Potrebbero piacerti anche
- NGT Feeding: by Group 2Documento25 pagineNGT Feeding: by Group 2karl montano100% (1)
- Care PlanDocumento4 pagineCare PlangopscharanNessuna valutazione finora
- Nursing Care of The Child With Congenital Heart DiseaseDocumento5 pagineNursing Care of The Child With Congenital Heart DiseaseAisyahKautsarIlmiNessuna valutazione finora
- Introduction in Nursing Research: Prepared By, Mrs Arjita Associate ProfesorDocumento22 pagineIntroduction in Nursing Research: Prepared By, Mrs Arjita Associate Profesorsivaspb5Nessuna valutazione finora
- Pa Tho Physiology PrintDocumento4 paginePa Tho Physiology Printaiconjucea0% (1)
- Nursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedDocumento25 pagineNursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedJrose CuerpoNessuna valutazione finora
- Retinopathy of PrematurityDocumento15 pagineRetinopathy of Prematuritymarissa ulkhairNessuna valutazione finora
- DDSTDocumento61 pagineDDSTji payNessuna valutazione finora
- NCP NecDocumento1 paginaNCP NecandikaisnaeniNessuna valutazione finora
- Glaucoma Guide: Causes, Types, Symptoms & TreatmentDocumento10 pagineGlaucoma Guide: Causes, Types, Symptoms & TreatmentIzza Mae Ferrancol PastranaNessuna valutazione finora
- Public Health Nursing in SchoolsDocumento45 paginePublic Health Nursing in SchoolsdaveNessuna valutazione finora
- Mechanisms Case StudyDocumento13 pagineMechanisms Case Studyshane_tin143Nessuna valutazione finora
- Measles case study with Koplik's spots and rubeola virusDocumento3 pagineMeasles case study with Koplik's spots and rubeola virusApex Torres0% (1)
- Administering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESDocumento14 pagineAdministering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESPb0% (1)
- ITP (Idiopathic Thrombocytopenic Purpura)Documento20 pagineITP (Idiopathic Thrombocytopenic Purpura)Iqra NaseemNessuna valutazione finora
- ASD Pathophysiology, Signs, Symptoms, and TreatmentDocumento1 paginaASD Pathophysiology, Signs, Symptoms, and TreatmentMSNessuna valutazione finora
- Acute & Chronic PancreatitisDocumento40 pagineAcute & Chronic PancreatitisDelvina GashiNessuna valutazione finora
- Oesophageal Atresia by GabriellaDocumento7 pagineOesophageal Atresia by GabriellaGabrielleNessuna valutazione finora
- Hydrocephalus Nursing CareDocumento27 pagineHydrocephalus Nursing CareyounggirldavidNessuna valutazione finora
- PATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalDocumento11 paginePATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalSelwynVillamorPatenteNessuna valutazione finora
- Live Preterm Baby Delivered NSDDocumento13 pagineLive Preterm Baby Delivered NSDKristine Anne SorianoNessuna valutazione finora
- Case Study-Infant With Fluid Imbalance08-10-KEYDocumento3 pagineCase Study-Infant With Fluid Imbalance08-10-KEYreecoleNessuna valutazione finora
- Laguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeDocumento4 pagineLaguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeKristine Louise JavierNessuna valutazione finora
- Blood Pressure MeasurementDocumento2 pagineBlood Pressure MeasurementMaryHope100% (1)
- Cast CareDocumento1 paginaCast CareCarmelita SaltNessuna valutazione finora
- Nursing Care PlanDocumento8 pagineNursing Care PlanVincent QuitorianoNessuna valutazione finora
- Nursing Care Plans - NurseryDocumento4 pagineNursing Care Plans - NurserySusie PadaoanNessuna valutazione finora
- Urine Specimen CollectionDocumento3 pagineUrine Specimen Collectionyota_ahlyNessuna valutazione finora
- Case Presentation HydrocephalusDocumento48 pagineCase Presentation HydrocephalusSu Osman50% (2)
