs for the
animals Old Macdonald had on his farm.
Mainstream nurseries attended by children
using Makaton often use this video as a suc
cessful introduction to signing for the other
children - the fact that it can be used at a reg
ular video time, in place of Rosie and jim or
Thomas the Tank Engine, gives it immediate
credibility for all children, and signing is thus
accepted as a valued form of communication.
4. Anticipation of routines / events
Many children with social communication
disorders spend time watching the same
videos repetitively, needing the familiarity
and routine they provide. [know of a child
with autism who will not watch Teletubbies on 1V but will watch
the video from beginning to end, anticipating events within the
video in a way she is unable to do at any other time.
5. Imaginative play
The story lines from videos can be re-enacted and extended by chil
dren, perhaps more easily than those in books, because the images
are vivid and motivating. (J am sick of listening to my own three
children arguing over who will be Tinkerbell, and who, like Peter
Pan, will be able to leap from the top bunk and fly to Never Never
Land. This play was meaningful and exciting even to my two year
old who, whilst initially being dragged into it by his older siblings
who needed a teddy bear-carrying Lost Boy, was soon well into the
swing of it.)
6. Interest in books
The Bookstart Project, started in 1992, suggests that babies and
children who are introduced to books at an early age go on to do
better at school in a number of areas of the curriculum, induding
Speaking and Listening, than children who do not have this expe
rience. Videos often link with a whole host of related books which
can provide the initial motivation and interest in books.
Reducing the guilt
Parents who are aware of their inability to provide their children
constantly with the type of st.imulating environment they feel they
should have, frequently express guilt about switching on the video.
effect. Many younger parents
do not remember, or perhaps
never knew, the nursery
rhymes and action songs we
suggest they sing with their
children. Perhaps videos
which have interesting, excit
ing characters and a clear,
unambiguous voice-over, can
fill this gap.
2. Imitation
Those of us in Scotland will be
familiar with The Singing
Kettle, a children's band from
Fife, whose jovial songs rouse
, the most reticent of children
into imitating the actions.
Similarly, numerous chil
dren's first attempts at vocal
imitation may be encouraged
by repetitive voice-over, ani
mal noises or vocalisat.ion on
video.
3. Signing
Many parents of young lan
guage delayed children who
have begun using Makaton
Practical points:
1. TV is here to stay and is part of children's culture, there
fore we should encourage sensible viewing habits rather
than a blanket ban.
2. Constant exposure interferes with the development of
selective attention and should be discouraged.
3. Parent child interaction groups facilitated by a
therapist enable parents to make informed decisions
about television in their household.
4. Good quality children's programmes provide information,
entertainment, good role models and, most importantly
for language development, extension activities.
5. When therapists recommend programmes and videos
they should consider factors such as a voice-over,
repetition, signing and the opportunities they give for
imitation, anticipation, imaginative play and fostering an
interest in books.
6. The value of television is increased when a child watches
it along with an interested adult.
I believe we can reduce this
guilt and support them further
by explaining the value of
videos in the development of
early language, so long as they
are presented in an environ
ment which fosters and
encourages social interaction
at other times. We should then
subtly suggest Pingu should be
exterminated, and quick..
Resources
The Makaton Nursery
Rhymes Video is available
from MVDP, 31 Firwood Drive,
Camberley, Surrey, tel. 01276
61390 price f8.99 + f3 p&p,
cheque to MVDP with order.
Information on Bookstart
from Book Trust, Book House,
45 East HilL London SW18
2QZ.
For a catalogue, contact The
Singing Kettle at Post House,
Main Street, Kingskettle, Fife,
tel. 01337 831543. 0
28 SPEECH & LANGUAGE THERAPY IN PRACTICE AUTUMN 1998
ISSN (online) 2045-6174 www.speechmag.com
.-.
.. .
IEVENTS
5 - 6 September 1998
Voice Care Network UK
Residential Annual Study
Meeting
Venue: Birmingham
Includes: Breathing, asthma,
non verbal behaviour in com
munication, classroom
acoustics, practical
workshops and AGM.