- Nursing ResearchDocumento5 pagineNursing ResearchGerald GarciaNessuna valutazione finora
- Case-Study-Final-1 BOSET NA CASE PRESENTATIONDocumento57 pagineCase-Study-Final-1 BOSET NA CASE PRESENTATIONGiselle EstoquiaNessuna valutazione finora
- National Anaemia Prophylaxis Programme Reduces Maternal MortalityDocumento15 pagineNational Anaemia Prophylaxis Programme Reduces Maternal MortalityAnkit TalujaNessuna valutazione finora
- PUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIADocumento10 paginePUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIAJulienne PucanNessuna valutazione finora
- Asphyxia NeonatorumDocumento29 pagineAsphyxia Neonatorummamaalyssa100% (1)
- Gastroschisis & OmphaloceleDocumento1 paginaGastroschisis & OmphaloceleMaecy PasionNessuna valutazione finora
- A Client Care StudyDocumento27 pagineA Client Care StudyTestimony WilliamNessuna valutazione finora
- Gastric Gavage OR Enteral: Naso/Orogastric Gastrostomy: Mrs .Jenifer Kaliso TutorDocumento39 pagineGastric Gavage OR Enteral: Naso/Orogastric Gastrostomy: Mrs .Jenifer Kaliso TutorSharon LawrenceNessuna valutazione finora
- Urine Specimen Collection Procedure PDFDocumento3 pagineUrine Specimen Collection Procedure PDFtincho9Nessuna valutazione finora
- Lumbar Puncture ReportDocumento5 pagineLumbar Puncture ReportTweenie DalumpinesNessuna valutazione finora
- Growth and Development of Newborn To InfancyDocumento54 pagineGrowth and Development of Newborn To Infancymerin sunilNessuna valutazione finora
- Kardex, Drug Study and CheckDocumento12 pagineKardex, Drug Study and CheckJemina Rafanan RacadioNessuna valutazione finora
- Terminologies Used in Nursing Education 1Documento11 pagineTerminologies Used in Nursing Education 1ramita sahNessuna valutazione finora
- Abbreviations For Nursing StudentsDocumento7 pagineAbbreviations For Nursing StudentssodiwoNessuna valutazione finora
- Neonatal Sepsis LectureDocumento142 pagineNeonatal Sepsis Lectureokwadha simion0% (1)
- Urine Albumin Test Detects Pregnancy RiskDocumento7 pagineUrine Albumin Test Detects Pregnancy RiskKaren Jae Grant CabrillosNessuna valutazione finora
- Assessment of Digestive and Gi FunctionDocumento3 pagineAssessment of Digestive and Gi FunctionEmi EspinoNessuna valutazione finora
- Case Study 1 - PneumoniaDocumento14 pagineCase Study 1 - PneumoniaJilkiah Mae Alfoja CampomanesNessuna valutazione finora
- Anatomy &physiology JaundiceDocumento2 pagineAnatomy &physiology JaundiceHCX dghhqNessuna valutazione finora
- Nursing Diagnosis For AppendicitisDocumento1 paginaNursing Diagnosis For AppendicitisTweenie DalumpinesNessuna valutazione finora
- Chemotherapy EssayDocumento2 pagineChemotherapy EssaySakina S. MoosaNessuna valutazione finora
- Manage Preterm Labor with Bed Rest and TocolysisDocumento4 pagineManage Preterm Labor with Bed Rest and TocolysisYeni PuspitaNessuna valutazione finora
- Assessing Newborns EffectivelyDocumento35 pagineAssessing Newborns EffectivelyBaldwin Hamzcorp Hamoonga100% (1)
- Introduction To Nursing ResearchDocumento17 pagineIntroduction To Nursing ResearchYounas BhattiNessuna valutazione finora
- Significance of Nursing ResearchDocumento22 pagineSignificance of Nursing ResearchPrincess Ivan Gayagoy100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- Naso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringDocumento12 pagineNaso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringmeisygraniaNessuna valutazione finora
- Nasogastric Tube ChildrenDocumento3 pagineNasogastric Tube ChildrenYwagar YwagarNessuna valutazione finora
- Testing Placement of Nasogastric Tubes in Infants & ChildrenDocumento4 pagineTesting Placement of Nasogastric Tubes in Infants & ChildrenYwagar YwagarNessuna valutazione finora
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocumento14 pagineClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarNessuna valutazione finora
- Sydney 2008 MarchDocumento8 pagineSydney 2008 MarchYwagar YwagarNessuna valutazione finora
- Walhalla Gold MineDocumento1 paginaWalhalla Gold MineYwagar YwagarNessuna valutazione finora
- Brisbane July 2008 RecallDocumento11 pagineBrisbane July 2008 RecallYwagar YwagarNessuna valutazione finora
- Gold Coast 2008Documento1 paginaGold Coast 2008Ywagar YwagarNessuna valutazione finora
- GPDocumento3 pagineGPYwagar YwagarNessuna valutazione finora
- Recall Brisbane February 2008Documento7 pagineRecall Brisbane February 2008Ywagar YwagarNessuna valutazione finora
- Draft May 08 WES ProgramDocumento2 pagineDraft May 08 WES ProgramYwagar YwagarNessuna valutazione finora
- Adel 2Documento24 pagineAdel 2Ywagar YwagarNessuna valutazione finora
- Adelaide 13th September 2008Documento16 pagineAdelaide 13th September 2008Ywagar YwagarNessuna valutazione finora
- AMC Clinical Exam Recall 8 Sep 2008 Melbourne Retest 1Documento7 pagineAMC Clinical Exam Recall 8 Sep 2008 Melbourne Retest 1Ywagar YwagarNessuna valutazione finora
- Adelaide, 5 April, 2008: PaediatricsDocumento17 pagineAdelaide, 5 April, 2008: PaediatricsYwagar YwagarNessuna valutazione finora
- Adelaide April 2008Documento16 pagineAdelaide April 2008Ywagar YwagarNessuna valutazione finora
- Dr CAI clinical cases under 40 charsDocumento31 pagineDr CAI clinical cases under 40 charsYwagar Ywagar100% (1)
- Adelaide 13th September 2008Documento16 pagineAdelaide 13th September 2008Ywagar YwagarNessuna valutazione finora
- Adelaide 13th September 2008Documento16 pagineAdelaide 13th September 2008Ywagar YwagarNessuna valutazione finora
- Melb RetestDocumento2 pagineMelb RetestYwagar YwagarNessuna valutazione finora
- 9 August 08 Melbourne Clinical Exam RecallDocumento6 pagine9 August 08 Melbourne Clinical Exam RecallYwagar YwagarNessuna valutazione finora
- Melb RetestDocumento6 pagineMelb RetestYwagar YwagarNessuna valutazione finora
- Melbourne 2008 Nov 8Documento10 pagineMelbourne 2008 Nov 8Ywagar YwagarNessuna valutazione finora
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocumento14 pagineClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarNessuna valutazione finora
- Brisbane, 11th October 2008Documento6 pagineBrisbane, 11th October 2008Ywagar YwagarNessuna valutazione finora
- To ReviseAug 22 AdelaideDocumento4 pagineTo ReviseAug 22 AdelaideYwagar YwagarNessuna valutazione finora
- ACln2007!09!08MEL Retest Wd97Documento6 pagineACln2007!09!08MEL Retest Wd97Ywagar YwagarNessuna valutazione finora
- MelbDocumento9 pagineMelbYwagar YwagarNessuna valutazione finora
- Paediatrics:: Case 1nsionDocumento16 paginePaediatrics:: Case 1nsionYwagar YwagarNessuna valutazione finora
- BrisDocumento9 pagineBrisYwagar YwagarNessuna valutazione finora
- Melb RetestDocumento4 pagineMelb RetestYwagar YwagarNessuna valutazione finora
- Brisbane, 11th October 2008Documento6 pagineBrisbane, 11th October 2008Ywagar YwagarNessuna valutazione finora
- Syd 1Documento11 pagineSyd 1Ywagar YwagarNessuna valutazione finora
- Health Plan Financials ExplainedDocumento467 pagineHealth Plan Financials Explainedvidya71v100% (1)
- Constructing Temporary Access Road for Geothermal PlantDocumento3 pagineConstructing Temporary Access Road for Geothermal PlantGad100% (6)