Details: Voice Care
Network, 29 South bank
Road, Kenilworth, Warks
CV8 1LA, tel. 01926
864000.
21 - 25 March 1999
AFASIC Third International
Symposium - Speech and
language impairments from
theory to practice
Venue: University of York
Speakers include Dorothy
Bishop, Joy Stackhouse, Paulo
Tallal, Susan Ellis Weismer,
Gino Conti-Ramsden,
Margaret Snowling and
Michael Rutter.
Details: AFASIC Symposium
Secretariat 29 Hove Park
Villas, Hove, BN3 6HH, tel.
01273 381009.
NB Abstracts are invitedfor
contributions to free
communications Of papers,
posters, videos and work
shops. Contact the Symposium
Secretariat for details. The
closing date is 76th October
7998.
- r' II,tl d 10 I[ tllrn
lor an a Ie mCllt to I11dkl'
Speech a Lilng Itlg
In Pra(tiCt pullt(ilY
avalldt'it' to those aUpntJlllg
Contributions to
Speech & Language
Therapy in Practice:
Contoa the Editor {or
more information and / or
to d,scuss your plans.
Please note:
articles must be o{
practical use to dlmdons
use case examples and
list usefUl resources
"length IS generally
around 2500 words
copy on drs!< if
possible
keep statistical
m{ormauon to a minimum
photographs and
illustratJOns will be retumed
:.. :... . .. - . ..
POSTCODe:
POSTCOOE:
::t
: '- .
ISSN (online) 2045-6174 www.speechmag.com
MyTop Resource
Julie Coley, a Specialist Speech and Language Therapist
working in an infant and junior language unit in Burton-on-Trent for
Premier Health Trust, has developed the product 'Mitten Mouth'. Readers
with ideas for books and equipment are encouraged to take them further.
I am sure as therapists we have all, from time to time, thought of
ideas for equipment which would be useful in our job. Perhaps my
experience will encourage you to take your ideas one step further
and make them work.
I have always been interested in and reasonably good at simple art
work in therapy. In my early years as a speech and language thera
pist my cupboards were full of home-made games and cardboard
cut-outs. As the years went by, family and
"Mitten MVlltll lS
time constraints - and daily diary sheets!
prrnlirlg fl ) be a
came along and my therapeutic aid pro
lIlutiuating <md aml/slllg
duction diminished. However, a couple of
Ilislla/ aid Whl d l (<II!
years ago, while trying to motivate some
a/so he I/s(!d a/o/lgsllle
children working on oral skills in the
olher lIk1faial. (I is larg
infant language unit, I invented a free
er dIal! U(t' ./I1d lit'l)'
standing mouth with a glove puppet
fi mct/ol 1,71. Olildrm c.m
tongue to encou rage exercises for devel
also h,7I'i? ,/ tlll"l l .I!
oping strength, range and direction of
helllg d}t' tOl/glte, "
tongue movements. It occurred to me
II.. I I
that, if my 'mouth' was more permanent
l ... m (.1,... 1 ':TrJi .. 1
I tl
and durable, it might be
a useful resource for
other therapists, so I
decided to look for a
company to produce it.
I sent a couple of pro
totypes to Winslow
and LOA. Winslow
described it as "an
innovative product"
but, as they are
publishers only,
Tongue. The director suggested
Mitten Mouth and one year
later it was in the catalogue.
Mitten Mouth is designed to improve oral
I /.l./I't /111, 1.1
awareness and to teach and improve tongue
\llftcn \ [, ml/'.1
movements. It is particularly useful with
I 'iT) ,1Ild
young children who have poor attention skills
II, 'U'
and who lack motivation. It works well with
')/l!i}lIl[lIilt'IlI.
children individually and in small groups. All
(JlIldrell IllId If
the children can focus on the larger-than-life
1I1l:1'1'.\llIlg /I) I. )uh
mouth and can clearly see the tongue move
.It. md It IS d
ments.They respond to the character and are
hltt
more willing to imitate it than the therapist.
('Ift'.:ill'l' 11',1,\ r It
Mitten Mouth can also help older children
dellli
with persistent speech problems (see case
111'.1! 1.. ill .11/11
examples).