- Hayrax Con Mascara Facial PDFDocumento8 pagineHayrax Con Mascara Facial PDFSantos LopNessuna valutazione finora
- Koding A & ZDocumento55 pagineKoding A & ZtofikNessuna valutazione finora
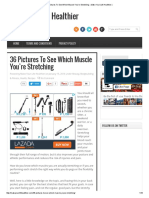
- 36 Pictures To See Which Muscle You'Re Stretching Make Your Life HealthierDocumento14 pagine36 Pictures To See Which Muscle You'Re Stretching Make Your Life HealthierGlenn Paul GalanoNessuna valutazione finora
- MSRT 0003Documento3 pagineMSRT 0003api-336525339Nessuna valutazione finora
- Pemanfaatan Drum Bekas Menjadi TangkiDocumento17 paginePemanfaatan Drum Bekas Menjadi TangkiChristina Mediana Cindy KhairaniNessuna valutazione finora
- Hyogo Framework of ActionDocumento90 pagineHyogo Framework of ActionDipendraGautamNessuna valutazione finora
- Parson Executive Order 21-10Documento1 paginaParson Executive Order 21-10KevinSeanHeldNessuna valutazione finora
- Program DescriptionDocumento17 pagineProgram DescriptionNichole KilbournNessuna valutazione finora
- NANDA DAFFA PRASETYAWAN Fix DirDocumento2 pagineNANDA DAFFA PRASETYAWAN Fix Dirbeauty asriNessuna valutazione finora
- Cetirizine 2Documento2 pagineCetirizine 2ianNessuna valutazione finora
- Pamaskong Handog NG Mga Inhenyero': Sacrificing The Christmas PartyDocumento4 paginePamaskong Handog NG Mga Inhenyero': Sacrificing The Christmas PartyJoeniferLecomisMontebonNessuna valutazione finora
- Toronto Public Health Absenteeism Notification LetterDocumento2 pagineToronto Public Health Absenteeism Notification LetterToronto StarNessuna valutazione finora
- Coursera Drug Developement PDFDocumento1 paginaCoursera Drug Developement PDFVasilis TsinterisNessuna valutazione finora
- IAEA SSR-3 - Safety of Research ReactorsDocumento152 pagineIAEA SSR-3 - Safety of Research Reactorsmadalina_troneaNessuna valutazione finora
- The Citizen's Body - Pamela GilbertDocumento202 pagineThe Citizen's Body - Pamela GilbertConor HeffernanNessuna valutazione finora
- Botulinum Toxin SeminarDocumento18 pagineBotulinum Toxin SeminarPreeyah ArasuNessuna valutazione finora
- EPB 261 - Chemical Use and Storage at WaterworksDocumento3 pagineEPB 261 - Chemical Use and Storage at WaterworksKONSTANTINOS TOMAZISNessuna valutazione finora
- Dataguise WP Why Add Masking PDFDocumento8 pagineDataguise WP Why Add Masking PDFdubillasNessuna valutazione finora
- Alteration of blood coagulation in CKD patients on dialysisDocumento26 pagineAlteration of blood coagulation in CKD patients on dialysissubankar NagNessuna valutazione finora
- Does Obesity Cause Type 2 Diabetes MellitusDocumento5 pagineDoes Obesity Cause Type 2 Diabetes Mellitusthebrotherhood2014Nessuna valutazione finora
- Tax Organizer ShortDocumento28 pagineTax Organizer ShortExactCPANessuna valutazione finora
- Dammam Logistic Center - HSE PlanDocumento143 pagineDammam Logistic Center - HSE PlanShah Muzzamil100% (1)
- IMer C Research CompetitionDocumento1 paginaIMer C Research CompetitiongabbynengNessuna valutazione finora
- Icd 10 Official WHO Updates Combined 1996-2010VOLUME-3Documento261 pagineIcd 10 Official WHO Updates Combined 1996-2010VOLUME-3nastitianNessuna valutazione finora
- I Am Sharing Research With YouDocumento10 pagineI Am Sharing Research With Youmikee albaNessuna valutazione finora
- Or Benchmarks CollaborativeDocumento18 pagineOr Benchmarks CollaborativeMcKesson Surgical SolutionsNessuna valutazione finora
- Bioavailability and BioequivalenceDocumento6 pagineBioavailability and BioequivalenceDharmesh PatelNessuna valutazione finora
- Drinking Water - Is 10500-1991 PDFDocumento3 pagineDrinking Water - Is 10500-1991 PDFearthanskyfriends100% (1)