Further information
Irtitld,1l1 '"
Mitten Mouth is available from TFH, 76 Barracks
Road, Sandy Lane Industrial Estate, Stourport-on- {ltd"';:C.
\AI h' !-IeI.." 11 "lk,.,.m ... llkc-
Severn, vvorcesters Ife . T" II.
OY 13 9QB, tel. 01299 Case exam SI . . , I f<?11I{,r Heat .
827820, price 44 (+ David is si pIe 2
'I.
'AT) 10% & x years old w' h
n + P p. dyspraxia, D 'd h It severe articulat 0
Winslow is at Telford tongue mo aVI ad a severely limited rang ory
0 vements and k e
R00, d BlCester, xon els. He wa spo e using only YO
OX6 OTS I 01869 s poorly motiv d w
' te. mUch success. Mitten M ate and hadn't had
244644 h
. friend and h . out has become h'
e IS now mo '1 . IS
LOA
: contaet
P
ro
d
uet attempt and peri re WI ling and able to
O e V e I 0
P
m e n t orm non-speech d
to
ngue movements U. . an speech
Secretary, LOA, conjunction With Sing M,tten Mouth in
Abbeygate House, Dyspraxia Programme s:eehch and the Nuffield
East Road, and Itl. e as acquired In!, III
Cambridge CB I I DB,
tel. 01223 365445.
Reference
Connery, V.M. et al (1992) Nuffield Centre Dyspraxia Programme.
London: RNTNE Hospital.
ISSN (online) 2045-6174 www.speechmag.com
Potrebbero piacerti anche
- Mount Wilga High Level Language Test (Revised) (2006)Documento78 pagineMount Wilga High Level Language Test (Revised) (2006)Speech & Language Therapy in Practice75% (8)
- Nursing Care Plan For Risk For Aspiration NCPDocumento5 pagineNursing Care Plan For Risk For Aspiration NCPderic100% (8)
- Oral and Written Language Scales Listening Comprehension and Oral Expression (OWLS)Documento13 pagineOral and Written Language Scales Listening Comprehension and Oral Expression (OWLS)alessarpon7557Nessuna valutazione finora
- Tongue Jaw Dissociation ExercisesDocumento5 pagineTongue Jaw Dissociation ExercisesZiva100% (1)
- Speech & Language Therapy in Practice, Spring 2001Documento32 pagineSpeech & Language Therapy in Practice, Spring 2001Speech & Language Therapy in PracticeNessuna valutazione finora
- Ylvisaker HandoutDocumento20 pagineYlvisaker HandoutSpeech & Language Therapy in PracticeNessuna valutazione finora
- In Brief (Spring 11) Dementia and PhonologyDocumento1 paginaIn Brief (Spring 11) Dementia and PhonologySpeech & Language Therapy in PracticeNessuna valutazione finora
- A Practical FocusDocumento2 pagineA Practical FocusSpeech & Language Therapy in PracticeNessuna valutazione finora
- Easy-to-Swallow, Easy-to-Chew PDFDocumento259 pagineEasy-to-Swallow, Easy-to-Chew PDFChatterjee Nikita100% (2)
- Chapter 22: Nutrition and DigestionDocumento114 pagineChapter 22: Nutrition and DigestionIrish Mae T. Espallardo100% (1)
- Maxillofacial Prosthetics Theory and PracticeDocumento305 pagineMaxillofacial Prosthetics Theory and PracticeMostafa Fayad100% (11)
- PLE 2019 Surgery Questions and AnswersDocumento30 paginePLE 2019 Surgery Questions and Answersdickson78% (9)
- Acute Gastroenteristis Case Study GRP 3Documento22 pagineAcute Gastroenteristis Case Study GRP 3juel_navarro86% (7)
- Speech & Language Therapy in Practice, Autumn 2002Documento32 pagineSpeech & Language Therapy in Practice, Autumn 2002Speech & Language Therapy in PracticeNessuna valutazione finora
- Speech & Language Therapy in Practice, Autumn 2010Documento32 pagineSpeech & Language Therapy in Practice, Autumn 2010Speech & Language Therapy in PracticeNessuna valutazione finora
- School-Based Play Therapy: Second EditionDocumento12 pagineSchool-Based Play Therapy: Second EditionWuDennisNessuna valutazione finora
- 122 OralMotorDevelopmentalMilestonesDocumento2 pagine122 OralMotorDevelopmentalMilestonesMaithri SivaramanNessuna valutazione finora
- BedtimeroutineDocumento1 paginaBedtimeroutineapi-538947968Nessuna valutazione finora
- 201 TypesofArticulationErrors PDFDocumento2 pagine201 TypesofArticulationErrors PDFEndiNessuna valutazione finora
- Speech & Language Therapy in Practice, Winter 2009Documento32 pagineSpeech & Language Therapy in Practice, Winter 2009Speech & Language Therapy in PracticeNessuna valutazione finora
- Speech & Language Therapy in Practice, Winter 2004Documento32 pagineSpeech & Language Therapy in Practice, Winter 2004Speech & Language Therapy in Practice100% (1)
- Let's CHAT: Communication Help and Awareness Team (CHAT) Diane CairnsDocumento4 pagineLet's CHAT: Communication Help and Awareness Team (CHAT) Diane CairnsSpeech & Language Therapy in Practice100% (2)
- Sample Treatment PlanDocumento3 pagineSample Treatment PlanLiza NaumannNessuna valutazione finora
- 460 VoicedvsVoicelessDocumento2 pagine460 VoicedvsVoicelessNOR-ALI SOUDNessuna valutazione finora
- Sometimes Stutter PDFDocumento44 pagineSometimes Stutter PDFPrajith VijayanNessuna valutazione finora
- Only A Story?Documento4 pagineOnly A Story?Speech & Language Therapy in PracticeNessuna valutazione finora
- Speech & Language Therapy in Practice, Summer 2005Documento32 pagineSpeech & Language Therapy in Practice, Summer 2005Speech & Language Therapy in PracticeNessuna valutazione finora
- Info For Dyslexic Students SloveniaDocumento32 pagineInfo For Dyslexic Students SloveniaskumavcNessuna valutazione finora
- Expressions of the Mind in Words: Writings by a 9 year old kidDa EverandExpressions of the Mind in Words: Writings by a 9 year old kidNessuna valutazione finora
- Word Meaning Map II PDFDocumento0 pagineWord Meaning Map II PDFBrian HaynesNessuna valutazione finora
- Isilimela Hospital Speech Therapy DepartmentDocumento2 pagineIsilimela Hospital Speech Therapy DepartmentSuné GreeffNessuna valutazione finora
- IDDSI Framework Testing Methods 2.0 - 2019Documento14 pagineIDDSI Framework Testing Methods 2.0 - 2019MayraNessuna valutazione finora
- Stuttering TherapyDocumento154 pagineStuttering Therapymechbull11100% (1)
- F S D G S: Eeding and Wallowing Ysfunction IN Enetic YndromesDocumento11 pagineF S D G S: Eeding and Wallowing Ysfunction IN Enetic YndromespaulaNessuna valutazione finora
- Witwer ST Developmental MilestonesDocumento2 pagineWitwer ST Developmental MilestonesErsya Muslih100% (1)
- Speech Therapy For Language-Based Learning DisabilitiesDocumento2 pagineSpeech Therapy For Language-Based Learning DisabilitiesBrainNessuna valutazione finora
- Clinical Guideline Stuttering-1Documento170 pagineClinical Guideline Stuttering-1Vaida MadalinaNessuna valutazione finora
- Miccio4s PDFDocumento7 pagineMiccio4s PDFMaria Patrixia AquinoNessuna valutazione finora
- Noun Derivation in LutirikiDocumento74 pagineNoun Derivation in LutirikiBryan Birama0% (1)
- Lamp Words For LifeDocumento3 pagineLamp Words For Lifeapi-400249453Nessuna valutazione finora
- Speech PathologistDocumento13 pagineSpeech PathologistFpj TarrobalNessuna valutazione finora
- Hanen Tips EnglishDocumento6 pagineHanen Tips EnglishGökçe Gökçümen KocaNessuna valutazione finora
- Speech & Language Therapy in Practice, Summer 2008Documento32 pagineSpeech & Language Therapy in Practice, Summer 2008Speech & Language Therapy in PracticeNessuna valutazione finora
- Handy Handouts: Hellos and Goodbyes - Teaching Children To Use GreetingsDocumento2 pagineHandy Handouts: Hellos and Goodbyes - Teaching Children To Use GreetingsIris PopescuNessuna valutazione finora
- Evidence+Based+Practices+for+Early+R+Therapy Full+Handout Lindsey+HockelDocumento45 pagineEvidence+Based+Practices+for+Early+R+Therapy Full+Handout Lindsey+HockelNoha Ibraheem Helmy100% (1)
- Fluency ShapingDocumento83 pagineFluency ShapingAltaf HasenNessuna valutazione finora
- Understanding Childhood Apraxia: Super Duper Handy Handouts!Documento3 pagineUnderstanding Childhood Apraxia: Super Duper Handy Handouts!Staci NeustadtNessuna valutazione finora
- Speech and Language StudiesDocumento17 pagineSpeech and Language StudiesafrawrrNessuna valutazione finora
- Entertainment AidsDocumento50 pagineEntertainment Aidsapi-304407528100% (2)
- Apraxia TXDocumento20 pagineApraxia TXadriricaldeNessuna valutazione finora
- WritingActivities 0 PDFDocumento15 pagineWritingActivities 0 PDFLouise Marie LicudineNessuna valutazione finora
- What Works SLT Interventions For SLCNDocumento170 pagineWhat Works SLT Interventions For SLCNlionella12Nessuna valutazione finora
- Cognitive Development of Young ChildrenDocumento6 pagineCognitive Development of Young ChildrenFloyd SeremNessuna valutazione finora
- A Guide For Parents and Caregivers of Toddlers 12-36 MonthsDocumento24 pagineA Guide For Parents and Caregivers of Toddlers 12-36 MonthsreenupNessuna valutazione finora
- 161 Basic ConceptsDocumento3 pagine161 Basic Conceptsilham ilahiNessuna valutazione finora
- Concepts in Occupational Therapy in Relation To The ICFDocumento16 pagineConcepts in Occupational Therapy in Relation To The ICFmarjan 01Nessuna valutazione finora
- Autism and LenguageDocumento13 pagineAutism and LenguageSergio Andres Villegas VillaNessuna valutazione finora
- Speech & Language Therapy in Practice, Autumn 1999Documento32 pagineSpeech & Language Therapy in Practice, Autumn 1999Speech & Language Therapy in PracticeNessuna valutazione finora
- Stop Think DoDocumento3 pagineStop Think Doapi-254018114Nessuna valutazione finora
- Speech & Language Therapy in Practice, Spring 2009Documento32 pagineSpeech & Language Therapy in Practice, Spring 2009Speech & Language Therapy in PracticeNessuna valutazione finora
- Communication Choice Board BundleDocumento5 pagineCommunication Choice Board BundleMadhu sudarshan ReddyNessuna valutazione finora
- Cluttering and Stuttering EbookDocumento2 pagineCluttering and Stuttering EbookPrakash ThakurNessuna valutazione finora
- Autism Handwriting SkillsDocumento8 pagineAutism Handwriting SkillsStephen GreenNessuna valutazione finora
- 01 WholeDocumento430 pagine01 WholeChi NguyenNessuna valutazione finora
- CamperdownDocumento10 pagineCamperdownPREMITHANessuna valutazione finora
- Adductor Spasmodic Dysphonia: A Case For Speech and Language TherapyDocumento3 pagineAdductor Spasmodic Dysphonia: A Case For Speech and Language TherapySpeech & Language Therapy in PracticeNessuna valutazione finora
- Speech Final SummariesDocumento50 pagineSpeech Final SummariesZoe king100% (1)
- Family Board Game Rules: One Time SetupDocumento12 pagineFamily Board Game Rules: One Time SetupFerdi GulNessuna valutazione finora
- Toilet Story1 PDFDocumento9 pagineToilet Story1 PDFImaa SyakiraNessuna valutazione finora
- Living with Hearing Difficulties: The process of enablementDa EverandLiving with Hearing Difficulties: The process of enablementNessuna valutazione finora
- Winning Ways (Winter 2007)Documento1 paginaWinning Ways (Winter 2007)Speech & Language Therapy in PracticeNessuna valutazione finora
- Winning Ways (Spring 2008)Documento1 paginaWinning Ways (Spring 2008)Speech & Language Therapy in PracticeNessuna valutazione finora
- Turning On The SpotlightDocumento6 pagineTurning On The SpotlightSpeech & Language Therapy in PracticeNessuna valutazione finora
- In Brief and Critical Friends (Summer 09)Documento1 paginaIn Brief and Critical Friends (Summer 09)Speech & Language Therapy in PracticeNessuna valutazione finora
- Winning Ways (Autumn 2008)Documento1 paginaWinning Ways (Autumn 2008)Speech & Language Therapy in PracticeNessuna valutazione finora
- Here's One I Made Earlier (Spring 2008)Documento1 paginaHere's One I Made Earlier (Spring 2008)Speech & Language Therapy in PracticeNessuna valutazione finora
- In Brief (Summer 10) TeenagersDocumento1 paginaIn Brief (Summer 10) TeenagersSpeech & Language Therapy in PracticeNessuna valutazione finora
- Winning Ways (Summer 2008)Documento1 paginaWinning Ways (Summer 2008)Speech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Spring 10 Dating ThemeDocumento1 paginaHere's One Spring 10 Dating ThemeSpeech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Summer 10Documento1 paginaHere's One Summer 10Speech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Sum 09 Storyteller, Friendship, That's HowDocumento1 paginaHere's One Sum 09 Storyteller, Friendship, That's HowSpeech & Language Therapy in PracticeNessuna valutazione finora
- In Brief (Autumn 09) NQTs and Assessment ClinicsDocumento1 paginaIn Brief (Autumn 09) NQTs and Assessment ClinicsSpeech & Language Therapy in PracticeNessuna valutazione finora
- In Brief (Summer 11) AphasiaDocumento1 paginaIn Brief (Summer 11) AphasiaSpeech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Spring 11Documento1 paginaHere's One Spring 11Speech & Language Therapy in PracticeNessuna valutazione finora
- In Brief and Here's One Autumn 10Documento2 pagineIn Brief and Here's One Autumn 10Speech & Language Therapy in PracticeNessuna valutazione finora
- Here's One I Made Earlier Summer 11Documento1 paginaHere's One I Made Earlier Summer 11Speech & Language Therapy in PracticeNessuna valutazione finora
- In Brief (Winter 10) Stammering and Communication Therapy InternationalDocumento2 pagineIn Brief (Winter 10) Stammering and Communication Therapy InternationalSpeech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Winter 11Documento1 paginaHere's One Winter 11Speech & Language Therapy in PracticeNessuna valutazione finora
- Here's One Winter 10Documento1 paginaHere's One Winter 10Speech & Language Therapy in PracticeNessuna valutazione finora
- In Brief... : Supporting Communication With Signed SpeechDocumento1 paginaIn Brief... : Supporting Communication With Signed SpeechSpeech & Language Therapy in PracticeNessuna valutazione finora
- In Brief Winter 11Documento2 pagineIn Brief Winter 11Speech & Language Therapy in PracticeNessuna valutazione finora
- My Top Resources (Winter 11) Clinical PlacementsDocumento1 paginaMy Top Resources (Winter 11) Clinical PlacementsSpeech & Language Therapy in PracticeNessuna valutazione finora
- New Pathways: Lynsey PatersonDocumento3 pagineNew Pathways: Lynsey PatersonSpeech & Language Therapy in PracticeNessuna valutazione finora
- Applying Choices and PossibilitiesDocumento3 pagineApplying Choices and PossibilitiesSpeech & Language Therapy in PracticeNessuna valutazione finora
- Understanding RhysDocumento3 pagineUnderstanding RhysSpeech & Language Therapy in PracticeNessuna valutazione finora
- Here's One I Made EarlierDocumento1 paginaHere's One I Made EarlierSpeech & Language Therapy in PracticeNessuna valutazione finora
- sWALLOWING iNTERVENTION MCNEIL TERAPYDocumento28 paginesWALLOWING iNTERVENTION MCNEIL TERAPYAngelica Maria LizarazoNessuna valutazione finora
- Tubular AerobicsDocumento7 pagineTubular AerobicsDee MonkNessuna valutazione finora
- Tongue (Anatomy) : See AlsoDocumento1 paginaTongue (Anatomy) : See AlsoSelenia025Nessuna valutazione finora
- 10.EffectofOrofacial JournalDocumento5 pagine10.EffectofOrofacial JournalJuliza Tatiana Suárez PatarroyoNessuna valutazione finora
- Digestive System Design Study GuideDocumento3 pagineDigestive System Design Study Guideapi-390361165Nessuna valutazione finora
- What Are Swallowing DisordersDocumento4 pagineWhat Are Swallowing DisordersNs AifNessuna valutazione finora
- Physiology of MastigationDocumento3 paginePhysiology of MastigationAlya Putri KhairaniNessuna valutazione finora
- Anatomy of Stomatognathic SystemDocumento144 pagineAnatomy of Stomatognathic SystemSwati SawalNessuna valutazione finora
- VASES Scoring Sheet - May 2022Documento16 pagineVASES Scoring Sheet - May 2022FERNANDA CAROLINA JARANessuna valutazione finora
- Pemicu 1 DessyDocumento184 paginePemicu 1 DessyDessy DsyNessuna valutazione finora
- Physiology of LarynxDocumento115 paginePhysiology of LarynxKashish HatukaNessuna valutazione finora
- Neurophysiology of Swallowing - Ertekin - 2003 PDFDocumento19 pagineNeurophysiology of Swallowing - Ertekin - 2003 PDFMaca Cerda DonosoNessuna valutazione finora
- 1 - Case Disfagia DisfoniaDocumento41 pagine1 - Case Disfagia DisfoniaMegan ShanzuNessuna valutazione finora
- Use of The ICF in Dysphagia ManagementDocumento11 pagineUse of The ICF in Dysphagia Managementlinm@kilvington.vic.edu.auNessuna valutazione finora
- Speech & Language Therapy in Practice, Autumn 1998Documento32 pagineSpeech & Language Therapy in Practice, Autumn 1998Speech & Language Therapy in PracticeNessuna valutazione finora
- Evaluation of Feeding, Eating, and Swallowing For Children With Cerebral PalsyDocumento9 pagineEvaluation of Feeding, Eating, and Swallowing For Children With Cerebral Palsyanner.socialsNessuna valutazione finora
- 2020 CPT® Codes For Speech-Language PathologyDocumento2 pagine2020 CPT® Codes For Speech-Language PathologyAllie BenoitNessuna valutazione finora
- ENT RadiologiDocumento70 pagineENT RadiologiyowwwNessuna valutazione finora
- Dysphagia From A Neurogeriatric Point of ViewDocumento6 pagineDysphagia From A Neurogeriatric Point of ViewVanessaCarrilloNessuna valutazione finora
- Lecture 4 5 - Fluid and Nutrition III IVDocumento117 pagineLecture 4 5 - Fluid and Nutrition III IVjimmy jimmyNessuna valutazione finora
- H & N - Pharynx& Deglutition PDFDocumento17 pagineH & N - Pharynx& Deglutition PDFRamin AmirkhiziNessuna valutazione finora
- 2 NCP Impaired Swallowing EditedDocumento4 pagine2 NCP Impaired Swallowing EditedLeonardo Montemayor100% (3)
- CHAPTER 9 Gastrointestinal SystemDocumento7 pagineCHAPTER 9 Gastrointestinal SystemGilianne Balatbat ManuelNessuna valutazione finora
- 2007 CASLPA Position Paper On Dysphagia in AdultsDocumento8 pagine2007 CASLPA Position Paper On Dysphagia in AdultsEva Sala RenauNessuna valutazione finora